efecto antihipertensivo de la amlodipina 48 a 72 hs despues del ...
efecto antihipertensivo de la amlodipina 48 a 72 hs despues del ...
efecto antihipertensivo de la amlodipina 48 a 72 hs despues del ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
96<br />
85<br />
nd<br />
on<br />
he<br />
10;<br />
in<br />
89;<br />
ian<br />
tile<br />
'87;<br />
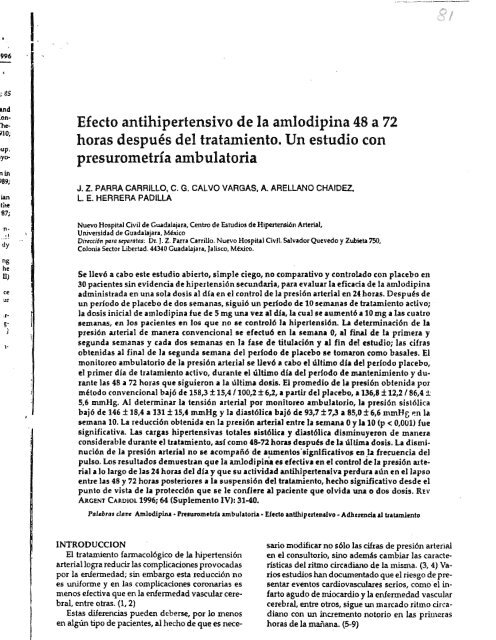
Efecto <strong>antihipertensivo</strong> <strong>de</strong> <strong>la</strong> <strong>amlodipina</strong> <strong>48</strong> a <strong>72</strong><br />
horas <strong>de</strong>spués <strong>de</strong>l tratamiento. Un estudio con<br />
presurometría ambu<strong>la</strong>toria<br />
J. Z. PARRA CARRILLO, C. G. CALVO VARGAS, A. ARELLANO CHAIDEZ.<br />
L E. HERRERA PADILLA<br />
Nuevo Hospital Civil <strong>de</strong> Gtada<strong>la</strong>jara, Centro <strong>de</strong> Estudios <strong>de</strong> Hipertensión Arterial,<br />
'n <br />
.1<br />
Universidad <strong>de</strong> Guada<strong>la</strong>jara, México<br />
Dirtcci6npara separatlls: Dr. J. Z. fArra Carrillo. Nuevo Hospital Civil. Salvador Quevedo y Zubieta750,<br />
dy<br />
Colonia Sector Libertad. 44340 Guada<strong>la</strong>jara, Jalisco. México.<br />
ng<br />
he<br />
D)<br />
ce<br />
ur<br />
Se llevó a cabo este estudio abierto, simple ciego, no comparativo y contro<strong>la</strong>do con p<strong>la</strong>cebo en<br />
30 pacientes sin evi<strong>de</strong>ncia <strong>de</strong> hipertensión secundaria, para evaluar <strong>la</strong> eficacia <strong>de</strong> <strong>la</strong> <strong>amlodipina</strong><br />
administrada en una so<strong>la</strong> dosis al día en el control <strong>de</strong> <strong>la</strong> presión arterial en 24horas. Después <strong>de</strong><br />
un período <strong>de</strong> p<strong>la</strong>cebo <strong>de</strong> dos semanas, siguió un periodo <strong>de</strong> 10 semanas <strong>de</strong> tratamiento activo; ,<br />
<strong>la</strong> dosis inicial <strong>de</strong> <strong>amlodipina</strong> fue <strong>de</strong> 5 mg una vez al día, La cual se aumentó a 10 mg a <strong>la</strong>s cuatro<br />
.rs<br />
semanas, en los pacientes en los que no se controló <strong>la</strong> hipertensión. u <strong>de</strong>terminación <strong>de</strong> <strong>la</strong><br />
) presión arterial <strong>de</strong> manera convencional se efectuó en <strong>la</strong> semana O, al final <strong>de</strong> <strong>la</strong> primera y<br />
segunda semanas y cada dos semanas en <strong>la</strong> fase <strong>de</strong> titu<strong>la</strong>ción y al fin <strong>de</strong>! estudio; <strong>la</strong>s cifras<br />
l-<br />
obtenidas al final <strong>de</strong> <strong>la</strong> segunda semana <strong>de</strong>l periodo <strong>de</strong> p<strong>la</strong>cebo se tomaron como basales. El<br />
monitoreo ambu<strong>la</strong>torio <strong>de</strong> <strong>la</strong> presión arterial se llevó a cabo el último día <strong>de</strong>l período p<strong>la</strong>cebo,<br />
el primer día <strong>de</strong> tratamiento activo, durante el último día <strong>de</strong>l período <strong>de</strong> mantenimiento y durante<br />
<strong>la</strong>s <strong>48</strong> a <strong>72</strong> horas que siguieron a <strong>la</strong> última dosis. El promedio <strong>de</strong> <strong>la</strong> presión obtenida por<br />
método convencional bajó <strong>de</strong> 158,3±15,4/100,2±6,2, a partir <strong>de</strong>l p<strong>la</strong>cebo, a 136,8±12,2/86,4 ±<br />
5,6 mmHg. Al <strong>de</strong>terminar La tensión arterial por monítoreo ambu<strong>la</strong>torio, <strong>la</strong> presión sistólica<br />
bajó <strong>de</strong> 146 ± 18,4 a 131 ± 15,4 mmHg y <strong>la</strong> diastólica bajó <strong>de</strong> 93,7 ± 7,3 a 85,0± 6,6 mmBE; en <strong>la</strong><br />
semana 10. La reducción obtenida en <strong>la</strong> presión arterial entre <strong>la</strong> semana Oy <strong>la</strong> 10 (p < 0,001) fue<br />
significativa. Las cargas hipertensivas totales sistólica y diast6lic
32<br />
REVISTA ARGENTINA DE CARDIOLOGlA, VOL 64, SUPLEMENTO IV 1996<br />
AM<br />
El USO <strong>de</strong> unida<strong>de</strong>s <strong>de</strong> monitoreo ambu<strong>la</strong>torio no<br />
ínvasívo (PAANI) ha permitido registrar el ritmo círcadiano<br />
<strong>de</strong> <strong>la</strong> presión arterial (PA) sin gran<strong>de</strong>s dííículta<strong>de</strong>s<br />
ni riesgos para los pacientes. (10, 11) TIenen<br />
una corre<strong>la</strong>ción alta con <strong>la</strong> medición intraarteriaJ<br />
(r. 0,81), permiten estudiar al sujeto <strong>de</strong>ntro <strong>de</strong><br />
<strong>la</strong> mayor parte <strong>de</strong> sus activida<strong>de</strong>s normales con excepción<br />
<strong>de</strong>l ejercicio, evitan <strong>la</strong>hipertensión <strong>de</strong> ,.guardapolvo<br />
b<strong>la</strong>nco", el <strong>efecto</strong> p<strong>la</strong>cebo y evalúan mucho<br />
mejor el <strong>efecto</strong> <strong>de</strong> los medicamentos <strong>antihipertensivo</strong>s.<br />
(10-14)<br />
Gradas a <strong>la</strong> disponibilidad <strong>de</strong> unida<strong>de</strong>s <strong>de</strong> monitoreo<br />
para PAANI y <strong>de</strong> los hal<strong>la</strong>zgos <strong>de</strong>scriptos en<br />
re<strong>la</strong>ción con el daño producido durante ciertas horas<br />
cruciales, <strong>la</strong> variabilidad <strong>de</strong> <strong>la</strong> PA, así como <strong>la</strong><br />
