

Difficult airway management in the emergency department.
Difficult airway management in the emergency department.
Difficult airway management in the emergency department.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Cl<strong>in</strong>ical<br />
Communications<br />
PII S0736-4679(01)00435-8<br />
DIFFICULT AIRWAY MANAGEMENT IN THE EMERGENCY DEPARTMENT<br />
Steven L. Orebaugh, MD<br />
Department of Anes<strong>the</strong>siology, University of Pittsburgh Medical Center, Southside, Pittsburgh, Pennsylvania<br />
Repr<strong>in</strong>t Address: Steven L. Orebaugh, MD, Department of Anes<strong>the</strong>siology, UPMC-Southside, 2000 Mary St., Pittsburgh, PA 15228<br />
e Abstract—Most <strong>airway</strong> <strong>management</strong> <strong>in</strong> <strong>the</strong> <strong>emergency</strong><br />
<strong>department</strong> is straightforward and readily accomplished by<br />
<strong>the</strong> <strong>emergency</strong> physician. The exact <strong>in</strong>cidence of difficult<br />
<strong>in</strong>tubations is difficult to discern from available evidence,<br />
but <strong>the</strong>se are probably more frequent <strong>in</strong> <strong>the</strong> Emergency<br />
Department than <strong>in</strong> <strong>the</strong> operat<strong>in</strong>g room, given <strong>the</strong> urgent<br />
nature of <strong>the</strong> procedure and <strong>the</strong> lack of preparation of <strong>the</strong><br />
patient population. A variety of adjuncts for <strong>airway</strong> <strong>management</strong><br />
are available to assist <strong>in</strong> both <strong>in</strong>tubation and ventilation.<br />
The utility of <strong>the</strong>se adjuncts is detailed <strong>in</strong> this<br />
review, with emphasis on techniques most useful to <strong>the</strong><br />
<strong>emergency</strong> physician. © 2002 Elsevier Science Inc.<br />
e Keywords—<strong>airway</strong> <strong>management</strong>; <strong>in</strong>tubation; ventilation<br />
laryngoscopy; <strong>airway</strong> adjuncts; difficult <strong>in</strong>tubation and<br />
ventilation<br />
INTRODUCTION<br />
Emergency physicians are frequently required to provide<br />
timely, def<strong>in</strong>itive <strong>airway</strong> <strong>management</strong> <strong>in</strong> acutely ill patients.<br />
As <strong>the</strong> specialty has emerged and <strong>the</strong>n matured<br />
over <strong>the</strong> last two and a half decades, practitioners of<br />
Emergency Medic<strong>in</strong>e have become <strong>in</strong>creas<strong>in</strong>gly proficient<br />
<strong>in</strong> this skill, and have modified <strong>the</strong>ir approaches to<br />
<strong>airway</strong> <strong>management</strong> significantly, rely<strong>in</strong>g less and less<br />
on assistance from o<strong>the</strong>r medical specialists (1). Residency<br />
tra<strong>in</strong><strong>in</strong>g <strong>in</strong> Emergency Medic<strong>in</strong>e, however, provides<br />
little tra<strong>in</strong><strong>in</strong>g <strong>in</strong> <strong>the</strong> nonsurgical approach to <strong>the</strong><br />
difficult <strong>airway</strong> (2). Emergency physicians are expected<br />
to emerge from residency with competence <strong>in</strong> <strong>the</strong> surgical<br />
<strong>management</strong> of <strong>the</strong> <strong>airway</strong>, but with improved <strong>in</strong>tubation<br />
rates have come reduced opportunity for cricothyrotomy<br />
(3). Because patients present<strong>in</strong>g with difficult<br />
