Das UniversitätsSpital Zürich - Rheuma Schweiz
Das UniversitätsSpital Zürich - Rheuma Schweiz
Das UniversitätsSpital Zürich - Rheuma Schweiz

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Editorial<br />
Impressum<br />
Gastkolumne<br />
<strong>Das</strong> <strong>UniversitätsSpital</strong> <strong>Zürich</strong> –<br />
ein erstaunliches Spital<br />
State of the art<br />
Basistherapie der rheumatoiden<br />
Arthritis (RA)<br />
Schwerpunkt<br />
Kiefernekrose unter<br />
Bisphosphonaten –<br />
aktueller Wissensstand<br />
Kongress<br />
ACR 2007<br />
Persönlich<br />
www.rheumaportal.ch<br />
Inhalt<br />
Publikationen<br />
Fort- und Weiterbildung<br />
<strong>Rheuma</strong>klinik und Institut für Physikalische Medizin<br />
45<br />
XXXXX<br />
2<br />
2<br />
3<br />
6<br />
8<br />
11<br />
18<br />
20<br />
22<br />
<strong>UniversitätsSpital</strong> <strong>Zürich</strong><br />
rheuma<br />
NACHRICHTEN<br />
Innehalten und Staunen –<br />
es lohnt sich<br />
Seite 3<br />
41–2006
2<br />
editorial<br />
PIUS BRÜHLMANN<br />
Liebe Kolleginnen, liebe Kollegen<br />
Seit einem halben Jahr ist Professor Dr. med. Urs Martin Lütolf Ärztlicher<br />
Direktor des <strong>UniversitätsSpital</strong>s <strong>Zürich</strong> und Autor unserer Gastkolumne. In einer<br />
sehr persönlichen Art erleben wir seinen Blick auf unser Spital aber auch auf den<br />
Sinn von Innehalten und Staunen, was in der heutigen Zeit als erster Eindruck<br />
überraschend sein mag. Für seine Tätigkeit an der Spitze des USZ wünschen wir<br />
Herrn Professor Lütolf viel Erfolg.<br />
Die Behandlung der rheumatoiden Arthritis wird durch die Einführung neuer<br />
Biologika und Kombinationstherapien immer komplexer. <strong>Das</strong> Ziel unserer «State<br />
of the Art-Übersichten» ist es, praxistaugliche Richtlinien in kurzer und knapper<br />
Form, basierend auf der neueren Literatur, zu präsentieren. In einem weiteren<br />
Beitrag wird der Stellenwert der Knochennekrose im Bereich des Kiefers unter<br />
einer Bisphosphonat-Therapie beleuchtet.<br />
Die Präsentationen am American College of <strong>Rheuma</strong>tology 2007, in Boston, sind<br />
Zeichen der vielfältigen und qualitativ hochstehenden Tätigkeit der Forschungsabteilung.<br />
Für Ihr Interesse und die positiven Rückmeldungen bezüglich unserer <strong>Rheuma</strong>-<br />
Nachrichten möchten wir uns an dieser Stelle bedanken. Wir wünschen Ihnen ein<br />
erfolgreiches 2008.<br />
Mit besten Grüssen<br />
Pius Brühlmann<br />
Impressum<br />
<strong>Rheuma</strong>-Nachrichten<br />
❙ 15. Jahrgang – Ausgabe Nr. 45<br />
❙ Auflage: 1000<br />
❙ Erscheint dreimal pro Jahr<br />
❙ Erscheinungsdatum: Dezember 2007<br />
Redaktion<br />
❙ Beat A. Michel (Klinikdirektor)<br />
❙ Pius Brühlmann (Klinik)<br />
❙ Steffen Gay (Basisforschung)<br />
❙ Daniel Uebelhart (Physik. Medizin)<br />
Autoren dieser Ausgabe<br />
❙ Pius Brühlmann<br />
Dr. med., Leitender Arzt<br />
❙ Diana Frey<br />
Dr. med., Oberärztin, Clinical Trials<br />
❙ Steffen Gay<br />
Professor Dr. med., Leitender Arzt<br />
Zentrum für Experimentelle<br />
<strong>Rheuma</strong>tologie<br />
❙ Diego Kyburz<br />
PD Dr. med., Leitender Arzt<br />
❙ Urs Martin Lütolf<br />
Professor Dr. med., Ärztlicher Direktor<br />
<strong>UniversitätsSpital</strong> <strong>Zürich</strong><br />
Klinikdirektor Radio-Onkologie, USZ<br />
❙ Daniel Uebelhart<br />
PD Dr. med., Leitender Arzt<br />
Institut für Physikalische Medizin<br />
Gestaltung und Druck<br />
Pomcany’s Marketing AG<br />
Aargauerstrasse 250, 8048 <strong>Zürich</strong><br />
Telefon 044 496 10 10<br />
Fotos<br />
Kim Landolt, <strong>Rheuma</strong>klinik und<br />
Institut für Physikalische Medizin<br />
Sponsoring<br />
GRÜNENTHAL Pharma AG<br />
8756 Mitlödi<br />
IBSA Institut Biochimique SA<br />
Via del Piano, P.O. Box 261<br />
6915 Pambio-Noranco<br />
SANOFI Synthélabo (<strong>Schweiz</strong>) SA<br />
11, rue de Veryrot, 1217 Meyrin<br />
Abonnemente<br />
Die <strong>Rheuma</strong>-Nachrichten können kostenlos<br />
abonniert werden bei:<br />
<strong>UniversitätsSpital</strong> <strong>Zürich</strong>, <strong>Rheuma</strong>klinik und<br />
Institut für Physikalische Medizin<br />
Gloriastrasse 25, 8091 <strong>Zürich</strong><br />
Telefon 044 255 29 96<br />
Telefax 044 255 89 78<br />
e-Mail ruzinfo@usz.ch<br />
Internet<br />
www.rheuma-schweiz.ch<br />
Nächste Ausgabe: April 2008
<strong>Das</strong> <strong>UniversitätsSpital</strong> <strong>Zürich</strong> –<br />
ein erstaunliches Spital<br />
Ein flüchtiger Blick durch die Frontscheibe auf nächtlicher<br />
Autobahn reicht nicht. Zum Staunen muss man innehalten,<br />
bereit sein, sich zu etwas Besonderem hinlenken lassen, sich von<br />
Störendem befreien. Der Gang vor die Berghütte vor dem<br />
Schlafengehen, die Schritte weg vom Feuer der Beduinen in der<br />
Wüste ermöglichen dieses Staunen. Um beim Firmament zu<br />
bleiben: Es ist belanglos, wieviel wir über den Urknall wissen, ob<br />
wir über die Position unserer Sonne in der Milchstrasse Bescheid<br />
wissen oder ob wir uns an die Physik der Kernprozesse im<br />
Sonneninnern erinnern. Wissen mag das Staunen auf andere<br />
Ebenen verschieben, aber wird es in der Tiefe nicht zerstören.<br />
Innehalten – Staunen<br />
Als Ärtzlicher Direktor des USZ wurde ich eingeladen,<br />
diese Gastkolumne zu schreiben. Der Blick in den Sternenhimmel<br />
auf einer kürzlichen Reise in die Berge des Sinai<br />
erinnerte mich, mit dem Unergründlichen und der Komplexität,<br />
auch an die Tätigkeiten und unsere Gemeinschaft im<br />
USZ mit seinen unendlich vielen Interaktionsebenen. Kurze,<br />
längere, tiefe und oberflächliche Beziehungen bilden einen<br />
«Organismus», der einer Analyse entgeht. In diesem Organismus<br />
USZ aber liegt, so meine Überzeugung, eine Vielfalt<br />
von Können, ein unschätzbares medizinisches Wissen vor. Es<br />
lohnt sich, gelegentlich innezuhalten und sogar zu staunen.<br />
<strong>Das</strong> USZ ist ein erstaunliches Spital: Ich habe über die<br />
Jahre erleben dürfen, dass das universitäre «unbedingte<br />
Wissen wollen» in unserem Umfeld USZ einen guten Nährboden<br />
findet. Auch wenn die Aussenbedingungen nun<br />
schwieriger geworden sind (ich nenne Budgetkürzungen,<br />
Konkurrenz von Privatspitälern), die Aufgaben für die einzelnen<br />
Mitarbeiterinnen und Mitarbeiter gelegentlich eine<br />
erhebliche Last darstellen, eine unverminderte, tiefe Faszination<br />
ist Triebfeder für Mitarbeitende aus allen Berufsgruppen,<br />
das meine ich auch heute feststellen zu können.<br />
Staunen als Triebfeder für den Fortschritt<br />
Die Medizin, die wir evidenzbasiert betreiben, hat oft mit<br />
Staunen begonnen: Beim Beobachten von Krankheitsverläufen<br />
oder Phänomenen im Labor sind Menschen auf Abnormes<br />
aufmerksam geworden, hielten inne und entwickelten<br />
Experimente, um zu verstehen. Flemming’s Pilze, Fieber, das<br />
Metastasen verschwinden liess, haben so zu Erkenntnissen<br />
und Fortschritten geführt.<br />
URS MARTIN LÜTOLF<br />
Sie alle kennen das Staunen in einer klaren Nacht, weit weg vom Streulicht einer grossen Stadt, wenn wir in den Sternenhimmel<br />
schauen. Wir staunen, weil wir die Pracht des Sternenzelts sehen und staunen vielleicht ob der Unmöglichkeit, das Universum zu<br />
ergründen. Allerdings, da sind ein paar Bedingungen, die es braucht, damit wir überhaupt staunen können.<br />
Beobachtungsgabe und kritisches Hinterfragen ist keine<br />
Exklusivität einer Berufsgattung. In unserem Fachbereich<br />
Radio-Onkologie zum Beispiel hat ein Laborant Beobachtungen<br />
gemacht und Experimente konzipiert, die ganz<br />
wesentlich zum Verständnis und zur Kenntnis der Strahlenbiologie<br />
beitrugen.Aus jeder beruflichen Perspektive werden<br />
Beobachtungen gemacht. Sie sind wertvoll und tragen die<br />
Möglichkeit des Fortschrittes in sich. Die Kultur, auf die solche<br />
Wahrnehmungen in einer Klinik oder in einem Labor<br />
treffen, wird entscheidend sein, ob Fortschritt Tatsache wird.<br />
Natürlich muss dazu das heutige Wissen zur Interpretation<br />
Zur Person<br />
❙ Professor Dr. Urs Martin Lütolf<br />
❙ Ärztlicher Direktor <strong>UniversitätsSpital</strong> <strong>Zürich</strong><br />
❙ Direktor der Klinik für Radio-Onkologie<br />
45–2007<br />
3<br />
GASTKOLUMNE
4<br />
KLININK-<br />
INFORMATION Dienstleistungen<br />
von Beobachtungen zur Verfügung stehen. Wissen über<br />
Anatomie, Physiologie und Pathophysiologie steht zum<br />
Glück im Zeitalter des Internets, der elektronischen Bibliothek<br />
und per Vernetzung allen zur Verfügung. Am USZ sind<br />
wir in dieser Hinsicht privilegiert.<br />
Nochmals die Sterne<br />
Der Stern von Bethlehem, eine «Anomalie» am abendländischen<br />
Himmel, hat den Blick zu einer grossen geschichtlichen<br />
Umwälzung hingelenkt, auch wenn die moderne Astronomie<br />
das Phänomen unterdessen erklärbar gemacht hat.<br />
Die Molekularbiologie, die Zellbiologie, die Systembiologie<br />
haben in der Medizin ebenfalls Vieles erklärbar und auch<br />
therapierbar gemacht. Darob vergessen wir gelegentlich, dass<br />
wir zwar viel, aber nicht das Letzte wissen.<br />
Ich wünsche Ihnen und uns, dass wir den Schwung und die<br />
Möglichkeiten nutzen, zur modernen Medizin beizutragen.<br />
Wir haben in der <strong>Schweiz</strong> und ganz besonders in unserem<br />
Kanton und am USZ ausgezeichnete Voraussetzungen dazu.<br />
Ich wünsche Ihnen und uns aber auch ab und zu ein bedächtiges<br />
Innehalten… und kreatives Staunen.<br />
der <strong>Rheuma</strong>klinik und<br />
Institut für Physikalische Medizin <strong>UniversitätsSpital</strong> <strong>Zürich</strong><br />
Poliklinik<br />