carga total hipertensiva y el estudio <strong>de</strong>l <strong>efecto</strong> <strong>de</strong> los<br />
medicamentos <strong>antihipertensivo</strong>s durante <strong>la</strong>s 24horas<br />
<strong>de</strong> <strong>la</strong> vida <strong>de</strong> un paciente hipertenso se han convertido<br />
en aspectos primordiales <strong>de</strong> <strong>la</strong> investigación<br />
cardiovascu<strong>la</strong>r, (15,16)<br />
La amlodipína es un nuevo bloqueante <strong>de</strong> los canales<br />
<strong>de</strong> calcio que pertenece al grupo <strong>de</strong> <strong>la</strong>s díhidropiridinas;<br />
se ha <strong>de</strong>mostrado que es efectiva y segura<br />
para disminuir <strong>la</strong>s cifras <strong>de</strong> PA evaluada por<br />
técnicas convencionales. Existen algunos estudios<br />
que <strong>de</strong>muestran este <strong>efecto</strong> durante <strong>la</strong>s 24 horas. (17<br />
20) Sin embargo todavía existen algunos interrogantes<br />
que es necesario contestar.<br />
El primero <strong>de</strong> ellos es <strong>de</strong>terminar si su <strong>efecto</strong> <strong>antihipertensivo</strong><br />
ocurre durante <strong>la</strong>s 24horas <strong>de</strong>l día en<br />
<strong>la</strong>s diferentes pob<strong>la</strong>ciones y si esta disminución <strong>de</strong><br />
<strong>la</strong> PA es efectiva durante el día y persiste durante <strong>la</strong><br />
noche.<br />
Por otra parte, es muy importante conocer si <strong>la</strong><br />
dosis administrada una vez al día, por <strong>la</strong> mañana,<br />
es capaz <strong>de</strong> reducir el pico matutino <strong>de</strong> <strong>la</strong> PA Y<strong>la</strong><br />
carga total hipertensiva <strong>de</strong> los pacientes, así como<br />
disminuir <strong>la</strong> variabilidad diaria <strong>de</strong> <strong>la</strong> PA. (4, 21-24)<br />
En algunos estudios se ha <strong>de</strong>terminado que <strong>la</strong><br />
<strong>amlodipina</strong> tiene <strong>efecto</strong> <strong>antihipertensivo</strong> sostenido<br />
hasta <strong>48</strong> horas <strong>de</strong>spués <strong>de</strong> <strong>la</strong> última dosis, con una<br />
marcada reducción <strong>de</strong> <strong>la</strong> variabilidad <strong>de</strong> <strong>la</strong> PA. (25)<br />
Sin embargo, este <strong>efecto</strong>, que podrfa ser <strong>de</strong> gran utilidad<br />
para reducir el posible daño a órganos b<strong>la</strong>nco,<br />
así como para proteger al paciente con un cumplimiento<br />
irregu<strong>la</strong>r <strong>de</strong>l tratamiento, no ha sido corroborado<br />
con técnicas que incluyan el monitoreo ambu<strong>la</strong>torio<br />
<strong>de</strong> 24 horas. (22)<br />
Objetivo .<br />
El objetivo <strong>de</strong> este estudio fue confirmar <strong>la</strong> eficacia<br />
antihipertensiva <strong>de</strong> <strong>la</strong> <strong>amlodipina</strong> durante<br />
<strong>la</strong>s 24 horas tomando una dosis al día, usando monitoreo<br />
ambu<strong>la</strong>torio <strong>de</strong> <strong>la</strong> presión arterial (MAPA).<br />
Espedficamente se <strong>de</strong>terminó el <strong>efecto</strong> <strong>de</strong> <strong>la</strong> <strong>amlodipina</strong><br />
en <strong>la</strong> carga total hipertensiva, el <strong>efecto</strong> <strong>de</strong><br />
una dosis en <strong>la</strong> PA d1wn& 1 nocturna, asl como en<br />
<strong>la</strong>s primeras horas <strong>de</strong>l día. A<strong>de</strong>mAs se evaluó su<br />
<strong>efecto</strong> sobre el ritmo circadiano y <strong>la</strong> efectividad antihipertensiva<br />
<strong>48</strong> a <strong>72</strong> hcns <strong>de</strong>spués <strong>de</strong> <strong>la</strong> última<br />
dosis administrada.<br />
MATERIALY METODO<br />
Se realizó un estudio abierto, simple ciego, no<br />
comparativo, contro<strong>la</strong>docoo p<strong>la</strong>cebo, <strong>de</strong> ocho semanas<br />
<strong>de</strong> duración en 30 pacientes <strong>de</strong> <strong>la</strong> consulta externa,<br />
los cuales dieron suconsentimiento informado<br />
por escrito antes <strong>de</strong> ser integrados al estudio.<br />
Se incluyeron pacienl2S adultos, mayores <strong>de</strong> 21<br />
años <strong>de</strong> edad, con diagnóstico <strong>de</strong> hipertensión arterial<br />
sistémica (HAS) leve a mo<strong>de</strong>rada. Tal diagnóstico<br />
se estableció si el promedio <strong>de</strong> dos tomas <strong>de</strong> <strong>la</strong><br />
presión arterial diastólica (pAD) en posición se<strong>de</strong>nte<br />
(utilizando el mismo brazo) estaba entre 95-115<br />
mmHg. Las tomas <strong>de</strong> <strong>la</strong> PAD se realizaron con un<br />
intervalo <strong>de</strong> por lo menos una semana. La diferencia<br />
entre el promedio <strong>de</strong> <strong>la</strong>s dos tomas diastólicas<br />
no <strong>de</strong>bió variar más <strong>de</strong> 10 mmHg. La HAS no <strong>de</strong>b<strong>la</strong><br />
ser secundaria a hiperaldosteronismo, feocromocitoma,<br />
estenosis <strong>de</strong> <strong>la</strong> arteria renal, coartación <strong>de</strong> <strong>la</strong><br />
aorta, enfermedad <strong>de</strong> Cushíng o anticonceptivos<br />
orales. Los pacientes fueron valorados con historia<br />
médica y examen físíco completo un mes antes <strong>de</strong>l<br />
comienzo <strong>de</strong>l estudio.<br />