<strong>airway</strong>s are uncommon but not rare, and because <strong>the</strong> very<br />
nature of <strong>emergency</strong> practice may predispose to difficulties<br />
with <strong>airway</strong> <strong>management</strong>, it behooves <strong>the</strong> <strong>emergency</strong><br />
physician to become familiar with a range of <strong>airway</strong><strong>management</strong><br />
techniques, <strong>in</strong>clud<strong>in</strong>g direct laryngoscopy<br />
with rapid sequence <strong>in</strong>tubation (RSI), alternatives to<br />
laryngoscopy for <strong>in</strong>tubation, rescue ventilation techniques,<br />
and surgical approaches to <strong>the</strong> <strong>airway</strong>. This review<br />
will concentrate upon recognition of <strong>the</strong> difficult<br />
<strong>airway</strong>, preparation for manag<strong>in</strong>g <strong>the</strong> difficult <strong>airway</strong>,<br />
and <strong>the</strong> various adjuncts available to facilitate <strong>in</strong>tubation<br />
and ventilation <strong>in</strong> this sett<strong>in</strong>g.<br />
Def<strong>in</strong>itions<br />
RECEIVED: 29 December 2000; FINAL SUBMISSION RECEIVED: 2 July 2000;<br />
ACCEPTED: 17 July 2000.<br />
31<br />
The Journal of Emergency Medic<strong>in</strong>e, Vol. 22, No. 1, pp. 31–48, 2002<br />
Copyright © 2002 Elsevier Science Inc.<br />
Pr<strong>in</strong>ted <strong>in</strong> <strong>the</strong> USA. All rights reserved<br />
0736-4679/02 $–see front matter<br />
The term “difficult <strong>airway</strong>” defies simple def<strong>in</strong>ition. It<br />
may be construed to mean difficult laryngoscopy, difficult<br />
mask ventilation, difficult endotracheal tube placement,<br />
or <strong>the</strong> failure to <strong>in</strong>tubate or ventilate. Some of<br />
<strong>the</strong>se ideas have been expressed quantitatively: difficult<br />
mask ventilation is def<strong>in</strong>ed by <strong>the</strong> American Society of<br />
Anes<strong>the</strong>siology as <strong>the</strong> <strong>in</strong>ability of a tra<strong>in</strong>ed anes<strong>the</strong>tist to<br />
ma<strong>in</strong>ta<strong>in</strong> <strong>the</strong> oxygen saturation above 90% by us<strong>in</strong>g<br />
face-mask ventilation (when <strong>the</strong> <strong>in</strong>itial saturation was <strong>in</strong><br />
<strong>the</strong> normal range) whereas difficult <strong>in</strong>tubation is def<strong>in</strong>ed
32 S. L. Orebaugh<br />
Figure 1. Grades of laryngeal exposure (repr<strong>in</strong>ted with permission by Blackwell Science, Ltd. (9)).<br />
as an <strong>in</strong>ability to place an endotracheal tube with<strong>in</strong> 10<br />
m<strong>in</strong> or three attempts (4).<br />
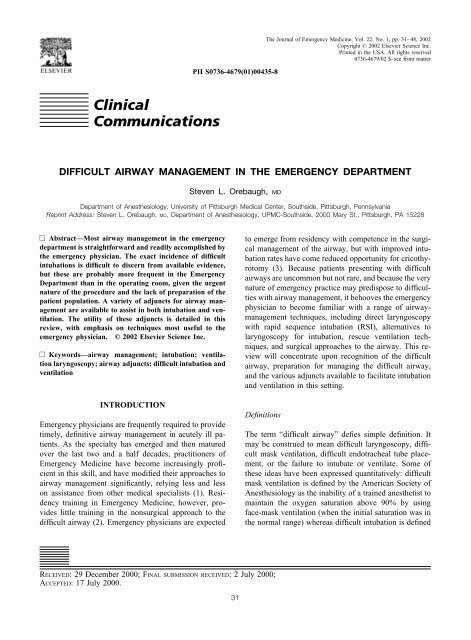
<strong>Difficult</strong> <strong>in</strong>tubation usually corresponds to poor glottic<br />
visualization dur<strong>in</strong>g direct laryngoscopy, or a highgrade<br />
laryngeal view with no ability to see <strong>the</strong> vocal<br />
cords or <strong>the</strong> glottic aperture (Figure 1) (5). Cormack and<br />
Lehane, <strong>in</strong> a paper that described <strong>the</strong> likelihood of difficult<br />
<strong>in</strong>tubation <strong>in</strong> obstetrics, proposed a classification<br />
scheme for views of <strong>the</strong> laryngeal <strong>in</strong>let obta<strong>in</strong>ed at laryngoscopy<br />
(5). This four-grade scheme has become <strong>the</strong><br />
standard measurement of glottic views, and facilitates<br />