Ambulante Abklärung und Therapie der rheumatischen<br />
Erkrankungen<br />
❙ Konsultation auf Zuweisung durch einen Arzt<br />
Spezielle Dienstleistungen, bestehend auf folgenden Gebieten<br />
❙ <strong>Rheuma</strong>toide Arthritis<br />
– interdisziplinäre Standortbestimmung mit<br />
standardisiertem Qualitätsmanagement<br />
– Radionuklidsynoviorthese<br />
– Experimentelle Therapien<br />
❙ Bindegewebserkrankungen (Kollagenosen, Vaskulitiden)<br />
– interdisziplinäre Abklärung mit Immunologie<br />
– Spezialuntersuchungen<br />
❙ Gelenkerkrankungen<br />
– funktionelle Ultraschalluntersuchung<br />
– diagnostische Nadelarthroskopie<br />
❙ Schmerzpatienten<br />
– ambulantes interdisziplinäres Schmerzprogramm<br />
❙ Rückenerkrankungen<br />
– umfassende Abklärungen<br />
– Infiltrationen unter bildgebender Kontrolle<br />
❙ Ergonomie<br />
– Evaluation der funktionellen Arbeitskapazität<br />
– Arbeitstraining<br />
– Begutachtung<br />
– Beratung<br />
❙ Knochenerkrankungen, speziell Osteoporose<br />
– Knochendichtemessung<br />
– Knochenbiopsie<br />
– Osteoporosemarker<br />
– Risikoerfassung<br />
❙ Begutachtungen für Versicherungen<br />
Anmeldung ambulante Sprechstunde<br />
Ambulante Behandlung sämtlicher Krankheiten im Bereich<br />
<strong>Rheuma</strong>tologie und Physikalische Medizin<br />
Die Anmeldung für die ambulante Sprechstunde kann nur<br />
durch einen Arzt erfolgen. Ausgenommen sind Notfälle.<br />
Telefon 044 255 26 87<br />
Fax 044 255 44 15<br />
E-mail RUZ@usz.ch<br />
Briefadresse<br />
<strong>UniversitätsSpital</strong> <strong>Zürich</strong><br />
Ärztliche Leitung<br />
<strong>Rheuma</strong>klinik und Institut für Physikalische Medizin<br />
Gloriastrasse 25, 8091 <strong>Zürich</strong><br />
Anmeldung stationärer Aufenthalt<br />
Stationäre Abklärung und Therapie-Einleitung aller rheumatischen<br />
Erkrankungen<br />
Dringende Abklärungen können telefonisch angemeldet<br />
werden<br />
Telefon 044 255 29 88<br />
Fax 044 255 89 33<br />
E-mail marie.ilktekin@usz.ch<br />
Briefadresse<br />
<strong>UniversitätsSpital</strong> <strong>Zürich</strong><br />
Ärztliche Leitung<br />
<strong>Rheuma</strong>klinik und Institut für Physikalische Medizin<br />
Gloriastrasse 25, 8091 <strong>Zürich</strong>
«Vor 6 Monaten<br />
wäre Wandern<br />
zu riskant für ihre<br />
Knochen gewesen…»<br />
HELFEN SIE IHR,<br />
DIE KNOCHEN FIT<br />
ZU HALTEN.<br />
Frauen mit Osteoporose können zu jeder Zeit<br />
und an jeder Stelle Frakturen erleiden.<br />
Nur Actonel ® schützt bereits<br />
nach 6 Monaten an den<br />
osteoporotischen Prädilektionsstellen. 1<br />
Eine frühzeitige Therapie mit Actonel ® schützt<br />
Ihre Patienten vor Frakturen und<br />
1, 2<br />
ermöglicht ihnen weiterhin ein aktives Leben.<br />
Helfen Sie ihr, die Knochen fit zu halten<br />
Kurzinformation Actonel ® : 5 mg, 30 mg Tabletten, 35 mg Wochentabletten<br />
Zusammensetzung: Na-Risedronat, Filmtabl. 5 mg, 30 mg, 35 mg. Liste B. Indikationen:<br />
Behandlung und Prävention der Osteoporose bei Frauen nach der Menopause; Behandlung und<br />
Prävention der corticosteroid-induzierten Osteoporose bei Männern und Frauen; Behandlung der<br />
Paget-Krankheit. Dosierung: Osteoporose: 1 Tabl. 5 mg/Tag oder 1 Tabl. 35 mg jede Woche;<br />
Paget: 1 Tabl. 30 mg/Tag während 2 Mt. Absorption wird durch Nahrungsaufnahme beeinflusst.<br />
Kontraindikationen: Überempfindlichkeit; Hypokalzämie; Unvermögen während 30 Minuten eine<br />
aufrechte Körperhaltung einzunehmen; schwere Niereninsuffizienz. Vorsichtsmassnahmen: Bei<br />
Oesophagusreaktionen Actonel ® absetzen und sich an den Arzt wenden; Störungen des Knochenund<br />
Mineralstoffwechsels müssen behandelt werden. Unerwünschte Wirkungen: Schmerzen im<br />
Bereich der Gelenke, Knochen und Muskeln; selten Duodenitis, Glossitis und Iritis; Verminderung<br />
derCa-,Mg-undP-Spiegel;seltenabnormeLeberfunktionswerte.Interaktionen: Die Absorption<br />
wirddurchz.B.Ca,Mg,Fe,Alreduziert.Packungen: 5mg28und84Tabl.;30mg28Tabl.;<br />
35mg4und12Tabl.Kassenzulässig. Ausführliche Informationen entnehmen Sie bitte dem<br />
Arzneimittel-Kompendium der <strong>Schweiz</strong>.<br />
Referenzen<br />
1 Boonen S. et al. Fracture protection in osteoporosis with risedronate. Hosp Med 2004: 65 (9):<br />
535-540. 2 Arzneimittel-Kompendium der <strong>Schweiz</strong>.<br />
Vertrieb: sanofi-aventis(schweiz)ag,11,ruedeVeyrot,1217Meyrin<br />
CH-RIS-07-01-02
6<br />
STATE OF THE ART<br />
Basistherapie der rheumatoiden Arthritis (RA)<br />
Die rheumatoide Arthritis (RA) ist die häufigste entzündlich-rheumatische Erkrankung. Neue Medikamente mit anti-entzündlicher<br />
Wirkung werden deshalb bevorzugt in dieser Indikation getestet und zugelassen. <strong>Das</strong> Resultat ist eine wachsende<br />
Anzahl von Basistherapeutika, die zur Behandlung von RA zugelassen worden sind oder kurz vor der Zulassung stehen.<br />
Diese Entwicklung ist für uns <strong>Rheuma</strong>tologen natürlich sehr erfreulich, erlaubt sie uns doch, in den nicht so seltenen Fällen<br />
von unbefriedigender Wirkung einer Basistherapie, wirksame Alternativen anbieten zu können. Andererseits wird die Wahl<br />
der geeigneten Basistherapie komplexer, da oft mehrere Möglichkeiten zur Auswahl stehen.<br />
Im Folgenden soll die Basistherapie einer rheumatoiden<br />
Arthritis unter Berücksichtigung neuer Erkenntnisse<br />
betrachtet werden.<br />
Frühe Diagnose und frühe Behandlung<br />
Die wahrscheinlich wichtigste Erkenntnis der vielen Studien<br />
zur «early RA» ist die Tatsache, dass ein früher Beginn einer<br />
Basistherapie zu einem langfristig besseren Verlauf mit<br />
weniger erosiv-destruktiven Veränderungen führt. Die frühe<br />
Diagnosestellung einer RA ist deshalb von zentraler Bedeutung.<br />
Wenn die Diagnose einer RA feststeht, sollte baldmöglichst<br />
eine Basistherapie begonnen werden. Selbst eine Verzögerung<br />
von wenigen Monaten kann den Therapie-Erfolg<br />
nachhaltig beeinträchtigen, wie in Studien gezeigt wurde (1, 2).<br />
Initiale Therapie<br />
Mit welchem Basistherapeutikum soll begonnen werden?<br />
Während für die gängigen konventionellen Basistherapeutika<br />
(Tabelle 1) die Wirksamkeit bei RA bewiesen worden<br />
ist, sind praktisch keine direkten Vergleichsstudien zwischen<br />
einzelnen Medikamenten durchgeführt worden. Für die Initialtherapie<br />
kommen deshalb mehrere Medikamente in Frage.<br />
In der Praxis wird in den meisten Fällen Methotrexat als<br />
erste Wahl zum Einsatz kommen, aufgrund der guten Wirksamkeit<br />
bei gleichzeitig guter langfristiger Verträglichkeit.<br />
Es ist jedoch auch der primäre Einsatz von Salazopyrin oder<br />
Leflunomid möglich oder bei milderen Verlaufsformen auch<br />
Hydroxychloroquin, das aufgrund der schwächeren Wirkung<br />
jedoch meist als Kombinationstherapie zum Einsatz kommt.<br />
Gold weist ein weniger günstiges Nebenwirkungsprofil auf<br />
und ist deshalb, wie auch Cyclosporin und Azathioprin, ein<br />
Basismedikament der zweiten Wahl.<br />
Zurzeit wird diskutiert, ob bei gewissen Patienten initial<br />
eine Kombinationstherapie begonnen werden soll. Diese Diskussion<br />
basiert auf der gut belegten Tatsache, dass mit einer<br />
intensiven initialen Basistherapie eine Remission erreicht<br />
werden kann, die zumindest mittelfristig in einer geringeren<br />
radiologischen Progression resultiert. Dies kann sowohl mit<br />
einer Kombination von konventionellen Basistherapeutika<br />
mit zusätzlich Hochdosis-Steroid-Therapie oder auch mit<br />
einem TNF-Hemmer zusätzlich zu Methotrexat erreicht werden<br />
(3). Problematisch ist bei diesem Vorgehen, dass keine<br />
verlässlichen Parameter bestehen, um die Patienten zu iden-<br />
Methotrexat (i.m./s.c./p.o.)<br />
Sulfasalazin (Salazopyrin ® )<br />
Leflunomid (Arava ® )<br />
Hydroxychloroquin (Plaquenil ® )<br />
Gold (Tauredon ® )<br />
Azathioprin (Imurek ® )<br />
Cyclosporin (Sandimmun ® )<br />
DIEGO KYBURZ<br />
Tabelle 1: Auswahl von konventionellen Basismedikamente<br />
bei RA<br />
tifizieren, die von einer aggressiven Therapie profitieren. Ein<br />
erhöhtes Risiko für einen progredienten erosiv-destruktiven<br />
Verlauf scheinen anti-CCP- und RF-positive Patienten zu<br />
haben, die bereits früh Erosionen aufweisen (4).<br />
Grundsätzlich können Biologika aufgrund der Limitatio<br />
der Kassenzulassung nach wie vor nur bei ungenügender<br />
Wirkung einer konventionellen Basistherapie angewendet<br />
werden. Konkret heisst das, dass in der Regel mit einer<br />
Monotherapie, am ehesten mit Methotrexat, begonnen wird.<br />
Sofern vom Patienten akzeptiert, wäre auch zusätzlich eine<br />
vorübergehende niedrig-dosierte Steroidtherapie in Betracht<br />
zu ziehen, da eine anti-erosive Wirkung von Steroiden nachgewiesen<br />
worden ist und damit die Zeit bis zum Eintritt der<br />
Wirkung der Basistherapie überbrückt werden kann.<br />
Therapie bei ungenügender Wirkung<br />
von Methotrexat<br />
Entsprechend der obigen Ausführungen sollte bei ungenügendem<br />
Ansprechen auf eine initiale Therapie mit Methotrexat<br />
ein rascher Therapie-Ausbau erfolgen. Dabei scheint eine<br />
Kombinationstherapie vorteilhafter zu sein als der Wechsel<br />
von einer Monotherapie zur anderen. Welche Patienten in<br />
diesem Stadium bereits einen TNF-Blocker erhalten sollten,<br />
bleibt letztendlich dem Urteil des behandelnden <strong>Rheuma</strong>tologen<br />
überlassen. Bei jüngeren Patienten mit hochtitrigem<br />
<strong>Rheuma</strong>faktor und anti-CCP-Antikörper und früh-erosivem<br />
Verlauf sollte zweifellos ein möglichst rascher Beginn einer<br />
TNF-Hemmertherapie erwogen werden. In anderen Fällen<br />
kann eine konventionelle DMARD-Kombination eingesetzt<br />
werden.