Se excluyó a pacientesembarazadas, amamantando<br />
o en riesgo <strong>de</strong> embarazo, pacientes con fármacos<br />
no usados como <strong>antihipertensivo</strong>s pero con <strong>efecto</strong>s<br />
<strong>antihipertensivo</strong>s o con finnacos que causan vasodi<strong>la</strong>tación<br />
o vasoconstricci6n sistémica, como<br />
anti<strong>de</strong>presores tridclicos o preparaciones para resfrío<br />
o tos que contengan simpaticomiméticos y pacientes<br />
tratados con otras drogas <strong>de</strong> investigación<br />
un mes previo al estudio o durante el mismo. Se excluyeron<br />
también los pacientes con angor pectoris,<br />
<strong>de</strong>scompensacíón cardiaca o evi<strong>de</strong>ncia clínica <strong>de</strong><br />
insuficienCia cardíaca. arritIñia severa o bloqueocar-<br />
díaco mayor <strong>de</strong> primer grado.<br />
La historia <strong>de</strong> disfunci6n hepática o <strong>la</strong> presencia<br />
clínicamente significativa<strong>de</strong> pruebas <strong>de</strong> función hepática<br />
anormales (fosfatasa alcalina, bilirrubinas totales,<br />
transaminasas), <strong>de</strong>scompensación renal o creatinina<br />
sérica <strong>de</strong> 3,0 mg!dl, hipotensión ortostática<br />
dada por disfunción autonómica no contro<strong>la</strong>ble con<br />
hidratación o cambios en el medicamento fueron<br />
causas <strong>de</strong> exclusión. al igual que <strong>la</strong> evi<strong>de</strong>ncia <strong>de</strong> daño<br />
a órganos b<strong>la</strong>nco (retinopatia grado mo IV, daño<br />
renal o cardiaco) o condiciones médicas que pudieran<br />
interferir en <strong>la</strong> finalización <strong>de</strong>l estudio o que<br />
pudieran aumentar el riesgo a los pacientes. También<br />
fueron excluidos los pacientes con historia <strong>de</strong><br />
alcoholismo, drogadicción o alteraciones mentales,<br />
hipertensión malignae historia<strong>de</strong> hipersensibilidad<br />
prr<br />
típ:<br />
(<br />
abé<br />
car<br />
pn<br />
no<br />
da,<br />
do:<br />
los<br />
el (<br />
.to.<br />
yr<br />
ine<br />
ine<br />
a1<br />
el ,<br />
di,<br />
tra<br />
na<br />
pu<br />
rec<br />
mI<br />
Pf'<br />
" ,<br />
re;<br />
rasil<br />
gr<br />
nc<br />
tv<br />
ti',<br />
' /<br />
cn<br />
SI;<br />
so<br />
<strong>la</strong><br />
<strong>la</strong><br />
d(<br />
vi<br />
re<br />
tn<br />
n~
1996<br />
AML.JD1PINA YPRESUROMETRIA AMBULATORIA I J. Z. Parra Carrillo y col.<br />
33<br />
Sen<br />
6 su<br />
f antima<br />
, no<br />
a<br />
ex<br />
a<br />
~.<br />
21<br />
te<br />
Sti<br />
~<strong>la</strong><br />
te<br />
15<br />
Wl<br />
m<br />
:as<br />
)fa<br />
ci<strong>la</strong><br />
os<br />
ia<br />
el<br />
previa a los bloqueantes <strong>de</strong> los canales <strong>de</strong> calcio <strong>de</strong>l<br />
tipo <strong>de</strong> <strong>la</strong>s dihidropiridinas.<br />
Se eliminaron <strong>de</strong>l estudio aquellos sujetos que<br />
abandonaron el tratamiento, los que tomaron medicamentos<br />
vasoactivos que modifican <strong>la</strong>s cifras <strong>de</strong><br />
presión arterial durante los días <strong>de</strong>l monitoreo y los<br />
no registraron a<strong>de</strong>cuadamente su diario <strong>de</strong> activida<strong>de</strong>s.<br />
Los registros en los que por Wl perlodo <strong>de</strong><br />
dos horas no existieron por lo menos dos lecturas y<br />
los queno completaron por lo menos 30lecturas en<br />
el día fueron <strong>de</strong>scartados.<br />
El estudio comprendió 12 semanas <strong>de</strong> tratamiento,<br />
incluyendo tres fases: p<strong>la</strong>cebo, ajuste <strong>de</strong> <strong>la</strong>s dosis<br />
y mantenimiento.<br />
.La fase <strong>de</strong> p<strong>la</strong>cebo, <strong>de</strong> dos semanas <strong>de</strong> duración,<br />
incluyó a los pacientes que llenaron los criterios <strong>de</strong><br />
inclusión. Los pacientes recibieron p<strong>la</strong>cebo simi<strong>la</strong>r<br />
a <strong>la</strong> tableta <strong>de</strong> 5 mg <strong>de</strong> amlodipína, una vez al día en<br />
el <strong>de</strong>sayuno. Se realizó toma <strong>de</strong> PA, frecuencia cardiaca<br />
(Fe), peso y evaluación <strong>de</strong>l cumplimiento <strong>de</strong>l<br />
tratamiento al final <strong>de</strong> <strong>la</strong> primera y segunda semanas.<br />
La PA Y <strong>la</strong> Fe se evaluaron 22 a 24 horas <strong>de</strong>spués<br />
<strong>de</strong> <strong>la</strong> última dosis <strong>de</strong> p<strong>la</strong>cebo. Los pacientes<br />
reóbieron instrucciones <strong>de</strong> cómo tomar el medicamento<br />
24 horas antes <strong>de</strong> su visita a <strong>la</strong> consulta. El<br />
promedio <strong>de</strong> dos mediciones <strong>de</strong> PAD (sentado) fue<br />
<strong>de</strong> 95 a 115 mmHg al final <strong>de</strong> <strong>la</strong> primera y segunda<br />
semanas y no varió más <strong>de</strong> 10 mmHg entre <strong>la</strong>s tomas.<br />
El promedio <strong>de</strong> <strong>la</strong>s PA al final <strong>de</strong> <strong>la</strong> segunda<br />
semana se consi<strong>de</strong>ró como <strong>la</strong> PA basal. Se hizo Wl<br />
registro basal <strong>de</strong> monitoreo ambu<strong>la</strong>torio en 24 horas<br />
(MAPA) durante <strong>la</strong> última visita <strong>de</strong> esta fase,<br />
siempre y cuando <strong>la</strong> PA cumpliera <strong>la</strong>s cifras <strong>de</strong> ingreso<br />