communication between researcher and practitioners as<br />
to <strong>the</strong> impact of <strong>the</strong> view obta<strong>in</strong>ed on <strong>the</strong> success of<br />
tracheal tube placement. Grade 1 corresponds to a view<br />
of all or most of <strong>the</strong> glottis; Grade 2 to a view <strong>in</strong> which<br />
only <strong>the</strong> posterior portion of <strong>the</strong> glottis is visible; Grade<br />
3 to visualization of only <strong>the</strong> epiglottis; and grade 4 to<br />
<strong>in</strong>ability to see <strong>the</strong> glottis or epiglottis at all (5). The<br />
authors ma<strong>in</strong>ta<strong>in</strong> that Grade 3 and 4 views are rare and<br />
likely to be difficult to manage, whereas grades 1 and 2<br />
are quite common and easily managed by <strong>the</strong> practic<strong>in</strong>g<br />
anes<strong>the</strong>siologist.<br />
<strong>Difficult</strong>y with glottic exposure at direct laryngoscopy<br />
also can be quantitated by <strong>the</strong> “Percent of Glottic Open<strong>in</strong>g<br />
(POGO)” score, which corresponds to <strong>the</strong> proportion<br />
of <strong>the</strong> open<strong>in</strong>g that can be visualized (6). In addition,<br />
Adnet et al. have more recently proposed an <strong>in</strong>tubation<br />
difficulty scale, which <strong>the</strong>y <strong>the</strong>n validated prospectively<br />
<strong>in</strong> 626 patients, and which corresponds well to <strong>the</strong> time<br />
required for <strong>in</strong>tubation and a visual analog scale assessment<br />
of procedural difficulty by <strong>in</strong>tubators (7).<br />
Prediction<br />
Predict<strong>in</strong>g which patients will present challeng<strong>in</strong>g or<br />
impossible ventilation, laryngoscopy, or <strong>in</strong>tubation is<br />
troublesome and most assessments lack accuracy. Falsepositive<br />
and false-negative predictions are <strong>in</strong>evitable.<br />
However, some predictors have proven consistently useful,<br />
and comb<strong>in</strong>ations of predictors even more so. Perhaps<br />
<strong>the</strong> most utilized predictive scheme for <strong>airway</strong><br />
assessment <strong>in</strong> anes<strong>the</strong>siology is <strong>the</strong> Mallampati classification,<br />
which assigns three gradations of <strong>in</strong>creas<strong>in</strong>g difficulty<br />
<strong>in</strong> visualiz<strong>in</strong>g <strong>the</strong> posterior pharyngeal structures<br />
<strong>in</strong> order to predict difficult laryngeal exposure (8). The<br />
Samsoon and Young modification breaks this assessment<br />
<strong>in</strong>to four classes, <strong>the</strong> highest grade divided <strong>in</strong>to those<br />
whose soft palate can be seen and those whose cannot<br />
(Figure 2) (9). These predictive tools evaluate <strong>the</strong> size of<br />
<strong>the</strong> tongue, which must be displaced <strong>in</strong> order to view <strong>the</strong><br />
glottis, relative to <strong>the</strong> oropharynx. In one study, 14 of 15<br />
Figure 2. Samsoon and Young modification of Mallampati classification, evaluat<strong>in</strong>g relative size of oropharyngeal structures <strong>in</strong><br />
order to predict difficulty <strong>in</strong> laryngeal exposure dur<strong>in</strong>g direct laryngoscopy. Higher class number suggests greater difficulty <strong>in</strong><br />
glottic exposure (repr<strong>in</strong>ted with permission by Blackwell Science, Ltd. (9)).