DMARD Kombination<br />
Rituximab<br />
Abatacept<br />
Schema: Basistherapie bei RA<br />
Diagnose RA<br />
Konv. DMARD<br />
DMARD + 1. TNF-Hemmer<br />
Entscheidend ist in jedem Fall, dass eine tiefe Krankheitsaktivität<br />
als Therapieziel angestrebt wird. Dies kann mit<br />
regelmässigen DAS28-Messungen verfolgt werden<br />
(DAS28�3.2). Mit einer intensiven Überwachung des<br />
Krankheitsverlaufes und Anpassung der Therapie bei residueller<br />
entzündlicher Aktivität kann auch ohne Anwendung<br />
eines TNF-Hemmers eine Remission erzielt werden (5). Studiendaten<br />
sind natürlich nicht immer für die Praxis umsetzbar.<br />
Kombinationstherapien mit zusätzlich Steroiden in<br />
hohen Dosen weisen eine beträchtliche Toxizität auf. In der<br />
Praxis wird es deshalb darum gehen, eine verträgliche Basistherapie<br />
zu finden, ohne jedoch das Ziel einer tiefen Krankheitsaktivität<br />
aus den Augen zu verlieren.<br />
Therapie bei ungenügender Wirkung<br />
von TNF-Hemmern<br />
2. TNF-Hemmer<br />
Bei Patienten, die ungenügend auf die Anwendung von<br />
TNF-Hemmer ansprechen, kommen zurzeit Rituximab und<br />
Abatacept in Frage. Für beide Medikamente wurde eine<br />
Wirkung in dieser Indikation nachgewiesen. Abatacept kann<br />
entsprechend der Limitatio auch anstelle eines TNF-Hemmers<br />
angewendet werden, jedoch ist bei limitierter Datenlage<br />
bezüglich Langzeitnebenwirkungen Vorsicht angebracht.<br />
Ob Rituximab oder Abatacept nach dem ersten oder<br />
eher nach dem zweiten oder dritten TNF-Hemmer eingesetzt<br />
werden sollte, ist noch unklar. Es gibt jedoch Hinweise<br />
aus dem SCQM RA, dass der Einsatz von Rituximab anstelle<br />
eines Versuches mit einem zweiten TNF-Hemmer vorteilhaft<br />
sein kann (6).<br />
Höchstwahrscheinlich wird 2008 zusätzlich Actemra<br />
(anti-IL-6) als weitere Option hinzukommen.Welches dieser<br />
Medikamente im Einzelfall vorzuziehen ist, kann zurzeit<br />
nicht klar definiert werden, da kaum Daten dazu erhältlich<br />
sind. Was alle bisherigen Studien aber klar gezeigt haben ist,<br />
dass Biologika nicht kombiniert werden sollten aufgrund des<br />
erhöhten Risikos für Infektionen.<br />
Ob B- oder T-Zell-gerichtete Therapien, wie Rituximab<br />
oder Abatacept, im Frühstadium einer RA eingesetzt, zu<br />
langfristigen Remissionen führen können, ist eine spannende<br />
Frage, die hoffentlich durch entsprechende Studien beantwortet<br />
wird. Bis solche mit Spannung erwartete Daten eintreffen<br />
und möglicherweise zu einem Paradigmenwechsel<br />
führen, wird die Basistherapie der RA weiterhin nach dem<br />
abgebildeten Schema durchgeführt werden.<br />
Bei allen Neuerungen wird die Zielsetzung dieselbe<br />
bleiben, den Patienten folgendes zu erhalten:<br />
❙ Schmerzlinderung<br />
❙ eine gute Gelenkfunktion und damit<br />
❙ eine möglichst uneingeschränkte Lebensqualität<br />
Literatur<br />
1 Lard LR, Visser H, Speyer I, vander Horst-<br />
Bruinsma IE, Zwinderman AH, Breedveld FC, et<br />
al.: Early versus delayed treatment in patients with<br />
recent-onset rheumatoid arthritis: comparison of<br />
two cohorts who received different treatment strategies.<br />
Am J Med 111(6):446-451, 2001.<br />
2 Nell VP, Machold KP, Eberl G, Stamm TA, Uffmann<br />
M, Smolen JS: Benefit of very early referral and<br />
very early therapy with disease-modifying anti-rheumatic<br />
drugs in patients with early rheumatoid arthritis.<br />
<strong>Rheuma</strong>tol (Oxford) 43(7):906-914, 2004.<br />
3 Goekoop-Ruiterman YP, de Vries-Bouwstra JK,<br />
Allaart CF, van Zeben D, Kerstens PJ, Hazes JM, et<br />
al.: Clinical and radiographic outcomes of four<br />
different treatment strategies in patients with early<br />
rheumatoid arthritis (the BeSt study): a randomized,<br />
controlled trial. Arthritis Rheum 52(11):3381-3390,<br />
2005.<br />
4 Combe B, Dougados M, Goupille P, Cantagrel A,<br />
Eliaou JF, Sibilia J, et al.: Prognostic factors for<br />
radiographic damage in early rheumatoid arthritis:<br />
a multiparameter prospective study. Arthritis<br />
Rheum 44(8):1736-1743, 2001.<br />
5 Grigor C, Capell H, Stirling A, McMahon AD, Lock<br />
P, Vallance R, et al.: Effect of a treatment strategy of<br />
tight control for rheumatoid arthritis (the TICORA<br />
study): a single-blind randomised controlled trial.<br />
Lancet 17-23;364(9430):263-269, 2004.<br />
6 Finckh A, Ciurea A, Brulhart L, Kyburz D, Moller B,<br />
Dehler S, et al.: B cell depletion may be more effective<br />
than switching to an alternative anti-tumor<br />
necrosis factor agent in rheumatoid arthritis patients<br />
with inadequate response to anti-tumor necrosis factor<br />
agents. Arthritis Rheum 56(5):1417-1423, 2007.<br />
45–2007<br />
7
8<br />
SCHWERPUNKT<br />
Einführung<br />
2003 wurden erstmals von zwei Autoren einige Fälle einer<br />
avaskulären Nekrose des Kieferknochens beschrieben, die<br />
nach Behandlung mit Pamidronat beziehungsweise Zoledronat,<br />
zwei intravenös verabreichten Amino-Bisphosphonaten,<br />
aufgetreten waren. Seither hat sich die Anzahl publizierter<br />
Fälle beinahe explosionsartig vervielfacht.<br />
Inzwischen haben die pharmazeutische Industrie, ärztlich-wissenschaftliche<br />
Kreise und die Gesundheitsämter<br />
zahlreiche Beurteilungen und Empfehlungen herausgegeben.<br />
Worum geht es genau und welches ist der Ursprung dieser<br />
besonderen Osteonekrose, die sich auf den Kiefer beschränkt?<br />
Wie erklärt man sich den Zusammenhang mit der<br />
Therapie mit Bisphosphonaten und wie verläuft die Erkrankung?<br />
Wie hoch ist ihre Prävalenz, wie ist ihre Prognose und<br />
wie kann man sie verhindern? Viele dieser Fragen bleiben<br />
zurzeit offen und können aktuell nicht beantwortet werden.<br />
Im Folgenden werden wir einige dieser Punkte kurz diskutieren.<br />
Definition der ONJ (Osteonecrosis of the Jaw)<br />
Von Osteonekrose spricht man bei seit mindestens acht<br />
Wochen freiliegendem Unter- und/oder Oberkieferknochen,<br />
ohne Tendenz zur Sekundärheilung, ohne vorangegangene<br />
Bestrahlung oder lokale Metastasierung. Hingegen geht der<br />
Entwicklung dieser Pathologie oft ein zahnärztlicher Eingriff<br />
voraus.<br />
Epidemiologische Daten<br />
Epidemiologisch können zwei verschiedene Gruppen unterschieden<br />
werden: einerseits Patienten, die wegen einer<br />
Osteoporose mit Bisphosphonaten behandelt werden, andererseits<br />
onkologische Patienten, die wegen Knochenmetastasen<br />
oder tumorbedingter Hyperkalzämie im Zusammenhang<br />
mit Malignomen verschiedenen Ursprungs mit Bisphosphonaten<br />
therapiert werden.<br />
DANIEL UEBELHART, DIANA FREY<br />
Kiefernekrose unter Bisphosphonaten –<br />
aktueller Wissensstand<br />
Die Problematik von Kiefernekrosen (Osteonecrosis of the Jaw: ONJ) bei Patienten, die mit Bisphosphonaten<br />
behandelt werden, ist erst in letzter Zeit ins Bewusstsein der medizinischen Welt gerückt.<br />
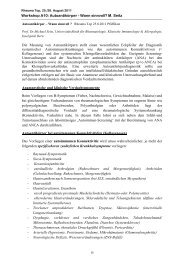
Kieferosteonekrose: Sicht auf einen nekrotischen<br />
Kieferknochen J Oral Maxillofac Surg 62:527-534, 2004<br />
a) Patienten, die wegen einer Osteoporose mit Bisphosphonaten<br />
behandelt werden<br />
Die Anzahl gemeldeter Fälle von Kiefernekrose in den letzten<br />
Jahren betrug weniger als ein Fall pro 100 000 Patienten<br />
pro Jahr. Eine ähnliche Inzidenz wurde auch in einer kürzlich<br />
untersuchten grossen Kohorte von Patienten im Rahmen<br />
des Deutschen Kiefernekrose-Registers ermittelt. Die<br />
Resultate dieser neuesten Studie wurden an den letzten<br />
nationalen und internationalen Kongressen durch das Team<br />
von D. Felsenberg des Charité-Hospitals in Berlin kommuniziert.<br />
Man kann deshalb davon ausgehen, dass auf 120 000<br />
bis 130 000 behandelte Patienten nur ein Fall von Kiefernekrose<br />
auftritt.<br />
b) Patienten, die wegen Knochenmetastasen mit Bisphosphonaten<br />
behandelt werden<br />
Bei diesen Patienten hat das Problem der Kiefernekrosen<br />
eine völlig andere Bedeutung. Im Allgemeinen erhalten<br />
diese Patienten hohe intravenöse Bisphosphonat-Dosen als<br />
adjuvante Therapie bei multiplem Myelom oder bei metastasierendem<br />
Brustkrebs. Bei solchen Patienten treten Kiefernekrosen<br />
in zirka 95 Fällen pro 100 000 Patienten pro Jahr<br />
auf. Diese Angabe muss zwar mit Vorsicht interpretiert<br />
werden, aber es scheint klar zu sein, dass das Risiko, eine<br />
Kiefernekrose unter Bisphosphonat-Behandlung wegen<br />
einer malignen Erkrankung zu entwickeln (bis zu zehn<br />
Prozent der Fälle), bedeutend höher ist als bei der Behandlung<br />
einer postmenopausalen Osteoporose.
Ätiopathogenese der Kiefernekrose<br />
Auch wenn bisher verschiedene Hypothesen zur Ätiopathogenese<br />
formuliert wurden, ist keine davon allgemein anerkannt.<br />
Eine Arbeitshypothese erwägt die Kombination verschiedener<br />
schädlicher Wirkungen der Bisphosphonate, wie<br />
beispielsweise eine übermässige Unterdrückung des Knochenmetabolismus,<br />
ein möglicherweise vermehrtes Auftreten<br />
von Mikrofrakturen in den Kieferknochen sowie eine<br />
Verminderung der Angiogenese als wahrscheinliche Ursache<br />
für Apoptose und Zelltod. In diesem Zusammenhang<br />
wurde allerdings nie bewiesen, dass die Verminderung des<br />
Knochenmetabolismus unter Bisphosphonat-Therapie zu<br />
einem adynamischen Knochen führt. Ebenso konnte bis<br />
heute kein direkter Zusammenhang zwischen Bisphosphonaten,<br />
Krebs und Kiefernekrose hergestellt werden, auch<br />
wenn die anti-angiogenetischen Auswirkungen der Bisphosphonate<br />
bekannt sind.<br />
Im Gegensatz dazu scheinen der Zustand der Mundschleimhaut<br />
und die mikrobakterielle Besiedelung der<br />
Mundhöhle bestimmende Faktoren in der Genese der Kiefernekrose<br />
zu sein.<br />
Risikofaktoren zur Entwicklung einer<br />
Kiefernekrose<br />
Bei mit Bisphosphonaten behandelten Osteoporose-Patienten<br />
stehen zu wenig Angaben zur Verfügung, um auf eventuelle<br />
spezifische Risikofaktoren für eine Kiefernekrose zu<br />
schliessen.<br />
Hingegen konnte bei den onkologischen Patienten unter<br />
Bisphosphonat-Therapie eine Anzahl Risikofaktoren identifiziert<br />
werden. Diese sind hohe Bisphosphonat-Dosen, eine<br />
langfristige Therapie, Zahnextraktionen und eine bestehende<br />
Parodontose.<br />
Es scheint, dass das Vorhandensein von Co-Morbiditäten,<br />
wie eine rheumatoide Arthritis oder ein schlecht eingestellter<br />
Diabetes mellitus, ebenso wie eine immunsuppressive<br />
Behandlung oder eine Chemotherapie, ebenfalls das<br />
Risiko erhöhen, eine Kiefernekrose zu entwickeln.<br />
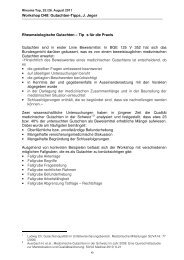
3-D-Rekonstuktion einer Nekrose nach Zahnextraktion<br />
Br J Haematol 128:738, 2005<br />
Orthopantomogramm nach Zahnextraktion (links unten).<br />
Nekrose beim Extraktionsort. J Oral Maxillofac Surg 62:527-534, 2004<br />
Demzufolge wird allgemein empfohlen, bei osteoporotischen<br />
Patienten unter Bisphosphonat-Therapie auf eine<br />
invasive Zahn- oder Mundhöhlenbehandlung, wenn immer<br />
möglich, zu verzichten, um eine Verletzung der Mundhöhle<br />
zu vermeiden. Ausserdem ist bei Patienten mit langjähriger<br />
Bisphosphonat-Therapie auf eine strikte Einhaltung der<br />
Mundhygiene zu achten.<br />
Diagnose der Kiefernekrose<br />
Die Diagnose wird aufgrund der Klinik in erster Linie durch<br />
den Zahnarzt gestellt, bei sichtbarer, direkter Freilegung des<br />
Kieferknochens (Ober- und/oder Unterkiefer) während<br />
mehr als acht Wochen, vorausgesetzt die Stelle wurde nicht<br />
einer vorherigen Bestrahlung unterworfen, die zu einer<br />
Osteonekrose nach Radiotherapie führen könnte, und die<br />
mit einer Gewebetransplantation behandelt werden müsste.<br />
Differenzialdiagnostisch muss ausserdem an Kieferknochenmetastasen<br />
sowie an eine klassische Osteomyelitis gedacht<br />
werden. Letztere müsste chirurgisch beziehungsweise antibiotisch<br />
behandelt werden.<br />
Falls durch gezielte Abklärungen andere Ursachen ausgeschlossen<br />
werden konnten, ist eine Kiefernekrose wahrscheinlich,<br />
und der Patient muss unverzüglich einem Kieferchirurgen<br />
zugewiesen werden. Nach Bestätigung der Diagnose<br />
sollte eine individuell auf die Situation des Patienten<br />
zugeschnittene Behandlung begonnen werden. Diese gestaltet<br />
sich relativ schwierig, denn im Gegensatz zu Knochennekrosen<br />
anderen Ursprungs ist diese Art Knochennekrose<br />
normalerweise schlecht behandelbar und der Heilungsprozess<br />
langwierig.<br />