a <strong>la</strong> fase <strong>de</strong> tratamiento activo .<br />
La fase <strong>de</strong> ajuste <strong>de</strong> dosis (fase TI) fue <strong>de</strong> 8 semanas.<br />
Se inició el tratamiento activo con <strong>amlodipina</strong> 5<br />
mg por día en dosis única antes <strong>de</strong> <strong>la</strong>s 10 <strong>de</strong> <strong>la</strong> mañana.<br />
Se realiz6 MAPA al primer día <strong>de</strong> tratamiento.<br />
Cada dos semanas los pacientes regresaron a <strong>la</strong><br />
consulta para control. A <strong>la</strong>s cuatro Semanas se aj1,1St6<strong>la</strong><br />
dosis a 10 mg por dia en los casos en que <strong>la</strong><br />
PAD (sentado) era superior o igual a 90 mmHg; ésta<br />
fue <strong>la</strong> dosis máxima a administrar. Se disminuyó o<br />
suspendió totalmente en los casos <strong>de</strong> <strong>efecto</strong>s adversos<br />
clínicamente significativos y en los casos en que<br />
<strong>la</strong> PAD no había disminuido más <strong>de</strong> 5 mmHg <strong>de</strong>s<strong>de</strong><br />
<strong>la</strong> basal a <strong>la</strong> dosis máxima. Enlos restantes casos se<br />
continuó con <strong>la</strong> dosis inicial hasta finalizar <strong>la</strong> fase<br />
<strong>de</strong> mantenimiento (fase ID). Enningún caso fue necesario<br />
reajustar <strong>la</strong> dosis a <strong>la</strong>s ocho semanas.<br />
Durante <strong>la</strong> fase <strong>de</strong> mantenimiento (fase ID), <strong>de</strong><br />
dos semanas <strong>de</strong> duración, los pacientes se mantuvieron<br />
con <strong>la</strong> dosis <strong>de</strong> amIodipina con <strong>la</strong> que lograron<br />
en <strong>la</strong> fase TI <strong>la</strong> PAD <strong>de</strong>seada o con <strong>la</strong> dosis máxima<br />
<strong>de</strong> ajuste. Durante el último día <strong>de</strong> <strong>la</strong> fase <strong>de</strong><br />
mantenimiento se llevó a cabo MAPA, así como en<br />
el tercer día posterior a <strong>la</strong> última dosis <strong>de</strong> amlodípína<br />
(<strong>48</strong>-<strong>72</strong> horas posúltima dosis).<br />
Los pacientes <strong>de</strong>volvieron el medicamento no utilizado<br />
al fínal <strong>de</strong> cada semana para valorar el cumplimiento.<br />
Valoraciones<br />
PAyFC<br />
Detmninacián <strong>de</strong> ]Q PA cDnvenci011JlI<br />
a) El sujeto permaneció sentado durante 5 minutos,<br />
<strong>la</strong> PA y <strong>la</strong> FC se tomaron <strong>de</strong>spués <strong>de</strong> este periodo<br />
<strong>de</strong> reposo, con el brazo apoyado y a <strong>la</strong> altura <strong>de</strong>l<br />
corazón.<br />
b) La presión arterial sistólica se <strong>de</strong>terminó con<br />
el primer ruido <strong>de</strong> Korotkoff y <strong>la</strong> presión arterial<br />
diast6lica con el quinto ruido. Las mediciones <strong>la</strong>s<br />
realizó el mismo investigador.<br />
e) En todas <strong>la</strong>s visitas subsecuentes los pacientes<br />
fueron evaluados22 a 24horas <strong>de</strong>spués <strong>de</strong> <strong>la</strong> última<br />
dosis <strong>de</strong> amlodipína,<br />
Mcmitoreo ambu<strong>la</strong>torio IÜ 1Jl PA<br />
Los pacientes fueron evaluados durante el último<br />
día <strong>de</strong> <strong>la</strong> fase J,el primer dia <strong>de</strong> tratamiento activo<br />
y el último día <strong>de</strong> <strong>la</strong> fase m, así como <strong>48</strong> horas<br />
<strong>de</strong>spués <strong>de</strong> terminar el tratamiento activo.<br />
a) Las <strong>de</strong>terminaciones <strong>de</strong> <strong>la</strong> PA ambu<strong>la</strong>toria se<br />
realizaron con <strong>la</strong> unidad Pulse Trend <strong>de</strong> HlLLMED.<br />
La duración <strong>de</strong>l monitoreo fue <strong>de</strong> 24 horas,<br />
iniciándoseentre <strong>la</strong>s 8Y<strong>la</strong>s9 <strong>de</strong> <strong>la</strong> mañana para cada<br />
día <strong>de</strong> registro. El período diurno se registró <strong>de</strong>s<strong>de</strong><br />
<strong>la</strong>s 7 hasta <strong>la</strong>s 22 horas (l5 horas). El perlodo nocturno<br />
comprendió <strong>de</strong>s<strong>de</strong> <strong>la</strong>s 22 hasta <strong>la</strong>s 7 horas (9 horas).<br />
Las mediciones se tomaron cada 15 minutos<br />
durante el periodo diurno y cada 20minutos durante<br />
el nocturno.<br />
b) El sujeto llen6 un pequeño diario <strong>de</strong> activída<strong>de</strong>s<br />
en <strong>la</strong>sque se <strong>de</strong>stacó: hora <strong>de</strong>l día en que se levanta<br />
<strong>de</strong> <strong>la</strong> cama y comienza a <strong>de</strong>ambu<strong>la</strong>r, hora <strong>de</strong><br />
entrada y salida <strong>de</strong>l trabajo, hora <strong>de</strong> <strong>la</strong>s comidas,<br />
hora en que se acuesta alUlque no duerma y número<br />
<strong>de</strong> horas <strong>de</strong> sueño.<br />
e) No se permitióel ejercicio durante los monitoreos.<br />
d) Durante <strong>la</strong> toma <strong>de</strong> <strong>la</strong> PA ambu<strong>la</strong>toria en cada<br />
medición el sujeto pennaneció sentado, <strong>de</strong> pie o acostado<br />
sin moverse ni hab<strong>la</strong>r, hasta que ésta terminó.<br />
Variables <strong>de</strong>l estudio<br />
Se <strong>de</strong>terminaron los siguientes aspectos <strong>de</strong> <strong>la</strong> PA<br />
y se utilizaron <strong>la</strong>s siguientes <strong>de</strong>finiciones: .<br />
A) Hipertensión arUrW<br />
PA igual o mayor a 140/95 mmHg en dos tomas
34 REVISTA ARGENTINA DE CARDlOLOGIA, VOL. 64, SUPLEMENTO IV 1996<br />
Al<br />
. ~~1<br />
Presl6n arterial convendonalu<strong>de</strong>nte, s<strong>la</strong>lóUcl (PAS), dlut6Uca (PAD>, frecuencia clrdfaa (fQ. morn promedio ±duviad6n<br />
utindar (DEI, en 30 pa<strong>de</strong>ntes tratados con amJodfpina<br />
PÚlctbo<br />
2' St1fUlrtll<br />
dt IJCtivo<br />
...<br />
...<br />
PAS"(mmHg) 158,3± 15,4 144,3± 17,5<br />
PAD(mmHg) 100,2±6,2 91.1 :i:9,4<br />
ns<br />
FC(l/m)+ 75,2:i:6,7 74,8:i: 9,8<br />
Los valores <strong>de</strong> p comparados a p<strong>la</strong>cebo. • p < O,OS. .. P < 0,01.<br />
4' 5mulM rSmws.t 10" StmIlrtll<br />
dttldiro ItIlCtitlo dt activo<br />
... ... ...<br />
... ... .<br />
87,3±7,5 It6,U7,3 86,4 *5,6<br />
ru ns •<br />
<strong>72</strong>,8 ± 8,5 73,2:t 7,9 71,5:i:7,7<br />
137,8:i: 19,7 137,3* 15,1 136,8 ± 12,2<br />
... P < 0,001. ns· No signiflQtiva. :t lAtidos por minuto.<br />
1<br />
1<br />
1<br />
diferentes en dos ocasiones distintas con el método<br />
convencional.<br />
B) Monitoreo ambu<strong>la</strong>torio<br />
Presión arterial media<br />
Se calculó con <strong>la</strong> siguiente fórmu<strong>la</strong>:<br />
PAM: Presión arterial media<br />
PAS: Presión arterial sistólica<br />
PAD: Presión arterial diastólica<br />
. PAM =PAD + 1/3 (PAS - PAD)<br />
Úlrga total hipertensioa<br />
Se <strong>de</strong>fine como el porcentaje <strong>de</strong> lecturas <strong>de</strong> PA<br />
sistólica-mayor <strong>de</strong> 140 mmHg y <strong>de</strong> PADpor arriba<br />
<strong>de</strong>90mmHg.<br />
El análisis estadístico se llevó a cabo con el programa<br />
EPI INFO versión 6.0. Los valores se expresan<br />
en media ± <strong>de</strong>sviación estándar (DE).<br />
. "<br />
RESULTADOS<br />
Se estudiaron 33 pacientes, <strong>de</strong> los cuales tres se<br />
excluyeron por <strong>efecto</strong>s secundarios; dos <strong>de</strong> ellos por<br />
cefalea intensa y el tercero por e<strong>de</strong>ma <strong>de</strong> extremida<br />
" . .<br />
<strong>de</strong>s inferiores a<strong>de</strong>más <strong>de</strong> cefalea y constipación intestinal.<br />
De los 30 pacientes en los que se completó el estudio,<br />
25correspondieron al género femenino y 5 al<br />
masculino. El peso promedio <strong>de</strong> estos pacientes fue<br />
<strong>de</strong> 71,7 ± 12,1 kg, <strong>la</strong> edad promedio <strong>de</strong> 52,9 ± 8,9<br />
años (30-65) y el tiempo <strong>de</strong> evolución <strong>de</strong> <strong>la</strong> hipertensión<br />
6,4 ± 4,5 años.<br />
En <strong>la</strong> Tab<strong>la</strong> 1 se observa que <strong>la</strong> PAconvencional,<br />
en posición se<strong>de</strong>nte, durante el período <strong>de</strong> p<strong>la</strong>cebo<br />
fue <strong>de</strong> 158,3 ± 15,4 / 100,2 ± 6,2 mmHg con FC <strong>de</strong><br />
75,2 ± 6,7 <strong>la</strong>tidos por minuto (l/m), <strong>de</strong>scendiendo<br />
hasta 136,8± 12,2 / 86,4±5,6mmHg (p < 0,(01), con<br />
Fe <strong>de</strong> 71,5± 7,7 l/m (p < O,OS), en <strong>la</strong> décima semana<br />
<strong>de</strong> tratamiento.<br />
La PAconvencional en ortostatismo no presentó<br />
diferencias significativos en re<strong>la</strong>ción con <strong>la</strong> se<strong>de</strong>nte.<br />
En<strong>la</strong> Tab<strong>la</strong> 2 se observa que <strong>la</strong> PA<strong>de</strong> 24 horas con<br />
monitoreo ambu<strong>la</strong>torio al final <strong>de</strong> p<strong>la</strong>cebo fue <strong>de</strong><br />
146,6 ± 18,4 / 93,7 ±7;l/J mmHg, con FC 76,0 ±8,71;<br />
sin cambios significativos en el primer día <strong>de</strong> tratamiento<br />
con <strong>amlodipina</strong> (Figura 1). A <strong>la</strong>s 10 semanas<br />
<strong>de</strong> tratamiento <strong>la</strong> PA<strong>de</strong>scendió hasta 131,0 ±15,34 /<br />
85,0 ± 6,6 mmHg (p < 0,(01) (Tab<strong>la</strong> 2); <strong>la</strong> FC fue <strong>de</strong><br />
Fl<br />
P<br />
rr<br />
Tab<strong>la</strong> 1<br />
Presl6n arterh1 slst6lica (PAS),dJ,ut6lica (PADI,medía (PAMI, frecuencia canUaca (fC), carga ltItal kJputenslva sist6lica
AMLODIPINA y PRESUROMETRlA AMBULATORIA I J.Z. Parra Carrillo y col. 35<br />
11<br />
uunHg<br />
180....-------------------.<br />
2<br />
-- Sist B<br />
120 . + Díast B<br />
"* Sist AML<br />
___ Diast AML<br />
e<br />
9 601-----------------<br />
8 10 12 14 16 18 20 22 24 2 4 6<br />
Tiempo (horas)<br />
1,<br />
) Fig. 1. Grifico comparativo <strong>de</strong>l comportamiento <strong>de</strong> <strong>la</strong> PAS y PAD evaluado con MAPA <strong>de</strong> 24 horas en 11 fase p<strong>la</strong>cebo y luego <strong>de</strong> <strong>la</strong><br />
primen dosis <strong>de</strong> arnlodipína, B:basal. AML: <strong>amlodipina</strong><br />
mmHg<br />
180,.---------------------,<br />
-- Sist B<br />
+ Diast B<br />
120 _ ~~<br />
*" Sist AML<br />
-It-<br />
Díast AML<br />
601--------------------'<br />
8 10 12 14 16 18 20 22 24 2 4 6<br />
Fig. 2. Gñfico comparativo <strong>de</strong>l comportamiento <strong>de</strong> <strong>la</strong> PAS y PAD evaluado con MAPA <strong>de</strong> 24 horas en <strong>la</strong> fase p<strong>la</strong>cebo y luego <strong>de</strong> 4<br />
semanas <strong>de</strong> tratamiento con <strong>amlodipina</strong>. B:basal. AML: amIodlpina (fin <strong>de</strong>l tratamiento). .