Allgemeine Richtlinien zur Behandlung<br />
Osteoporotische Patienten ohne zusätzliche Begleiterkrankungen<br />
und -medikamente, die eine Bisphosphonat-Behandlung<br />
beginnen, sollten auf ihre Mundhygiene achten und<br />
regelmässige zahnärztliche Kontrollen durchführen lassen.<br />
Wenn eine Zahn- oder Kieferbehandlung bei einem<br />
bereits unter Bisphosphonaten stehenden Patienten notwendig<br />
wird und der Patient ausserdem Risikofaktoren wie<br />
45–2007<br />
9
10<br />
CT der Mandibula mit Osteolysen<br />
einen Diabetes mellitus oder eine chronische Steroidtherapie<br />
aufweist, sollten regelmässige zahnärztliche Nachkontrollen<br />
vorgesehen und die Mundhöhle täglich mit desinfizierenden<br />
Produkten gespült sowie eine angepasste Antibiotika-Prophylaxe<br />
durchgeführt werden. Dies ist speziell<br />
wichtig bei onkologischen Patienten, deren zahnärztliche<br />
Behandlung möglichst vor Beginn einer Bisphosphonat-<br />
Therapie durchgeführt werden sollte.<br />
Hingegen besteht kein rationaler Grund, während einer<br />
zahnärztlichen Behandlung die Verabreichung von Bisphosphonaten<br />
zu sistieren, um das Risiko einer Kiefernekrose zu<br />
senken.<br />
Die Kiefernekrose-Behandlung unter Bisphosphonaten,<br />
insbesondere bei onkologischen Patienten, bleibt exklusiv<br />
dem Kieferchirurgen vorbehalten, auch wenn bisher bei keinem<br />
therapeutischen Ansatz die Wirksamkeit bewiesen werden<br />
konnte und deshalb dieses Kapitel ebenfalls noch offen<br />
bleibt.<br />
«Take home message»<br />
J Oral Maxillofac Surg 62:527-534, 2004<br />
❙ <strong>Das</strong> Auftreten einer Kiefernekrose unter Bisphosphonaten<br />
ist bei osteoporotischen Patienten äusserst selten,<br />
während sie bei onkologischen Patienten unter dieser<br />
Behandlung viel öfters vorkommt.<br />
❙ Die Pathogenese dieser Kiefernekrose ist zurzeit nicht<br />
bekannt, wohl aber einige Risikofaktoren, die ihr Auftreten<br />
begünstigen können.<br />
❙ Die wichtigsten Risikofaktoren sind eine schlechte Mundhygiene<br />
mit lokaler bakterieller Besiedelung, Zahnextraktionen,<br />
Zahnimplantate oder Schädigung der<br />
Mundhöhle und der Kiefer.<br />
❙ Die Diagnose wird in erster Linie klinisch gestellt und<br />
durch einen spezialisierten Zahnarzt oder Kieferchirurgen<br />
bestätigt.<br />
❙ Wichtige Differenzialdiagnosen sind unter anderem<br />
Osteomyelitis, Metastasen und Nekrosen nach Radiotherapie.<br />
❙ Die Behandlung ist wegen schlechter Heilungstendenz<br />
aufwendig und langwierig und sollte individuell auf den<br />
Patienten abgestimmt sein.<br />
❙ Die seit Jahren in der Prävention oder Behandlung der<br />
postmenopausalen Osteoporose und der Tumortherapie<br />
eingesetzten oral oder intravenös verabreichten<br />
Bisphosphonate sind Substanzen, die gleichzeitig sehr<br />
wirksam und in der grossen Mehrzahl der Fälle gut verträglich<br />
sind.<br />
Kontakt<br />
PD Dr. med. Daniel Uebelhart, LA<br />
<strong>Rheuma</strong>klinik und Institut für Physikalische Medizin<br />
OsteoporoseZentrum<br />
<strong>UniversitätsSpital</strong> <strong>Zürich</strong><br />
Gloriastrasse 25, 8091 <strong>Zürich</strong><br />
e-mail: daniel.uebelhart@usz.ch<br />
Frau Dr. med. Diana Frey, OA<br />
<strong>Rheuma</strong>klinik und Institut für Physikalische Medizin<br />
Clinical Trials<br />
<strong>UniversitätsSpital</strong> <strong>Zürich</strong><br />
Gloriastrasse 25, 8091 <strong>Zürich</strong><br />
Literatur<br />
1 Marx RE et al.: Pamidronate (Aredia) and<br />
Zoledronate (Zometa) induced avascular necrosis<br />
of the jaws: a growing epidemic. J Oral Maxillofac<br />
Surg 61:1115-1118, 2003.<br />
2 Robertson A et al.: Ostéonécrose maxillaire due aux<br />
bisphosphonates: recommendations diagnostiques et<br />
thérapeutiques. Forum Med Suisse 7:408-412, 2007.<br />
3 Khosla S et al.: Bisphosphonate-associated<br />
osteonecrosis of the jaw: report of a task force of<br />
the ASBMR. J Bone Miner Res 22:1479-1491, 2007.<br />
4 Yarom N et al.: Osteonecrosis of the jaw induced by<br />
orally administered bisphosphonates: incidence,<br />
clinical features, predisposing factors and treatment<br />
outcome. Osteoporos Int 18:1363-1370, 2007.<br />
5 Jung TI et al.: Osteonecrosis of the jaw under<br />
bisphosphonate therapy – A german register for<br />
patients with osteonecrosis of the jaw. Osteoporos<br />
Int 18:S8, 2007.<br />
6 Von Moos R.: Bisphosphonate treatment recommendations<br />
for oncologists. The Oncologist 10<br />
(Suppl.1):19-24, 2005.<br />
7 Ruggiero S et al.: Practical guidelines for the<br />
prevention, diagnosis, and treatment of osteonecrosis<br />
of the jaw in patients with cancer. J Oncology<br />
Practice 2:7-14, 2006.
ACR 2007<br />
STEFFEN GAY<br />
Im letzten Heft (<strong>Rheuma</strong>-Nachrichten Vol. 44) haben wir Sie in ein neues Forschungsgebiet eingeführt. Nachdem das menschliche<br />
Genom sequenziert wurde, widmet man sich jetzt der Regulation der bestimmten Genfrequenzen. Diese Regulation, die man<br />
auch «Epigenetics» nennt, bedient sich unter anderem kleiner RNA-Sequenzen, die man als «microRNA» beziehungsweise «miRNA»<br />
bezeichnet. Eines der State of the Art-Lectures zum diesjährigen ACR-Meeting in Boston, MA, wurde vom Nobelpreisträger<br />
Philip A. Sharp gehalten und dabei genau die immer wichtiger werdende Rolle dieser miRNA in normalen und pathologischen<br />
Entwicklungsprozessen in den Mittelpunkt gestellt.<br />
<strong>Das</strong> Zentrum für Experimentelle <strong>Rheuma</strong>tologie beschäftigt<br />
sich seit zwei Jahren mit der Rolle von miRNA bei der <strong>Rheuma</strong>toiden<br />
Arthritis (RA). Somit konnte Joanna Stanczyk,<br />
MD, PhD, in ihrer «oral presentation» über die Rolle von<br />
miRNA 145 und 155 berichten.<br />
Ebenfalls konnte Emmanuel Karouzakis, PhD Student, der<br />
unter Anleitung von Dr. Michel Neidhart in unserem Zentrum<br />
arbeitet, in einer weiteren «oral presentation» über<br />
einen anderen epigenetischen Mechanismus in der Pathogenese<br />
der RA sprechen. Diese Arbeiten konnten zeigen,<br />
dass aggressive Fibroblasten in RA demethylierte Sequenzen<br />
aufweisen, die zur Re-Expression von bestimmten endogenen<br />
retroviralen Sequenzen in diesen Zellen führen, und<br />
damit für ihre endogene Aktivierung verantwortlich sind.<br />
Weiterhin erklärten Jörg Distler, MD, und Falk Moritz, MD,<br />
in je einer «oral presentation» neue Erkenntnisse zur Pathogenese<br />
der Systemischen Sklerose (Sklerodermie).<br />
Andere zwölf Posters dokumentierten die Rolle von weiteren<br />
epigenetischen Prozessen der Acetylierung, der Zellaktivierung<br />
durch Fibrin sowie von neuen Zytokinen, Adipokinen<br />
und Chemokinen.<br />
Es war uns eine besondere Freude, dass alle Abstracts unseres<br />
Zentrums angenommen wurden.<br />
01<br />
THE ADIPOKINE VISFATIN AND ITS INFLUENCE ON THE<br />
INFLAMMATORY STATE IN RHEUMATOID ARTHRITIS<br />
Florian MP Meier 1 , Anette Knedla 1 , Stephanie Lefèvre 1 , Klaus Frommer 1 ,<br />
Andreas Schäffler 2 , Christa Büchler 2 , Jürgen Steinmeyer 3 , Henning Stürz 4 , Steffen<br />
Gay 5 , Ulf Müller-Ladner 1 , Elena Neumann 1 .<br />
1 Dept Int Med and <strong>Rheuma</strong>tology, Justus-Liebig-University of Gießen, Bad<br />
Nauheim, Germany; 2 Internal Med I, University of Regensburg, Regensburg,<br />
Germany; 3 Dept Exp Orthopedics, Justus-Liebig-University Gießen, Gießen,<br />
Germany; 4 Dept Orthopedics, Justus-Liebig-University Gießen, Gießen, Germany;<br />
5 Ctr Exp <strong>Rheuma</strong>tology, USZ, <strong>Zürich</strong>, Switzerland<br />
Objective: Influencing a variety of processes including metabolism, atherosclerosis<br />
and inflammation multifunctional adipokines such as adiponectin became<br />
a subject of major interest.Visfatin, a recently discovered adipokine, is inducible<br />
via trans-signaling through IL-6 in synovial fibroblasts (SF) of patients suffering<br />
rheumatoid arthritis (RA). Further cellular lifespan is extended by the enzymatic<br />
function of visfatin as nicotinamide phosphoribosyltransferase. Hence, we<br />
investigated whether visfatin plays a role in the pathogenesis of RA specifically<br />
in joint destruction and contribution to the inflammatory process.<br />
Methods: Visfatin concentrations in synovial fluid of RA, osteoarthritis (OA)<br />
and psoriatic arthritis patients were detected by ELISA and correlations to<br />
BMI, CRP and ESR were determined. Visfatin expression and localization was<br />
determined in RA and OA synovial tissues by immunohistochemistry. Isolation<br />
and cell culture of RASF and OASF was performed using standard protocols.<br />
RASF and OASF were stimulated with different concentrations of visfatin<br />
(between 2.5 to 10000 ng/ml) using adiponectin (25 µg/ml) as positive control.<br />
Supernatants were used to perform a cytokine and chemokine antibody array.<br />
Afterwards they were investigated by ELISA measuring the production of<br />
cytokines and matrix remodelling enzymes (IL-1beta, TNF-alpha, IL-6, IL-8,<br />
pro-MMP-1, MMP-3, activin A, follistatin, MCP-1, TIMP-1, TIMP-2).<br />
Results: Visfatin was correlated positively to CRP, but not to ESR or BMI. The<br />
mean concentration of visfatin in RA synovial fluid was 77.1 ng/ml.Visfatin was<br />
predominantly expressed in the lining layer, lymphoid aggregates and in<br />
endothelial cells of capillaries. Furthermore, visfatin induced in a dose-dependent<br />
manner the synthesis of IL-6, IL-8, pro-MMP-1, MMP-3 and activin a in<br />
RASF. Interestingly, a strong induction of IL-6, IL-8, activin A, MCP-1, MMP-3<br />
and pro-MMP-1 in RASF (6.1-, 51.3-, 1.4-, 3.3-, 3.6-, 1.2-fold) and OASF (6.3-,<br />
56.3-, 2.2-, 3.3-, 6.4-, 2.2-fold) was measured when using physiological visfatin<br />
concentrations.<br />
Conclusions: In comparison to adiponectin, visfatin appears to be more prominently<br />
expressed in inflamed arthritic tissue. As visfatin exerted also strong<br />
stimulatory effects on proinflammatory and matrix-degrading enzymes, the<br />
data support the idea that visfatin is a highly potent molecule in the pathophysiology<br />
of RA.<br />
02<br />
DESUMOYLATION DECREASES LEVELS OF HISTONE ACETYLATION<br />
IN RHEUMATOID ARTHRITIS SYNOVIAL FIBROBLASTS<br />
Hanna Maciejewska 1 , Hossein Hemmatazad 1 , Renate E. Gay1, Beat Michel 1 ,<br />
Michel Neidhart 1 , Christoph Kolling 2 , Steffen Gay1,Thomas Pap 3 ,Astrid Juengel 1 .<br />
1 University Hospital, Zurich, Switzerland; 2 Schulthess Clinic, Zurich, Switzerland;<br />
3 University Hospital, Munster, Germany<br />
Purpose: Previously, we could show the small ubiquitin-like modifier 1<br />
(SUMO1) to be overexpressed in rheumatoid arthritis (RA) synovium and<br />
demonstrated the contribution of SUMO1 to the resistance of RA synovial<br />
fibroblasts (RASF) to FasL induced apoptosis as well as to their increased production<br />
of matrix metalloproteinases (MMP) (MMP1, 3, 9 and 13) and inflammatory<br />
cytokines (IL-6). This work addresses the question whether desumoylation<br />
by the SUMO specific protease SENP1 might influence gene expression by<br />
decreasing levels of histone acetylation, which is associated with the repression<br />
of genes.<br />
Methods: Synovial fibroblasts were obtained from patients with RA undergoing<br />
surgical procedures (n=6). All RA patients fulfilled the ACR criteria. RASF<br />
from passages 4-6 were used for transfection with SENP1-GFP or mock transfected<br />
(vector with GFP only) by AMAXA nucleotransfection.<br />
For immunofluorescence, transfected cells were fixed after 48h with 4%<br />
paraformaldehyde and permeabilized with 0.1% Triton in PBS for 10 minutes.To<br />
assess the global histone acetylation, cells were incubated with anti-acetyl-histone<br />
H4 antibodies (Upstate) and next with CyTM3 goat anti-rabbit antibodies<br />
(Jackson ImmunoResearch) for analysis with the fluorescence microscope.<br />
To perform flow cytometry SENP1 transfected cells and mock transfected cells<br />
were cultured for 48h, fixed with Cytofix (BD) and permeabilized with 0.4%<br />
Triton. Cells were stained with anti-acetyl-histone H4 antibodies followed by<br />
R-PE donkey anti-rabbit antibodies (Jackson ImmunoResearch).<br />
Results: RASF could be successfully transfected with SENP1-GFP or mock<br />
transfected as shown by immunofluorescence and FACS analysis. Transfection<br />
45–2007<br />
KONGRESS<br />
11
12<br />
efficiency determined by flow cytometry was in the range of 25-70%.Visualised<br />