36 REVISTA ARGENTINA DE CARDlOLOClA. VOL. 64. SUPLEMENTO IV 1996<br />
/<br />
Tab<strong>la</strong>'<br />
Presión arterial sistólica (PASI. diutóUca (PADI, media (pAM), mcuenda cardíaca (FO. arp total hJpatelUlva.I.t6Uca (CTHS)<br />
'1 diutólica (CTHDI, valora promtdio ± DE durantt el periodo diwno (6 a 2.1 horas) por monitoreo ambu<strong>la</strong>torio.<br />
en 30 pacientes tnt.ado. con <strong>amlodipina</strong><br />
Final th p<strong>la</strong>etbo 24hcmI.ctitIo JO lCffJtMS .cfiw <strong>48</strong>-<strong>72</strong> hort2s posúltinul D<br />
ns<br />
PAS(mmHg) 151,2± 18,3 U8.4±2{),l<br />
ni<br />
134,5 :t 16.1<br />
PAD(mmHg) 97,7t. 7,5 95,5±9.9 88,3 ± 6,4<br />
-<br />
-<br />
140,5 ± 17.a<br />
o..<br />
92,3 ± 6.9<br />
ns<br />
PAM(mmHg) <strong>la</strong>,6±9,5 113,1± 11.9 103.1U.6 107,5±8,2<br />
ns ns ns<br />
Fe (I/m)+ 79,5±9.97 81.1 ± 13,5 BO,3:tU<br />
80,0+ 7.7<br />
ni<br />
Sistólica ('Yo) 66,3:t 26,3 6O,3:t29,5<br />
38.H30,5<br />
44,7±31,97<br />
ns<br />
o<br />
Diastólica ('Yo) 67,5:t 19.4 6O,6±22,1 4l.9±22.2 5S,7±23,2<br />
Losvalores <strong>de</strong> p comparados a p<strong>la</strong>cebo . o p < 0,05. .. P < 0,01. ."p < 0,001. ns » No signific.ativa. + Latidos por minuto.<br />
-<br />
-<br />
1<br />
1<br />
1<br />
J<br />
J<br />
76,8 ± 7,83 l/m (p NS). En el período <strong>de</strong> <strong>la</strong>s <strong>48</strong>-<strong>72</strong><br />
horas luego <strong>de</strong> <strong>la</strong> última dosis <strong>de</strong> <strong>amlodipina</strong>, <strong>la</strong> presión<br />
se encontró en 135,4 ± 25.1 / 88,8 ± 6.9 mmHg<br />
(p < 0.01), y <strong>la</strong> Fe en 75,9 ± 6.22 l/m (p NS) (Figura<br />
3). También se aprecia que <strong>la</strong> carga total hípertensíva<br />
sistólica <strong>de</strong>scendió <strong>de</strong> 58,4 ± 26,1% al final <strong>de</strong>l<br />
período p<strong>la</strong>cebo, a 34,9±31,7% (p < 0,001) en <strong>la</strong> décima<br />
semana <strong>de</strong> tratamiento, ya <strong>la</strong>s <strong>48</strong>-<strong>72</strong> horas <strong>de</strong><br />
<strong>la</strong> última dosis fue <strong>de</strong> 39.7 ± 30,0% (p < 0,001). La<br />
carga hipertensiva total diastólica <strong>de</strong>scendió <strong>de</strong> 55,4<br />
± 17% al final <strong>de</strong> p<strong>la</strong>cebo. a 33,1 ± 20% (p < 0,001) en<br />
<strong>la</strong> décima semana <strong>de</strong> tratamiento y a <strong>la</strong>s <strong>48</strong>-<strong>72</strong> horas<br />
<strong>de</strong> <strong>la</strong> última dosis fue <strong>de</strong> 45,8 ±20,8% (p NS).<br />
En <strong>la</strong> Tab<strong>la</strong> 3 se observa que en el período diurno<br />
(6 a 22 horas) el <strong>de</strong>scenso <strong>de</strong> <strong>la</strong> PA, así como el <strong>de</strong>scenso<br />
<strong>de</strong> <strong>la</strong>s cargas hipertensivas sistólica y diastólica<br />
fue sigrúficativo a <strong>la</strong>s 10 semanas <strong>de</strong> tratamiento<br />
activo, permaneciendo aún significativo <strong>48</strong> a <strong>72</strong><br />
horas <strong>de</strong>spués <strong>de</strong> <strong>la</strong> última dosis <strong>de</strong> <strong>amlodipina</strong>. En<br />
forma simi<strong>la</strong>r. durante el periodo nocturno el <strong>de</strong>scenso<br />
fue significativo a <strong>la</strong>s10 semanas <strong>de</strong> tratamiento<br />
(Tab<strong>la</strong> 4). Sin embargo, en el <strong>la</strong>pso <strong>de</strong> <strong>48</strong> a <strong>72</strong> horas<br />
<strong>de</strong> <strong>la</strong> última dosis, aunque los valores <strong>de</strong> presión<br />
arterial y cargas totales hipertensivas son menores<br />
que con p<strong>la</strong>cebo. <strong>la</strong>s diferencias no son estadísticamente<br />
significativas.<br />
En <strong>la</strong> Tab<strong>la</strong> 5 se pue<strong>de</strong> apreciar que <strong>la</strong> PA sistólica<br />
se normalizó en 21 <strong>de</strong> los 30 pacientes tratados<br />
con <strong>amlodipina</strong> (70%) tanto con el método convencional<br />
<strong>de</strong> toma como con el monitoreo <strong>de</strong> 24 horas<br />
y el <strong>efecto</strong> persistió en 19 (63%) <strong>48</strong> a <strong>72</strong> horas <strong>de</strong>spués<br />
<strong>de</strong> <strong>la</strong> última dosis <strong>de</strong> amlodípína. En cuanto a<br />
<strong>la</strong> PA diastólica, <strong>de</strong>scendió a menos <strong>de</strong> 90 mmHg<br />
en 20 (67%) <strong>de</strong> los pacientes mediante toma convencional,<br />
pero con monitoreo ambu<strong>la</strong>torio, 2S<br />
(83%) <strong>de</strong> los pacientes lograron estas cifras. A <strong>la</strong>s<br />
Tab<strong>la</strong>t<br />
Pruión arterial slst6lica (PASI. diast6lica tPAD), media (PAM), frtcuenda cardíaca 0:0, carp total hJpertmslva si!tólica (CTHS) y<br />
dlut6llca (C'THDI, valores promedio ± <strong>de</strong>sviadón ur.tnchr (DEI durante un periodo noctumo (2.1 a , koml por moniloreo<br />
ambuJatorio, en 30 pa<strong>de</strong>ntu tratado. con amlodlpw<br />
P<strong>la</strong>cebo 241wnu JOstmJmlll <strong>48</strong>-<strong>72</strong> hort2S<br />
ns • ns<br />
PAS(rnmHg) 135.6±21.t 132.9±20,O UU±2ll.t<br />
126,8± 16.8<br />
nJ<br />
ns<br />
PAD(mmHg) 84.9±9.1 83,9±U,3 78,O±7,t ·<br />
8l.6 ± 8,5<br />
ns<br />
ns<br />
PAM(mmHg) 101,7± 11,7 100,3± 13,5 93,O±8,9 96.7 ± 10,2<br />
nJ nJ nJ<br />
fCO/m)+ 69,2± 8.1 68,8:t1.6 12,8:19,9 68,9 ± 6.9<br />
ns<br />
-<br />
ns<br />
Sistólica (%) 40,3± 33,t 30,9 ± 31,5 · 20,6 ± 28.9 27,4:t 30.7<br />
ns<br />
ns<br />
OiaslóUca 'Yo) 2B.8 ± 24,1 28,o±23.1 14,3±19,3 23,4±22,9<br />
-<br />
-<br />
..<br />
Los valores <strong>de</strong> p comparados a p<strong>la</strong>cebo. o p < 0,05. .. P < 0.01. -<br />
P < 0,001. nJ. No significativa. + <strong>la</strong>tidO\! por minuto.