by immunofluorescence, RASF transfected with SENP1-GFP revealed lowered<br />
levels of acetylated histone H4 when compared both to nontransfected as<br />
well as GFP transfected cells (n=3). Using flow cytometry analysis we could<br />
further confirm that the levels of H4 acetylation were significantly decreased<br />
by 40% when compared to nontransfected cells (n=3) (p
elated with the expression of LINE-1 ORF1p in the respective synovial tissues<br />
(r = 0.83, p< 0.05, by sequencing 6 RA and 1 OA clones in a total of 7 patients).<br />
Most important, the promoter methylation array showed that genes coding for<br />
maspin, talin and interferon regulatory factor 7 (IRF7) were hypomethylated<br />
in RA-SF, in comparison to normal SF (55-58% RA-SF and 100% normal SF).<br />
In contrast, 7 out of 83 gene promoters were methylated in both RA-SF and<br />
normal SF, whereas hypomethylated genes in both cell types included p16, p21,<br />
Ras, MLH1, E-cadherin, MGMT, TIMP-3 and COX-2.<br />
Conclusion: These results clearly show that global hypomethylation occurs in<br />
RA synovial tissues and especially in RA-SF. The specific hypomethylation of<br />
maspin, a novel serine protease inhibitor, talin, a cytoskeletal protein, and<br />
IRF7, a regulator of interferon genes, may contribute to the activated phenotype<br />
of RA-SF and their aggressive behaviour.<br />
06<br />
FIBRIN PROMOTES INVASIVENESS OF RHEUMATOID ARTHRITIS<br />
SYNOVIAL FIBROBLASTS BY THE INDUCTION OF MATRIX<br />
METALLOPROTEINASES 1 AND 3<br />
Olga Sanchez-Pernaute 1 , Emmanuel Karouzakis 1 , Astrid Juengel 1 , Peter Kuenzler<br />
1 , Renate E. Gay 1 , Christoph Kolling 2 , Gabriel Herrero-Beaumont 3 , Steffen<br />
Gay 1 , Michel Neidhart 1 .<br />
1 Center of Experimental <strong>Rheuma</strong>tology, University Hospital, Zurich, Switzerland;<br />
2 Department of Orthopedic Surgery, Schulthess Klinik, Zurich, Switzerland;<br />
3 <strong>Rheuma</strong>tology Section, Fundacion Jimenez Di¬az, Madrid, Spain<br />
Purpose: Fibrin has been identified as a major autoantigen in rheumatoid<br />
arthritis (RA) as a result of its citrullination inside joints. We have previously<br />
hypothesized that fibrin could account not only for autoimmunity but also for<br />
the destructive behaviour of RA synovial cells. Our aim in the present work<br />
was to study the expression of the matrix metalloproteinases (MMP)1 and 3 in<br />
synovial fibroblasts upon stimulation with fibrin.<br />
Methods: Synovial fibroblasts from patients with RA (RASF) or osteoarthritis<br />
(OASF) were cultured and stimulated with fibrin freshly clotted by adding 0.75<br />
U/ml thrombin to 1 mg/ml purified fibrinogen. The gene expression of MMP1,<br />
MMP3 and the alpha 5 integrin chain were determined by real-time PCR. By<br />
immunoblotting, we studied the appearance of pro- and active MMP1 and<br />
MMP3, as well as levels of the mitogen activated kinase p38 (phosphorylated<br />
and non phosphorylated isoforms) in RASF exposed to fibrin at different time<br />
points. Co-localisation studies of fibrin and MMP1 and 3 were performed in<br />
synovial specimens from RA patients by immunohistochemistry.<br />
Results: In cultured RASF, a 12 h stimulation with fibrin resulted in a 23-fold<br />
increase of the gene expression of MMP1 (n = 4, p < 0.03) and a 27-fold<br />
increase of the gene expression of MMP3 (n = 4, p < 0.03). A slight induction<br />
was also found in OASF, although it was only significant for the MMP3 mRNA<br />
(2-fold up-regulation, n = 4, p < 0.03). The alpha 5 integrin chain, which acts as<br />
receptor for several extracellular matrix proteins, was found up-regulated in<br />
RASF (1.8-fold, p < 0.03) but not in OASF. An increase in MMP1 protein levels<br />
followed fibrin treatment in RASF, peaking at 18 h (4-fold and 11-fold for<br />
latent and active isoforms, respectively), while the release of MMP3 to supernatants<br />
was 2-fold increased at 18 h of treatment compared to untreated RASF.<br />
Additionally, phosphorylation of p38 was observed between 1 h to 4 h of exposure<br />
to fibrin. In rheumatoid synovial tissues, interstitial immune-reactivity to<br />
both MMP1 and 3 was associated to fibrin deposits and both proteases colocalised<br />
with fibrin at the invasive interfaces. Fibroblast-like cells in fibrin-rich<br />
areas depicted a strong immune-reactivity to MMP1 and MMP3.<br />
Conclusion: Our observations support a role for fibrin in the aggressive potential<br />
of RASF, suggesting that these cells are stimulated by fibrin to enhance<br />
their production of proteases that mediate the destruction of cartilage and<br />
bone in RA. The selective up-regulation of the alpha 5 integrin observed in<br />
RASF, points to this molecule as a candidate receptor for the transduction of<br />
fibrin-dependent invasive signals in RASF.<br />
07<br />
PRODUCTION OF MATRIX METALLOPROTEINASES IN<br />
RHEUMATOID ARTHRITIS IS REGULATED BY<br />
PHOSPHATIDYLINOSITOL 3-KINASE GAMMA<br />
Noreen Pundt 1 , Marvin A. Peters 1 , Inga Kühnel 1 , Christina Wunrau 1 , Katja<br />
Neugebauer 1 , Lars H. Meyer 1 , Georg Schett 2 , Silvia Hayer 3 , Anja Baier 4 , Tzvetanka<br />
Bondeva 5 , Steffen Gay 6 ,Thomas Ruekle 7 , Montserrat Camps 7 , Matthias K.<br />
Schwarz 7 , Christian Rommel 7 , Reinhard Wetzker 5 , Thomas Pap 1 .<br />
1 University Hospital Muenster, Muenster, Germany; 2 University Hospital<br />
Erlangen, Erlangen, Germany; 3 University Vienna, Vienna, Austria; 4 University<br />
Hospital Magdeburg, Magdeburg, Germany; 5 University Hospital Jena, Jena,<br />
Germany; 6 University Hospital Zurich, Zurich, Austria; 7 Serono Pharm Res<br />
Inst., Geneva, Switzerland<br />
Purpose: We analyzed the expression of the gamma isoform of PI3K in synovial<br />
fibroblasts from patient with RA (RASF) and OA (OASF). Further we<br />
investigated the effects of PI3K� on EGF induced Akt-phosphorylation and<br />
MMP expression as well as on the invasive behaviour of RASF and synovial<br />
fibroblasts from hTNFtg mice.<br />
METHODS: RASF and OASF were analyzed for the expression of mRNA for<br />
the catalytic p110 and regulatory p101 subunit of PI3K� by PCR and western<br />
blot. The involvement of PI3K� in Akt-phoshorylation was studied in EGFstimulated<br />
cells (10-100 ng/ml, 5 min) using the pan-PI3K-inhibitor LY294992<br />
(200-500ng/ml) and a PI3KÁ specific inhibitor AS-252424 (50-100 mM). The<br />
expression of MMP-1 and MMP-3 was studied by ELISA following stimulation<br />
of synovial fibroblasts with EGF (10 ng/ml, 24 h). The invasive behaviour of<br />
EGF-stimulated RASF treated with AS-252424 was investigated using transepithelial<br />
resistant assay (TEER). Synovial Fibroblasts from hTNFtg mice<br />
crossed into PI3K�-/- mice were used to confirm these data in an animal model<br />
of RA.<br />
RESULTS: PCR and Western blot revealed the expression of p110 catalytic<br />
subunit of PI3K� but not of the regulatory p101 subunit in RASF. OASF<br />
showed only negligible levels of p110. Stimulation of RASF and OASF resulted<br />
in the phosphorylation of Akt with LY294002 inhibiting completely the<br />
EGF-mediated activation.AS-252424 reduced the EGF-stimulated phosphorylation<br />
of Akt in RASF but had no effect in OASF. Treatment of RASF with<br />
both LY294002 and AS-252424 significantly reduced the EGF-mediated induction<br />
of MMP-1 (63% and 42%, respectively) and MMP-3 (20% and 40%,<br />
respectively). Similarly, fibroblast from hTNFtg mice expressed significantly<br />
more MMP-3 than fibroblasts from hTNFtg/PI3K�-/- mice. As determined by<br />
TEER assay, AS-252424 significantly inhibited the invasive behaviour of<br />
RASF.<br />
CONCLUSIONS: These data suggest a disease-specific expression of PI3K� in<br />
RASF that contribute to EGF-mediated phosphorylation of Akt, induction of<br />
MMP-1 and MMP-3 and subsequent decreased invasive phenotype. Therefore<br />
specific inhibitors of PI3K� may be a possibility to interfere with the activation<br />
of RASF and to reduce cartilage destruction in RA.<br />
08<br />
THE NOVEL CHEMOKINE RECEPTOR CXCR7 IS EXPRESSED<br />
IN RHEUMATOID ARTHRITIS SYNOVIUM<br />
Yvonne Y. Rengel Colina 1 , Renate E. Gay 1 , Christoph Kolling 2 , Beat A. Michel 1 ,<br />
Steffen Gay 1 , Caroline Ospelt 1<br />
1 Center of Experimental <strong>Rheuma</strong>tology, University Hospital Zurich and<br />
Zurich Center of Integrative Human Physiology (ZIHP), Zurich, Switzerland;<br />
2 Schulthess Clinic, Zurich Switzerland, Zurich, Switzerland<br />
Purpose: In rheumatoid arthritis (RA), the chemokine stromal cell-derived<br />
factor (SDF-1), also known as chemokine ligand 12 (CXCL12), has been related<br />
to cell recruitment, angiogenesis, proliferation, and to the production of<br />
matrix metalloproteinases by synovial fibroblasts (SF). It was generally<br />
believed that SDF-1 mediates these diverse processes via a single cell surface<br />
receptor known as chemokine receptor 4 (CXCR4). Recently, an alternative<br />
receptor for CXCL12 has been discovered in tumor cell lines, the chemokine<br />
receptor CXCR7. We analyzed the expression and regulation of CXCR7 in tissues<br />
from RA patients and RA synovial fibroblasts (RASF).<br />
Methods: Immunohistochemistry and Western blot with rabbit anti-human<br />
CXCR7 antibodies were used to detect the expression of CXCR7 protein in<br />
RA and osteoarthritis (OA) synovial tissues. To assay the expression of<br />
CXCR7 in synovial fibroblasts and macrophages, we performed a double staining<br />
with rabbit anti-human CXCR7 antibodies and mouse anti-vimentin or<br />
mouse anti-CD68 antibodies. The role of IL-1� (1ng/ml), TNF-� (10ng/ml) and<br />
TGF-� (10ng/ml) in the regulation of the expression of CXCR7 were analyzed<br />
by Real-time PCR (6, 12, 24h of stimulation) and Western blot (24 and 48h of<br />
stimulation). The expression of CXCR7 at protein level was measured by densitometry<br />
and a ratio CXCR7/·-tubulin was calculated.<br />
Results: By immunohistochemistry (4 RA, 3 OA), we demonstrate that<br />
CXCR7 is expressed in RA and OA synovium. RA synovial tissues exhibit a<br />
moderate to high expression of CXCR7, with a preferred localization in the lining<br />
layer. In contrast, OA samples showed a much weaker expression. However,<br />
around blood vessel, RA and OA samples showed a similar intensity of<br />
CXCR7. Double staining with vimentin and CD68 revealed that CXCR7 is<br />
45–2007<br />
13
14<br />
expressed in both vimentin and CD68 positive cells. Western blot analysis confirmed<br />
that CXCR7 is more abundant in RA samples than in OA (ratio<br />
CXCR7/·-tubulin: 0.81± 0.57 SEM vs 0.34± 0.17 SEM, n=4 each). After stimulation<br />
of cultured RASF (n=4) with Il-1�, TNF-� and TGF-�, there were no significant<br />
changes in the expression of CXCR7 mRNA and protein in all the<br />
measured timepoints.<br />
Conclusions: The discovery of the alternative receptor CXCR7, opened a new<br />
field in the study of CXCL12 pathways. This is the first time that the chemokine<br />
receptor CXCR7 is described in synovial tissue and fibroblasts of RA patients.<br />
Based on this data, we suggest that the upregulation of CXCR7 in RA is not<br />
driven by cytokines like IL-1�, TNF-� and TGF-�, but possibly by alternative<br />
mechanisms like epigenetic modulations.<br />
09<br />
LONG DISTANCE MIGRATION OF RASF: ROLE OF EXTRACELLULAR<br />
MATRIX<br />
Stephanie Lefèvre 1 , Anette Knedla 1 , Christoph Tennie 1 , Ingo H. Tarner 1 , Henning<br />
Stürz 2 , Jürgen Steinmeyer 3 , Steffen Gay 4 , Ulf Müller-Ladner 1 , Elena Neumann 1 .<br />
1 Internal Med and <strong>Rheuma</strong>tology, Justus-Liebig-University of Gießen, Bad<br />
Nauheim, Germany; 2 Dept Orthopedics and Orthopedic Surgery, Justus-Liebig-<br />
University of Gießen, Gießen, Germany; 3 Dept Orthopedics and Exp Orthopedics,<br />
Justus-Liebig-University of Gießen, Gießen, Germany; 4 Ctr Exp <strong>Rheuma</strong>tology,<br />
USZ, <strong>Zürich</strong>, Switzerland<br />
Background: Key players in rheumatoid arthritis (RA) pathophysiology are<br />
activated synovial fibroblasts (SF) which actively attach to, invade into and<br />
degrade cartilage which can be simulated in the SCID mouse model of RA. In<br />
preliminary experiments, we could show that RASF are able to migrate from a<br />
primary implantation site to a distant one, mainly via the blood stream. Therefore,<br />
the route of migration and the role of the extracellular matrix (ECM) were<br />
further analyzed in this study.<br />
Methods: Healthy human cartilage was implanted into SCID mice together<br />
with RASF. At the contralateral flank, cartilage without cells was implanted. In<br />
addition, RASF were injected intravenously (iv), subcutaneously (sc) or<br />
intraperitoneally (ip) 14 days after cartilage implantation. To evaluate the role<br />
of the ECM towards the migratory behavior of RASF, complete RA synovium,<br />
bovine cartilage or necrotic cartilage, respectively, and contralaterally normal<br />
human cartilage were implanted. After 60 days, implants, organs, blood, murine<br />
ear cartilage and joints were removed. To detect human cells, species-specific<br />
immunohisto- and -cytochemistry were performed.<br />
Results: RASF were not only able to invade and degrade cartilage which was<br />
inserted simultaneously with RASF, they also migrated to and invaded into the<br />
contralateral cartilage (Scores: inv 2.3±0.8 and 1.9±0.9, deg 1.8±0.8 and 1.6±0.6).<br />
Injection of cells led to strong destruction of the implanted cartilage, particularly<br />
after sc and iv application. Interestingly, implantation of complete synovial<br />
tissue, containing ECM and other cell types, led to migration of RASF to the<br />
contralateral cartilage in 5/11 animals (inv 2.0±1.0, deg 2.3±0.4). Single RASF<br />
were able to invade bovine and human necrotic cartilage and they could also be<br />
found in the murine ear and joint, but no invasion and degradation could be<br />
detected at day 60 after RASF application. Conclusions: RASF have the ability<br />
to migrate from a primary implant of cartilage or RA synovium to the contralateral<br />
implantation site via the blood stream and to mediate cartilage degradation.<br />
The cells are also able to cross the peritoneum after ip injection. Cartilage<br />
degradation appears to be independent of chondrocyte viability and of<br />
species background since RASF invade necrotic human as well as bovine cartilage.Therefore,<br />
the exposure to cartilage matrix, e. g. after microinjuries, may be<br />
sufficient for RASF to attach to the cartilage, to initiate destruction and spread<br />
RA from one joint to another.<br />
10<br />
FIBRIN TRIGGERS AN INNATE IMMUNE RESPONSE IN RHEUMA-<br />
TOID ARTHRITIS SYNOVIAL FIBROBLASTS ACTING AS AN ENDOGE-<br />
NOUS LIGAND OF TOLL LIKE RECEPTOR<br />
Olga Sanchez-Pernaute 1 , Fabia Brentano1, Caroline Ospelt 1 , Christoph Kolling 2 ,<br />
Beat A. Michel 1 , Renate E. Gay 1 , Gabriel Herrero-Beaumont 3 , Steffen Gay 1 ,<br />
Michel Neidhart 1 .<br />
1 Center of Experimental <strong>Rheuma</strong>tology, University Hospital and Zurich Center<br />
for Integrative Human Physiology (ZIHP), Zurich, Switzerland;<br />
2 Orthopaedic Surgery, Schulthess Klinic, Zurich, Switzerland; 3 <strong>Rheuma</strong>tology<br />
Section, Fundacion Jimenez Diaz, Madrid, Spain<br />
Purpose: The deposition of fibrin inside joints is followed by its citrullination<br />
and has been associated with the perpetuation of rheumatoid arthritis (RA)<br />
through the development of a specific immune response. In macrophages, fibrin(ogen)<br />
has been shown to be a ligand of Toll-like receptor 4 (TLR4). Since<br />
RA synovial fibroblasts (RASF) express functional TLR4, we investigated the<br />
role of fibrin in the activation of RASF as well as the effect of citrullination on<br />
the cellular response.<br />
Methods: Isolated RASF obtained from surgical explants were used for the<br />
experiments. Fibrin was polymerized in situ by the addition of 0.7 U/ml thrombin<br />
to 0.8 mg/ml fibrinogen. Citrullination was performed by adding 2.84 U/ml<br />
peptidylarginine deiminase 2 to the components of the clot. Differential gene<br />
expression was analysed using cDNA arrays (Affymetrix GeneChip ® ) and<br />
mRNA isolated from RASF, alone or with fibrin, native or citrullinated, after<br />
an incubation period of 18h. The transcripts induced by native or citrullinated<br />
fibrin were compared with the untreated RASF, establishing a bidirectional<br />
2-fold filter and merging results from two experiments. Quantitative real time<br />
PCR using SYBR green was employed to confirm the up-regulation of selected<br />
genes by native or citrullinated fibrin in additional cultures of RASF.<br />
Results: The cDNA arrays showed that the exposure of RASF to fibrin resulted<br />
in the up-regulation of genes participating in the innate response and relevant<br />
to the pathogenesis of RA, including the pro-inflammatory cytokine IL-6,<br />
the chemokines IL-8, CXCL1 and CCL2, the TNF· induced peptide 3 and the<br />
adhesion molecule ICAM-1. These inductions were observed with both native<br />
and citrullinated fibrin. Quantitative real time PCR confirmed the up-regulation,<br />
after incubation with fibrin, of IL-8 (959 ± 418 fold), CXCL1 (98 ± 37<br />
fold), IL-6 (22 ± 11 fold), COX-2 (21 ± 6 fold) and CCL2 (14 ± 3 fold) (n = 3<br />
RASF, mean ± SEM). Interestingly, compared to native fibrin, citrullinated fibrin<br />
revealed an even stronger effect on the induction of IL-8.The up-regulation<br />
of COX-2, CXCL1 and IL-8 induced by fibrin was suppressed by 70% after 2h<br />
preincubation of RASF with TLR4 blocking monoclonal antibodies (HTA125,<br />
10 mg/ml, Abcam).<br />
Conclusion: Fibrin and in particular its citrullinated form can trigger an innate<br />
immune response in RASF through a TLR4 dependent pathway. Based on<br />
these data, it can be concluded that fibrin contributes significantly to sustain<br />
the inflammatory process in RA.<br />
11<br />
DIFFERENTIAL INDUCTION OF IL-23 SUBUNITS BY TLR LIGANDS<br />
IN RHEUMATOID ARTHRITIS SYNOVIAL FIBROBLASTS AND<br />
MONOCYTES<br />
Fabia Brentano 1 , Caroline Ospelt 1 , Joanna Stanczyk 1 , Renate E. Gay 1 , Christoph<br />
Kolling 2 , Steffen Gay 1 , Diego Kyburz 1 .<br />
1 Center of Experimental <strong>Rheuma</strong>tology and Zurich Center of Integrative<br />
Human Physiology (ZIHP), University Hospital of Zurich, Switzerland;<br />
2 Schulthess Clinic, Zurich, Switzerland<br />
Purpose: IL-23 was found to have key roles in autoimmune diseases. We analyzed<br />
the expression of IL-23 in rheumatoid arthritis (RA) and osteoarthritis<br />
(OA) synovial tissues. Furthermore we studied the induction of both subunits<br />
of IL-23, p19 and p40, in cultured RA synovial fibroblasts (RASF) and monocytes<br />
after the activation of TLR2, 3 and 4.<br />
Methods: Expression of p19 and p40 was analyzed in synovial tissues by in situ<br />
hybridization (n=3) and immunohistochemistry (n=6). RASF and blood monocytes<br />
from healthy donors were stimulated with bacterial lipoprotein (bLP),<br />
poly(I-C) (PIC) and lipopolysaccharide (LPS) for 24h (n=4). The expression of<br />
p19 and p40 mRNA was analyzed by RT-PCR as well as by Real-time PCR. To<br />
detect IL-23 in supernatants of RASF and monocytes a bioassay was performed:<br />
MACS sorted CD8+ T-cells were preactivated with anti-CD3 and anti-<br />
CD28 antibodies and stimulated with supernatants of TLR-ligand stimulated<br />
RASF and monocytes or rhIL-23 as a positive control. Subsequently IL-23<br />
dependent IL-17 production was determined by ELISA.<br />
Results: p19 mRNA and protein were abundantly expressed in RA synovial<br />
tissues. Specifically p19 was expressed in the sublining and lining layer as well<br />
as at sites of invasion. Double staining with cell type specific markers revealed<br />
that p19 positive cells expressed the fibroblast marker vimentin or the<br />
macrophage marker CD68. In addition we found that not all p19 positive cells<br />
were double positive for p40. In OA synovial tissues only low levels of p19 were<br />
expressed.<br />
By in vitro stimulation of RASF with the TLR2 ligand bLP, the TLR3 ligand<br />
PIC and the TLR4 ligand LPS we found p19 mRNA to be induced most<br />
markedly by PIC (PIC: 24.4±4; bLP: 9.3±3.5; LPS: 5.8±2.8 fold upregulation relative<br />
to control). However, in RASF the expression of the p40 subunit could<br />
not be induced by any of the TLR ligands. In monocytes both subunits for IL
23 were found to be induced by bLP and LPS (p19 x-fold upregulation: bLP<br />
40±21, LPS: 66±28; p40 x-fold upregulation: bLP: 68±21; LPS: 69±26). The result<br />
that RASF in contrast to monocytes express only p19 but not p40 was further<br />
confirmed with a bioassay. IL-17 production in preactivated T-cell cultures was<br />
induced by rhIL-23 as well as by supernatants of TLR-ligand stimulated monocytes,<br />
but not by supernatants of TLR-ligand stimulated RASF.<br />
Conclusion: The IL-23 subunit p19 is over expressed in RA synovium and<br />
beside macrophages p19 is also expressed by synovial fibroblasts. However, in<br />
contrast to monocytes RASF do not express p40 and therefore RASF are not a<br />
source of functionally active IL-23. The upregulation of p19 by TLR ligands in<br />
RASF suggests, that p19 may either by itself or as a heterodimer with a yet<br />
unknown binding partner have a certain functional role in joint inflammation<br />
and/or destruction.<br />
12<br />
INDUCTION AND ACTIVATION OF THE PATTERN RECOGNITION<br />
RECEPTOR NOD2 IN RHEUMATOID ARTHRITIS<br />
Caroline Ospelt 1 , Fabia Brentano 1 , Beat A. Michel 1 , Beat R. Simmen 2 , Renate E.<br />
Gay 1 , Steffen Gay 1 .<br />
1 Center of Experimental <strong>Rheuma</strong>tology, University Hospital Zurich and Zurich<br />
Center of Integrative Human Physiology (ZIHP), Zurich, Switzerland;<br />
2 Schulthess Clinic, Zurich, Switzerland<br />
Purpose: The pattern recognition receptor Nod2 belongs to the family of Nodlike<br />
receptors, which are critical components of the innate immune response<br />
and are considered to act as cytoplasmic counterparts of Toll-like receptors<br />
(TLR).We analyzed the expression of Nod2 in synovial fibroblasts (SF) and tissues<br />
of rheumatoid arthritis (RA) and osteoarthritis (OA) patients. Furthermore<br />
we studied the influence of Nod2 activation on the expression of cartilage<br />
degrading and pro-inflammatory molecules in RA SF.<br />
Methods: Immunohistochemistry was performed using rabbit anti-human Nod2<br />
antibodies. RA SF (n=4) and OA SF (n=4) were stimulated with TNF (10<br />
ng/ml), IL-1 (1 ng/ml), bacterial lipoprotein (bLP) (300 ng/ml), poly(I-C) (10<br />
µg/ml), LPS (100 ng/ml) and muramyl dipeptide (MDP) (10µg/ml). Expression<br />
of Nod2 mRNA was measured with SYBR green Real-time PCR, levels of IL-<br />
6 and MMP3 protein with ELISA.<br />
Results: Immunohistochemical staining of Nod2 was much more abundant in<br />
the synovium of RA patients compared to OA synovium and was mainly found<br />
at sites of synovial invasion. In unstimulated SF Nod2 mRNA was not<br />
detectable, but it could be strongly induced in RA SF by stimulation with TNF<br />
(571 ±226 fold) and IL-1 (287 ±132 fold), as well as by the TLR2 ligand bLP<br />
(164 ±73 fold), the TLR3 ligand poly(I-C) (6864 ±1871 fold) and the TLR4 ligand<br />
LPS (1069 ±563 fold). Also in OA SF the expression of Nod2 mRNA could<br />
be induced, but to a much lower extend than in RA SF (TNF: 116 ±99 fold; IL-<br />
1: 163 ±66 fold; bLP: 17 ±10 fold; poly(I-C): 981 ±418 fold; LPS: 78 ±19 fold).<br />
Activation of the Nod2 pathway by its ligand MDP only slightly increased the<br />
production of IL-6 by RA SF (control: 3.93 ±0.7 ng/ml; MDP: 4.73 ±1 ng/ml),<br />
but a synergistic effect could be seen, when the cells were pre-stimulated for 5h<br />
with the respective stimulators to induce the expression of Nod2 and then MDP<br />
was added (TNF: 16.9 ±2.6 ng/ml, TNF + MDP: 24.5 ±8 ng/ml; IL-1: 177.5 ±23.3<br />
ng/ml, IL-1 + MDP: 228 ±42.8 ng/ml; bLP: 12.5 ±1.9 ng/ml, bLP + MDP: 25.5<br />
±7.0 ng/ml; poly(I-C): 106 ±33 ng/ml, poly(I-C) + MDP: 247.3 ±50.6 ng/ml; LPS:<br />
41.7 ±3.8 ng/ml, LPS + MDP: 107.1 ±22.7 ng/ml).The same effect was seen when<br />
the expression of MMP-3 was measured (control: 1.5 ±0.6 ng/ml; MDP: 2.2 ±0.8<br />
ng/ml; TNF: 1.9 ±0.6 ng/ml, TNF + MDP: 3.2 ±0.8 ng/ml; IL-1: 41.2 ±24.6 ng/ml,<br />
IL-1 + MDP: 55.5 ±19.3 ng/ml; bLP: 1.9 ±0.7 ng/ml, bLP + MDP: 3.7 ±1.0 ng/ml;<br />
poly(I-C): 6.3 ±1.9 ng/ml, poly(I-C) + MDP: 12.5 ±2.8 ng/ml; LPS: 15.3 ±7.9<br />
ng/ml, LPS + MDP: 32.4 ± 6.0 ng/ml).<br />
Conclusion: Based on the fact that the expression of Nod2 is shown to be<br />
increased in the synovium of RA patients, we suggest that activated TLR pathways<br />