SMlZW_1<br />
rzwmrn*1ft'Sfttfilllliilia<br />
V 1996<br />
1HS)<br />
AMLODIPINA y PRESUROMETRlA AMBULATORIA I J. Z. Parra Carrillo y coL<br />
mmHg<br />
... .<br />
1S0.----~---~-------,<br />
37<br />
160 .<br />
... Sist AML<br />
..... Diast AML<br />
120 '* Sist <strong>48</strong> h posdosis<br />
100 .<br />
-+- Diast <strong>48</strong> h posdosis<br />
so<br />
601.------------------.J<br />
ores 8 10 12 14 16 18 20 22 24 2 4 6<br />
ica-<br />
l.En<br />
<strong>de</strong>suenhoíón<br />
'ólidos<br />
en<br />
ras<br />
Fig. 3. Gr~fico comparativo <strong>de</strong>l comportamiento <strong>de</strong> u PAD y PAS evaluado con MAPA <strong>de</strong> 2thoras <strong>de</strong>spués <strong>de</strong> 10 semanas <strong>de</strong> tratamiento<br />
ya <strong>la</strong>s 24-<strong>72</strong> horas postratamiento. AML: <strong>amlodipina</strong> (fin <strong>de</strong>l tratamiento).<br />
mmHg<br />
es 180..-----------------.<br />
)a<br />
ig<br />
n<br />
!5 160<br />
LS<br />
--<br />
.. Sist B<br />
+<br />
Diast B<br />
Sist AML<br />
120 . .<br />
.... DiastAML<br />
80 J ••~ ~ .-.T":..._<br />
"*<br />
Sist <strong>48</strong> h posdosis<br />
-+- Diast <strong>48</strong> h posdosis<br />
60---------------..,...-----1<br />
8 10 12 14 16 18 20 22 24 ' 2 4 6<br />
FJg. t. Gráfico comparativo <strong>de</strong>l comportamiento <strong>de</strong> <strong>la</strong> PAD YPASevaluado con MAPA <strong>de</strong> 2t horas <strong>de</strong>spués <strong>de</strong> 10 semanas <strong>de</strong> tratamíenlo<br />
y. <strong>la</strong>s 24-<strong>72</strong> horas postratamiento, en reía<strong>de</strong>n con los valores basales. B: basal. AML: amIodipina (fin <strong>de</strong>l tratamiento).
38 REVISTA ARGENTINA DE CARDlOLOGlA, VOL 64. SUPLEMENTO IV 1996 A i<br />
Tab<strong>la</strong> 5<br />
Número y porcenuJe <strong>de</strong> normallzacl6n <strong>de</strong> <strong>la</strong> presl6n arteriallvaluada medánte toma convmdoD&l '1con monitono<br />
ambu<strong>la</strong>torio (MAPA) <strong>de</strong> 24 horu en 30 pa<strong>de</strong>ntes traudo. con amJodJpina<br />
Tol7UI corwt7lciDnlll<br />
10SellUfnlU activo<br />
Sistólica < 140 mmHg 21 70<br />
Diastólica < 90 mmHg 20 67<br />
Diastólica. 90 mmHg 3 10<br />
<strong>48</strong>-<strong>72</strong> horas <strong>de</strong> <strong>la</strong> última dosis, 17 <strong>de</strong> estos pacientes<br />
(56%) mantenían PA diastólica normal. Tres pacientes<br />
(10%) tuvieron PA diastólica igual a 90<br />
mmHg con toma convencional y dos (6%) con monitoreo<br />
<strong>de</strong> 24 horas, <strong>la</strong> cual se mantuvo luego<br />
<strong>de</strong> suspendido el tratamiento.<br />
En <strong>la</strong> Tab<strong>la</strong> 6 se aprecia <strong>la</strong> normalización <strong>de</strong> <strong>la</strong> PA<br />
sistólica a <strong>la</strong>s 10 semanas <strong>de</strong> tratamiento activo en el<br />
63% <strong>de</strong> los pacientes durante el período diurno yen<br />
87% en el nocturno. Después <strong>de</strong> <strong>48</strong>-<strong>72</strong> horas <strong>de</strong> <strong>la</strong><br />
última dosis <strong>la</strong> PA sistólica diurna permaneció en el<br />
mismo 63% y <strong>la</strong> nocturna <strong>de</strong>scendió 76%. La diastólica<br />
fue menor a 90 rnrnHg en el 60% <strong>de</strong> los pacientes<br />
en el período diurno y en el 97% en el nocturno,<br />
ambos a <strong>la</strong>s 10 semanas <strong>de</strong> tratamiento. En <strong>la</strong>s <strong>48</strong>-<strong>72</strong><br />
horas <strong>de</strong> <strong>la</strong> última dosis encontramos 33% en el período<br />
diurno y 86% en el período nocturno. A <strong>la</strong>s 10<br />
semanas <strong>de</strong> tratamiento activo encontramos una<br />
diastólica igual a 90 rnrnHg en el 10% <strong>de</strong> los pacientes<br />
en el período diurno. A <strong>la</strong>s <strong>48</strong>-<strong>72</strong> horas postraramiento<br />
encontramos 6% <strong>de</strong> los pacientes con presión<br />
diastólica igual a 90 rnrnHg tanto en el período<br />
diurno como en el nocturno.<br />
De los 33 pacientes tratados con arnlodipina y<br />
evaluados para seguridad, los <strong>efecto</strong>s secundarios<br />
encontrados fueron: cefalea en ocho (24%), que<br />
sólo persistió en uno hasta el final <strong>de</strong>l estudio, ya<br />
que dos abandonaron el estudio por este motivo;<br />
náusea en cuatro pacientes (12%); e<strong>de</strong>ma <strong>de</strong> tobi<br />
110sen tres (9%) que persistió en dos hasta el final<br />
(uno se excluyó); disnea en dos pacientes (6%) y<br />
constipación, mareo o insomnio en uno (3%).<br />
N<br />
"<br />
N<br />
21<br />
2S<br />
2<br />
MAPA 24 horlU<br />
10mn:l7<strong>la</strong>s activo<br />
"<br />
70<br />
83<br />
6<br />
MAPA <strong>48</strong>-<strong>72</strong> hora<br />
Posúltinu dMiI<br />
DlSCUSlON<br />
Nuestro estudiocorrobora<strong>la</strong> eficacia antihipertensiva<br />
<strong>de</strong> <strong>la</strong> arnlodipina observada por Escu<strong>de</strong>ro y co<strong>la</strong>boradores<br />
y Olivera y co<strong>la</strong>boradores, entre otros.<br />
Se muestra que el <strong>de</strong>scenso es estadísticamente<br />
significativo, tanto en los promedios <strong>de</strong> 24 horas<br />
como en los periodos'diurno y nocturno y que el <strong>efecto</strong><br />
permanece, aunque menor, a <strong>la</strong>s.<strong>48</strong>-<strong>72</strong> horas tanto<br />
en los valores <strong>de</strong> 24 horascomo en el periodo diurno,<br />
que se ha <strong>de</strong>mostrado que es el <strong>de</strong> más riesgo para los<br />
pacientes. Por otro <strong>la</strong>do, <strong>la</strong> carga total hipertensiva<br />
<strong>de</strong>scien<strong>de</strong> significativamente con el tratamiento acti<br />
vo y permanece menor a <strong>la</strong>s~<strong>72</strong> horas, en el prome<br />
die <strong>de</strong> 24 horas y el diurno. Los valores en elperiodo<br />
nocturno son menores en comparación con los basa<br />
les, aunque <strong>de</strong>spués <strong>de</strong> <strong>la</strong>s60 horas los cambiosno se<br />
manifestaron en lo estadístico pero clínicamente son<br />
significativos. Lo anterior nos indica que no sólo exis<br />
te un <strong>de</strong>scenso promedio <strong>de</strong> <strong>la</strong> PA durante <strong>la</strong>s 24<br />
horas, sino que el tiempo que nuestros pacientes per<br />
manecen con niveles superiores a lo normal son sig<br />
nificativamente menores al ser tratados con amlodí<br />
pina Yque esto suce<strong>de</strong> más en elperíodo diurno, que<br />
es don<strong>de</strong> elpaciente presenta cifras <strong>de</strong> PA mayores.<br />
Indirectamente po<strong>de</strong>mos inferir que existe menosvariabilidad<br />
<strong>de</strong> <strong>la</strong> PA, lo que se corre<strong>la</strong>ciona con riesgo<br />
cardiovascu<strong>la</strong>r menor.<br />
Finalmente, <strong>de</strong>bemos resaltar que, hasta don<strong>de</strong><br />
sabemos, éste es el único estudio con monitoreo<br />
ambu<strong>la</strong>torio que analiza los <strong>efecto</strong>s <strong>de</strong> <strong>la</strong> amlodípína<br />
sobre <strong>la</strong> PA durante el período <strong>de</strong> <strong>48</strong>-<strong>72</strong> horas<br />
<strong>de</strong> <strong>la</strong> última dosis y que su eficacia y <strong>efecto</strong> prolon-<br />
N<br />
"<br />
gl<br />
al<br />
al<br />
~<br />
ro<br />
te<br />
19 63 2~<br />
17 56<br />
<strong>la</strong><br />
2 6<br />
Tab<strong>la</strong> 6<br />
Número y porcentaje <strong>de</strong> normüWd6n <strong>de</strong> <strong>la</strong> presi6n arteria! evahuda con monitoreo ambubtorio (MAPA) <strong>de</strong> 24 hora,.<br />
diurno (6 a 22 horas) y nocturno (22 a 6 horas) en 30 paeíentes lraudo. con amJodlpina . l<br />
1<br />
24/lOrtU<br />
MAPA <strong>la</strong>SettulJW dt actiw<br />
Diurno<br />
N' % N' % N'<br />
Nocturno<br />
"<br />
MAPA <strong>48</strong>-<strong>72</strong> horasposúllil7Ul dosil<br />
24horas Diurno Noctllrno<br />
N' Ir % N' ,"<br />
SlstóUca < 140 mmHg 21 70 19 63 26 87 19· 63<br />
~ . 19 63 23 76<br />
Dia5tóU~ < 90 mmHg 25 ,83 18 60 . 29 97 17 56 10 33 26 86<br />
Diastólica .. 90 ~mHg 2 6 3 10 2 6 2 6 2 6<br />
"<br />
si<br />
!ir<br />
s'<br />
A<br />
A<br />
T<br />
B<br />
A<br />
'V<br />
ti<br />
fi<br />
1<br />
J'<br />
b<br />
J<br />
Ii<br />
"<br />
f
- AMLoDIPlNA y PRESUROMETRlA AMBU!.ATORlA I J. Z. Parra CarrUlo y col.<br />
39<br />
I<br />
<br />
en<br />
ca<br />
S.<br />
ntf:<br />
ras<br />
ecto<br />
o,<br />
los<br />
va<br />
tiedo<br />
a<br />
se<br />
on<br />
is<br />
24<br />
g.<br />
lile<br />
5.<br />
1<br />
o<br />
gado representan un beneficio extraordinario al<br />
atenuar los <strong>efecto</strong>s <strong>de</strong>l incumplimiento ocasional<br />
al tratamiento, tan frecuente en los pacientes hípertensos.<br />
Se concluye que <strong>la</strong> amlodípína es un medicamento<br />
eficaz y seguro en el tratamiento <strong>de</strong>l paciente<br />
lúpertenso, comprobando su <strong>efecto</strong> durante <strong>la</strong>s<br />
2. horas <strong>de</strong>l día y que éste pue<strong>de</strong> permanecer hasta<br />
<strong>48</strong>-<strong>72</strong> horas <strong>de</strong> <strong>la</strong> última dosis, disminuyendo<br />
significativamente <strong>la</strong> carga total hipertensiva sistó<br />
1ia y diastólica.<br />
SUMMARY<br />
ANTIHYPERTENSlVE EFFECT OF<br />
AMLODIPINE <strong>48</strong> TO <strong>72</strong> HOURS AFfER<br />
TREATMENT. A SruDY wrru AMBULATORY<br />
BLOOD PRESSURE MONITORING<br />
Ara open non-comparative single-blind study in 30<br />
essential hypertensive patients was carried out to<br />
evaluate the efficacy of arnlodipine once a day in the<br />
control of hypertension during the 24 hours. After a<br />
2 weeks-p<strong>la</strong>cebo period, treatment started with 5<br />
mglday increased when necessary alter four weeks<br />
to 10 mg. Duration oi treatment period was 10<br />
weeks. ConventionaI blood pressure measurements<br />
were c.uried out as baseline, week 1, 2.md every two<br />
weeks during treatment periodo Continuous ambu<strong>la</strong>tnry<br />
blood pressure monitoring was performed at<br />
the end of p<strong>la</strong>cebo period, during the firsl day oí<br />
active treatment, during the <strong>la</strong>st day of treatment<br />
and again started <strong>48</strong>hours alter the intake of the <strong>la</strong>st<br />
<strong>de</strong>se. Average conventional blood pressure dropped<br />
from 158.3±15.4/100.2±6.2at the cnd ofpIacebo to<br />
136.8 ± 12.2/86.4 ± 5.6 mmHg. Changes in blood<br />
pressure registered by continuous ambuJatory<br />
blood pressure monitoring were 14f ±18.4 to 131 ±<br />
14.4 mmHg for systolic and 93.7 ± 7.3 to 85.0 ± 6.6<br />
mmHg for diastolic al the end of p<strong>la</strong>cebo and active<br />
trutment periods respeclively (p < 0.001). Total hypmensive<br />
systolic and diastolic hypertensive burdrn<br />
were reduced significantIy at the end oi treatment<br />
as well as <strong>48</strong>-<strong>72</strong> hours alter <strong>la</strong>st dose. There<br />
we:re no significant changes in heart rateo Results<br />
<strong>de</strong>monstrate the antihypertensive efficacy of amIadipine<br />
during 24 hours and its antihypertensive action<br />
remains <strong>48</strong>·<strong>72</strong> hours after discontinuation of<br />
the treatment, and the potenliaI protection to the<br />
palient thal forgel one or two doses.<br />
1