and/or pro-inflammatory cytokines up-regulate the expression of Nod2,<br />
which in turn increases the production of pro-inflammatory cytokines and joint<br />
destructive proteases.<br />
13<br />
AUTO-ANTIBODIES AGAINST SERPIN E2 MIGHT CONTRIBUTE TO<br />
JOINT DESTRUCTION IN RHEUMATOID ARTHRITIS<br />
Hanna Maciejewska, Mariam Al-Shamisi, Renate E. Gay, Beat Michel, Alexander<br />
Knuth, Michel Neidhart, Steffen Gay, Astrid Juengel.<br />
University Hospital, Zurich, Switzerland.<br />
Purpose: Certain auto-antigens in rheumatoid arthritis (RA) have been<br />
defined as disease markers and/or implied to contribute to the induction and<br />
maintenance of inflammatory reactions against the host tissues. In this study we<br />
searched for the presence of novel auto-antibodies in the sera of patients with<br />
RA.<br />
Methods: Novel auto-antigens were identified using a modified serological<br />
analysis of recombinant cDNA expression libraries (SEREX) with synovial<br />
fluid from one RA patient as a source of antibodies. A human cDNA library<br />
from RA synoviocytes (Stratagene) was used for screening. Synovial fluids<br />
were obtained from RA (n=24) and osteoarthritis (OA) (n=16) patients and<br />
pretreated with hyaluronidase for 1h at 37°C. Sera were obtained from patients<br />
with RA (n=7), OA (n=6) and from healthy controls (n=6). The levels of antiserine<br />
protease inhibitor E2 (Serpin E2) auto-antibodies in synovial fluids and<br />
sera were assessed by ELISA. For purification of auto-antibodies from two RA<br />
patients CNBr-activated Sepharose 4 (GE Healthcare) was used. Serpin E2<br />
inhibitory activity was estimated using the urokinase (uPA) activity assay<br />
(Chemicon). In vivo expression of Serpin E2 was determined by immunohistochemistry.<br />
Results: Serpin E2 was prominent among other novel auto-antigenes detected<br />
by the SEREX method. The levels of Serpin E2 reactive antibodies were present<br />
at titers > 20 ng/ml in 50% of RA synovial fluids and differed significantly<br />
from OA synovial fluids of which only 19% had increased levels of anti Serpin<br />
E2 antibodies (p
16<br />
and the endogenous src inhibitor csk in SSc fibroblasts reduced also the synthesis<br />
of ECM proteins. Treatment with SU6656 did not affect the proliferation<br />
capacity of fibroblasts or increase the number of apoptotic or necrotic cells even<br />
after long-term incubation. Consistent with the in vitro data, SU6656 reduced<br />
the accumulation of ECM in vivo. The dermal thickness was reduced dosedependently<br />
by up to 54 ± 16 % with SU6656 compared to bleomycin treated<br />
animals. Furthermore, the number of myofibroblasts decreased by 66 ± 21 % (p<br />
< 0.05 for both). Toxic effects were not observed.<br />
Conclusion: These data indicate that src kinases play important roles for the<br />
activation of fibroblasts by major profibrotic cytokines and for the development<br />
of experimental fibrosis. Thus, src kinases might be interesting targets for novel<br />
antifibrotic therapeutic approaches in SSc.<br />
15<br />
THE ANGIOPOIETIN / TIE2 SYSTEM IN SYSTEMIC SCLEROSIS (SSC)<br />
Falk Moritz 1 , Lars C. Huber 1 , Jörg HW Distler 1 , Astrid Juengel 1 , Beat A. Michel 1 ,<br />
Margerita Pileckyte 2 , Holm Häntzschel 3 , Steffen Gay 1 , Oliver Distler 1 .<br />
1 University Hospital Zurich, Zurich, Switzerland; 2 University Hospital Kaunas,<br />
Kaunas, Lithuania; 3 University Hospital Leipzig, Leipzig, Germany<br />
Purpose: The Angiopoietin (Ang) / Tie2 system represents a receptor ligand<br />
system, which is crucial for the regulation of vessel stability during neoangiogenesis.<br />
Based on recent findings that Ang1 mediates the stabilisation of blood<br />
vessels by binding to its receptor Tie2, whereas Ang2 and soluble Tie2 (sTie2)<br />
modulate the effects of Ang1, we explored the Ang / Tie2 system in SSc.<br />
Methods: 25 SSc patients (17 limited, 7 diffuse SSc) and 20 healthy controls<br />
were included. Serum levels of Ang1, Ang2 and sTie2 were measured by<br />
ELISA. Immunohistochemistry was performed on skin sections obtained from<br />
9 healthy donors and 10 SSc patients. Sections were incubated with antibodies<br />
specific for Tie2, Ang1, Ang2, von Willebrand Factor (vWF) or with the respective<br />
isotypes. In situ hybridization (ISH) for Tie2 specific mRNA was performed<br />
after the generation of riboprobes. Luminal structures were counted in 2-3 arbitrarily<br />
chosen microscopic areas and assessed for the expression of vWF, Tie2<br />
and Ang2. vWF+ structures were defined as microvessels (MV).<br />
Results: The density of MV was lower in biopsies from SSc patients compared<br />
to healthy controls (27.1±7.3 /mm2 vs. 44.3±16.6 /mm2; p=0.053). In addition,<br />
the expression of Tie2 was strongly reduced in SSc skin biopsies: 90% of MV<br />
were positive for Tie2 in healthy skin compared to 5% in SSc (Tie2+/vWF+=0.9<br />
vs. 0.05; p
��� �<br />
�����
18<br />
PERSÖNLICH<br />
Herzliche Gratulation<br />
Dr. med. Giorgio Tamborrini wurde auf den<br />
1. Dezember 2007 zum Oberarzt befördert.<br />
Nach einer Assistententätigkeit in Orthopädie<br />
und Innere Medizin erfolgte die Weiterbildung<br />
in <strong>Rheuma</strong>tologie am Bethesda Spital Basel und in<br />
den letzten zwei Jahren an unserer Klinik. Seine Interessen<br />
Abschied<br />
Erika Omega Huber, Medizinisch-therapeutische Leiterin<br />
Nach über 15-jähriger Tätigkeit an der Spitze der Physio- und<br />
Ergotherapie, an der <strong>Rheuma</strong>klinik und Institut für Physikalische<br />
Medizin des <strong>UniversitätsSpital</strong>s <strong>Zürich</strong>, nimmt Omega<br />
Huber Abschied und stellt sich einer neuen Herausforderung<br />
im Bereich der Klinischen Forschung, im Team von Prof. Dr.<br />
Heike Bischoff-Ferrari.<br />
Die Entwicklung in der Physikalischen Medizin und Rehabilitation<br />
hat sie durch inhaltliche Impulse und organisatorische<br />
Anpassungen wesentlich mitgeprägt. Die Integration<br />
der Ergotherapie und Physiotherapie in interdisziplinäre<br />
Behandlungsteams, die Förderung der funktionellen Diagnostik<br />
und Einführung neuer Therapietechniken sowie die<br />
Unterstützung von Spezialgebieten, welche die vielfältigen<br />
<strong>Das</strong> Kader Physiotherapie 1990<br />
hinten links: Margret Schomburg, Omega Huber, Beatrice<br />
Teuscher, Claudia Frei-Fleischli, Sigrid Kowitz, Karin Staub.<br />
vorne links: Agnès Verbay, Karin Niedermann, Hendrik<br />
Kersch, Barbara Christen<br />
gelten neben der Manuellen Medizin insbesondere der Sonografie<br />
des Bewegungsapparates, wo er seine Erfahrung in der<br />
Ausbildung der Assistenten einbringen wird.<br />
Wir gratulieren herzlich zur Beförderung und wünschen ihm<br />
eine erfolgreiche Oberarzttätigkeit.<br />
Bedürfnisse eines <strong>UniversitätsSpital</strong>s abdecken, waren entscheidend<br />
für den Erfolg unseres Institutes. Selber war sie<br />
mehr als zehn Jahre involviert in die Betreuung von Patienten<br />
mit Hämophilie.<br />
Ein besonderes Anliegen war ihr stets die Zusammenarbeit<br />
aller in den verschiedenen Disziplinen tätigen Medizinalpersonen<br />
als Grundlage einer erfolgreichen Rehabilitation.<br />
Die Wichtigkeit der Qualitätssicherung und Förderung der<br />
Weiter- und Zusatzausbildung wurde von ihr schon früh<br />
erkannt.<br />
Zielgerichtet und nicht immer ohne Widerstand hat Omega<br />
Huber zusammen mit Karin Niedermann die universitäre<br />
Weiterbildung der Physiotherapie in Kooperation mit der<br />
Gesundheitswissenschaftlichen Fakultät der Universität<br />
Maastricht aufgebaut und wird auch weiterhin als Stiftungsratsmitglied<br />
dieses «Kind» aktiv begleiten.<br />
Neben dem grossen beruflichen Engagement hat sie ein<br />
Nachdiplomstudium an der Fachhochschule für Wirtschaft in<br />
St. Gallen mit einem Master of Health Services Administration<br />
abgeschlossen und sich auch standespolitisch stets für<br />
die Anliegen des Berufsverbandes eingesetzt. So ist sie seit<br />
dem Jahr 2005 Präsidentin des <strong>Schweiz</strong>er Physiotherapie Verbandes<br />
und auch Vorstandsmitglied der <strong>Schweiz</strong>erischen<br />
Arbeitsgemeinschaft für Rehabilitation (SAR) sowie Mitglied<br />
der <strong>Schweiz</strong>erischen Gesellschaft für Gesundheitspolitik<br />
(SGGP).<br />
Für den langjährigen, engagierten Einsatz für unsere Klinik<br />
danken wir Omega Huber im Namen aller Mitarbeiterinnen<br />
und Mitarbeitern und wünschen ihr in der neuen Tätigkeit<br />
Genugtuung und insbesondere viel Erfolg. Wir freuen uns<br />
auf die weitere Zusammenarbeit im Rahmen der klinischen<br />
Forschungstätigkeit.<br />
Beat A. Michel, Pius Brühlmann
Omega Huber bei der Hämophiliebehandlung<br />
Am Abschiedssymposium von Esther Meili<br />
(links Omega Huber, rechts Dr. Manuel Rodrigues)<br />
Omega Huber (links) und Karin Niedermann, Co-Programmleiterinnen<br />
Physiotherapie Wissenschaften (PTW)<br />
45–2007<br />
19
20<br />
PUBLIKATIONEN<br />
Original- und Übersichtsartikel<br />
August bis Dezember 2007<br />
Originalartikel<br />
1. Allet L, Cieza A, Bürge E, Finger M, Stucki G, Huber<br />
EO: Intervention categories for physiotherapists treating<br />
patients with musculoskeletal conditions on the basis<br />
of the International Classification of Functioning,<br />
Disability and Health. Int J Rehabil Res 30(4):273-280,<br />
2007.<br />
2. Schenk P, Läubli T, Hodler J, Klipstein A: Symptomatology<br />
of recurrent low back pain in nursing and<br />
administrative professions. Eur Spine 16(11):1789-1798,<br />
2007.<br />
3. Distler JHW, Jüngel A, Pileckyte M, Zwerina J, Michel<br />
BA, Gay RE, Kowal-Bielecka O, Matucci-Cerinic M,<br />
Schett G, Marti HH, Gay S, Distler O: Hypoxia-induced<br />
increase in the production of extracellular matrix proteins<br />
in systemic sclerosis. Arthritis Rheum 56:4203-<br />
4215, 2007.<br />
4. Brentano F, Schorr O, Ospelt C, Stanczyk J, Gay RE Gay<br />
S, Kyburz D: PBEF/Visfatin, a new marker of inflammation<br />
in rheumatoid arthritis with proinflammatory and<br />
matrix degrading activities. Arthritis Rheum 56:2829-<br />
2839, 2007.<br />
5. Jüngel A, Distler O, Schulze-Horsel U, Huber LC, Ha<br />
HR, Simmen B, Kalden JR, Pisetsky DS, Gay S, Distler<br />
JHW: Microparticles stimulate the synthesis of<br />
prostaglandin E(2) via induction of cyclooxygenase 2<br />
and microsomal prostaglandin E synthase 1. Arthritis<br />
Rheum 56: 3564-3574, 2007.<br />
6. Janiak, Thumshirn M, Menne D, Fox M, Halim S, Fried<br />
M, Brühlmann P, Distler O, Schwizer W: The effects of<br />
adding ranitidine at night to twice daily omeprazole<br />
therapy on nocturnal acid breakthrough and acid reflux<br />
in patients with systemic sclerosis: a randomized controlled,<br />
cross over trial. Aliment Pharm Therap 26:1259-<br />
1265, 2007.<br />
7. Walker UA, Tyndall A, Czirják L, Denton C, Farge-<br />
Bancel D, Kowal-Bielecka O, Distler O, Müller-Ladner<br />
U, Bocelli-Tyndall C, Matucci-Cerinic M: Clinical risk<br />
assessment of organ manifestations in systemic sclerosis:<br />
a report from the EULAR Scleroderma Trials And<br />
Research group database. Ann Rheum Dis 66:754-763,<br />
2007.<br />
8. Broe KE, Chen TC, Weinberg J, Bischoff-Ferrari HA,<br />
Holick MF, Kiel DP: A higher dose of vitamin d reduces<br />
the risk of falls in nursing home residents: a randomized,<br />
multiple-dose study. J Am Geriatr Soc 55(2):234-239,<br />
2007.<br />
9. Bischoff-Ferrari HA, Orav JE, Barrett JA, Baron JA:<br />
Effect of seasonality and weather on fracture risk in<br />
individuals 65 years and older. Osteoporos Int<br />
8(9):1225-1233, 2007.<br />
10. Forman JP, Giovannucci E, Holmes MD, Bischoff-<br />
Ferrari HA, Tworoger SS, Willett WC, Curhan GC:<br />
Plasma 25-hydroxyvitamin D levels and risk of incident<br />
hypertension. Hypertension 49(5):1063-1069, 2007.<br />
11. Bischoff-Ferrari HA, Dawson-Hughes B, Baron JA,<br />
Burckhardt P, Li R, Spiegelman D, Specker B, Orav JE,<br />
Wong JB, Staehelin HB, O'Reilly E, Kiel DP, Willett<br />
WC: Calcium intake and hip fracture risk in men and<br />
women: a meta-analysis of prospective cohort studies<br />
and randomized controlled trials. Am J Clin Nutr<br />
86(6):1780-1790, 2007.<br />
12. Aviña-Zubieta JA, Alarcón GS, Bischoff-Ferrari HA,<br />
Fischer-Betz R, Schneider M: Measurement of fatigue in<br />
systemic lupus erythematosus: A systematic review.<br />
Arthritis Rheum 57(8):1348-1357, 2007.
Reviews<br />
13. Hilfiker R, Bachmann LM, Heitz C, Lorenz T, Joronen<br />
H, Klipstein A: Value of predictive in 06. struments to<br />
determine return to work in patients with subacute nonspecific<br />
low back pain. Systematic review. Eur Spine J<br />
16(11):1755-1775, 2007.<br />
14. Goldhahn J, Kolling C, Gay S, Simmen BR: Functional<br />
staging and surgical intervention of the elbow and shoulder<br />
joints in a patient with rheumatoid arthritis. Nat Clin<br />
Pract <strong>Rheuma</strong>tol 3:112-117, 2007.<br />
15. Huber LC, Stanczyk J, Jungel A, Gay S: Epigenetics in<br />
inflammatory rheumatic diseases. Arthritis Rheum<br />
56:3523-3531, 2007.<br />
16. Abraham D, Distler O: How does endothelial cell injury<br />
start? The role of endothelin in systemic sclerosis.<br />
Arthritis Res Ther 9:S2, 2007.<br />
17. Koch AE, Distler O: Vasculopathy and disordered<br />
angiogenesis in connective tissue disease. Arthritis Res<br />
Ther 9: S3, 2007.<br />
18. Vieth R, Bischoff-Ferrari H, Boucher BJ, Dawson-<br />
Hughes B, Garland CF, Heaney RP, Holick MF, Hollis<br />
BW, Lamberg-Allardt C, McGrath JJ, Norman AW,<br />
Scragg R, Whiting SJ, Willett WC, Zittermann A: The<br />
urgent need to recommend an intake of vitamin D that<br />
is effective. Am J Clin Nutr 85(3):649-650, 2007.<br />
19. Bischoff-Ferrari HA, Dawson-Hughes B: Where do we<br />
stand on vitamin D? Bone 41(1 Suppl 1):S13-19, 2007.<br />
20. Bischoff-Ferrari HA: The 25-hydroxyvitamin D threshold<br />
for better health. J Steroid Biochem Mol Biol 103(3-<br />
5):614-619, 2007.<br />
21. Bischoff-Ferrari HA: How to select the doses of vitamin<br />
D in the management of osteoporosis. Osteoporos Int<br />
18(4):401-407, 2007.<br />
Editorial<br />
22. Muller-Ladner U, Gay S: Molecular mechanisms. Z<br />
<strong>Rheuma</strong>tol 66:285, 2007.<br />
Buchkapitel<br />
23. Meinecke I, Rutkauskaite E, Cinski A, Muller-Ladner U,<br />
Gay S, Pap T: Gene transfer to synovial fibroblast:<br />
methods and evaluation in the SCID mouse model.<br />
Methods Mol Med 135:393-412, 2007.<br />
24. Neumann E, Judex M, Gay S, Muller-Ladner U:<br />
Genotyping of synovial fibroblasts: cDNA array in combination<br />
with RAP-PCR in arthritis. Methods Mol Med<br />
135:377-391, 2007.<br />
25. Muller-Ladner U, Judex M, Neumann E, Gay S: Laser<br />
capture as a tool for analysis of gene expression in<br />
inflamed synovium. Methods Mol Med 135:91-104, 2007.<br />
26. Distler JH, Distler O, Neidhart M, Gay S: Subtractive<br />
hybridization of the inflamed synovium. Methods Mol<br />
Med 135:77-90, 2007.<br />
27. Kuchen S, Seemayer CA, Neidhart M, Gay RE, Gay S:<br />
In situ hybridization of synovial tissue. Methods Mol<br />
Med 135:65-75, 2007.<br />
28. Pap T, Gay S, Schett G: Matrix metalloproteinases, in<br />
Contemporary Targeted Therapies in <strong>Rheuma</strong>tology,<br />
Ed. by JS Smolen and PE Lipsky, informa Healthcare<br />
UK Ltd 353-366, 2007.<br />
45–2007<br />
21
22<br />
FORT- UND<br />
WEITERBILDUNG<br />
Fort- und Weiterbildung in<br />
<strong>Rheuma</strong>tologie und Physikalischer Medizin (USZ)<br />
31. Januar bis 10. April 2008<br />
Datum Thema Zeit Ort<br />
Donnerstag Weiterbildung 16.00 bis Kursraum U Ost 157<br />
31. Januar 2008 Grenzgebiete 17.00 Uhr (gross)<br />
– Dr. Mark Fox, Klinik für Gastroenterologie, USZ<br />
Dyspepsie<br />
Apéro<br />
Donnerstag Weiterbildung 15.00 bis Kursraum U Ost 157<br />
7. Februar 2008 Grenzgebiete 16.00 Uhr (gross)<br />
– Prof. Dr. Eli Alon, PD Dr. Peter Sandor, PD Dr. Haiko Sprott, USZ<br />
– Dr. Kyrill Schwegler, Praxis: Vogelsangstrasse 52, 8006 <strong>Zürich</strong><br />
Schmerzmedizinische Schlüsselbotschaften<br />
Donnerstag Weiterbildung 15.00 bis Kursraum U Ost 157<br />
28. Februar 2008 <strong>Rheuma</strong>tologie 16.00 Uhr (gross)<br />
– PD Dr. Robert Theiler, Stadtspital Triemli <strong>Zürich</strong><br />
Qualitätssicherung bei der Therapie von Schmerz-Patient/innen<br />
mit Hüft- und/oder Knie-Arthrose – das Qualitouch-Projekt<br />
Donnerstag Weiterbildung 15.00 bis Kursraum U Ost 157<br />
6. März 2008 Klinische Immunologie 16.00 Uhr (gross)<br />
– Prof. Adriano Fontana, Klinik für Immunologie, Departement Innere Med, USZ<br />
Weshalb sind wir bei der rheumatoiden Arthritis, dem systemischen<br />
Lupus erythematodes wie auch bei akuten Infektionserkrankungen<br />
müde?<br />
Donnerstag 175-Jahr-Feier der Universität <strong>Zürich</strong> Lichthof Universität<br />
13. März 2008 Unitage der Medizinischen Fakultät<br />
Donnerstag Jahresversammlung der Zürcher Fachärztegesellschaft 15.30 bis Kursraum U Ost 157<br />
27. März 2008 für <strong>Rheuma</strong>tologie 18.00 Uhr (gross)<br />
– Generalversammlung 13.30 bis 15.00 Uhr<br />
– Dr. med. Hans-Kaspar Schwyzer, Schulthess Klinik <strong>Zürich</strong> 15.30 Uhr<br />
Wann soll was an der Schulter operiert werden?<br />
– Dr. med. Jörg Jeger, MEDAS, Luzern 16.15 Uhr<br />
Beurteilung der Arbeitsfähigkeit – eine ärztliche Aufgabe?<br />
– PD Dr. med. Diego Kyburz, <strong>Rheuma</strong>klinik und<br />
Institut für Physikalische Medizin, <strong>UniversitätsSpital</strong> <strong>Zürich</strong> 17.00 Uhr<br />
BIOLOGIKA: Was ist wann indiziert und was ist bei ungenügender<br />
Wirkung zu tun?<br />
Stehbuffet
Datum Thema Zeit Ort<br />
Donnerstag Weiterbildung 15.00 bis Kursraum U Ost 157<br />
10. April 2008 Grenzgebiete 16.00 Uhr (gross)<br />
Thema: Sprtmedizin<br />
– Dr. Walter O. Frey «Iatrogenes Doping»<br />
move>med, Swiss Olympic Medical Center, Forchstrasse 317, 8008 <strong>Zürich</strong><br />
Schmerz-Kolloquium 16.05 bis Kleiner Hörsaal B Ost<br />
Schmerztherapeutische Schlüsselbotschaften aus der Interdisziplinären 18.00 Uhr Gloriastrasse 29<br />
Schmerzsprechstunde (ISSS)<br />
Moderation: PD Dr. M. Felder<br />
Prof. Eli Alon, Institut für Anästhesiologie, USZ<br />
PD Dr. Peter Sandor, Neurologische Klinik, USZ<br />
Dr. Kyrill Schwegler, Praxis: Vogelsangstrasse 52, 8006 <strong>Zürich</strong><br />
PD Dr. Haiko Sprott, <strong>Rheuma</strong>klinik und Institut für Physikalische Medizin, USZ<br />
Aktualisierte Informationen finden Sie auf der Website http://www.rheuma-schweiz.ch/go2/de/1030<br />
Sponsoren «Fort- und Weiterbildung»<br />
Folgende Firmen haben unsere Weiterbildungsveranstaltungen unterstützt, wofür wir uns herzlich bedanken!<br />
Essex Chemie AG<br />
45–2007<br />
23
Condrosulf ® hält das Fortschreiten der Arthrose auf. 1,2<br />
1. Kahan A, Vignon E et al. STOPP (STudy on Osteoarthritis Progression Prevention): A new two-year trial with chondroitin 4&6<br />
sulfate. Presented in a Satellite Symposium held at the Annual European Congress of <strong>Rheuma</strong>tology (EULAR), Amsterdam,<br />
21–24 June 2006. 2. Michel BA, Stucki G, Frey D, De Vathaire F, Vignon E, Bruehlmann P, Uebelhart D. Chondroitin 4 and 6<br />
Sulfate in Osteoarthritis of the Knee: A Randomized, Controlled Trial. Arthritis Rheum 2005; 52(3): 779–786.<br />
Z: chondroitini sulfas natricus. I: Degenerative Gelenkerkrankungen. D: 800 mg täglich während einer 3-monatigen Kur. Kl: Überempfindlichkeit<br />
gegen den Wirkstoff. UW: Leichte gastrointestinale Beschwerden, sporadisch allergische Reaktionen. IA: Keine<br />
bekannt. P: Tabletten zu 800 mg: 30*/90*; Granulat in Beuteln zu 800 mg: 30*/90*. Liste B. *Kassenzulässig. Ausführliche<br />
Angaben siehe Arzneimittel-Kompendium der <strong>Schweiz</strong>.<br />
IBSA Institut Biochimique SA, Headquarters and Marketing Operations, Via del Piano, CH-6915 Pambio-Noranco, www.ibsa.ch<br />
Bewegt Menschen.