<strong>Difficult</strong> Airway Management 33<br />
patients whose <strong>airway</strong> assessment fell <strong>in</strong>to <strong>the</strong> Mallampati<br />
Class 3 were determ<strong>in</strong>ed to have a poor laryngoscopic<br />
grade at direct laryngoscopy (10).<br />
Many o<strong>the</strong>r <strong>airway</strong> assessment schemes have been<br />
proposed and evaluated, <strong>in</strong>clud<strong>in</strong>g evaluation of <strong>the</strong> jaw<br />
size, thyromental distance, and cervical range of motion<br />
(11–14). Each of <strong>the</strong>se has limited sensitivity and specificity,<br />
and most anes<strong>the</strong>siologists comb<strong>in</strong>e an assessment<br />
of <strong>the</strong> Mallampati class, mouth open<strong>in</strong>g, cervical<br />
range of motion, and thyromental distance to comprise a<br />
multifactorial approach to predict<strong>in</strong>g difficulty <strong>in</strong> direct<br />
laryngoscopy. This approach successfully predicts difficulty<br />
<strong>in</strong> nearly all <strong>in</strong>stances (15,16). A simple “Rule of<br />
Three’s” also can be applied: If one can place three<br />
f<strong>in</strong>gerbreadths between <strong>the</strong> teeth, between <strong>the</strong> mandibular<br />
genu and <strong>the</strong> hyoid bone, and between <strong>the</strong> thyroid<br />
cartilage and <strong>the</strong> sternal notch <strong>in</strong> neutral position, direct<br />
laryngoscopy probably will be successful (15). Recent<br />
evidence suggests that difficult bag-valve-mask (BVM)<br />
ventilation may be more frequent than previously<br />
thought (17). Langeron found that 5% of 1502 patients<br />
were difficult to ventilate by BVM under general anes<strong>the</strong>sia<br />
(SaO 2 fell below 92% or unable to obta<strong>in</strong> evidence<br />
of effective ventilation) but this situation was anticipated<br />
<strong>in</strong> less than one fifth of <strong>the</strong>se cases. Body mass <strong>in</strong>dex,<br />
advanc<strong>in</strong>g age, presence of a beard, lack of teeth, and a<br />
history of snor<strong>in</strong>g all predicted difficult ventilation by<br />
BVM.<br />
Unfortunately, <strong>the</strong>se assessment tools have been derived<br />
from studies <strong>in</strong> which cooperative, composed patients<br />
are exam<strong>in</strong>ed by anes<strong>the</strong>siologists on preoperative<br />
rounds ra<strong>the</strong>r than by <strong>emergency</strong> physicians evaluat<strong>in</strong>g<br />
patients <strong>in</strong> extremis. The utility of <strong>the</strong>se tools <strong>in</strong> <strong>the</strong><br />
Emergency Department (ED) sett<strong>in</strong>g has not been demonstrated.<br />
Never<strong>the</strong>less, an appreciation of mouth open<strong>in</strong>g,<br />
cervical mobility, thyromental distance, and tongue<br />
size can be rapidly ga<strong>in</strong>ed and may help <strong>the</strong> <strong>emergency</strong><br />
physician avoid a disastrous sequence of events when<br />
difficulty is likely.<br />
Incidence<br />
Much had been done to document <strong>the</strong> occurrence of<br />
difficult <strong>airway</strong>s <strong>in</strong> <strong>the</strong> perioperative sett<strong>in</strong>g. Grade 3<br />
laryngoscopy, requir<strong>in</strong>g multiple attempts at <strong>in</strong>tubation,<br />
occurs <strong>in</strong> 1–4% among all types of patients, but was<br />
estimated to occur <strong>in</strong> only 1 of 2000 obstetric patients,<br />
who have relatively normal necks and cervical mobility<br />
(5,11,18,19). Inability to <strong>in</strong>tubate due to severe Grade 3<br />
or Grade 4 laryngoscopic views is present <strong>in</strong> only 0.05–<br />
0.35% of operat<strong>in</strong>g room (OR) cases, but aga<strong>in</strong> appears<br />
to be more rare among those with normal cervical mobility<br />
(5,9,18,20). <strong>Difficult</strong> mask ventilation occurs 5%<br />
of <strong>the</strong> time, as outl<strong>in</strong>ed above (17). Fortunately, <strong>in</strong>ability<br />
to ventilate comb<strong>in</strong>ed with <strong>in</strong>ability to <strong>in</strong>tubate is very rare<br />
<strong>in</strong> <strong>the</strong> OR, compris<strong>in</strong>g less than 2 <strong>in</strong> 10,000 cases (13,21).<br />
Mild difficulty with <strong>in</strong>tubation requir<strong>in</strong>g a change of blades<br />
or operators is fairly common, reportedly occurr<strong>in</strong>g <strong>in</strong><br />
1–18% of <strong>in</strong>tubations <strong>in</strong> <strong>the</strong> OR (21–23).<br />
Management of <strong>the</strong> difficult <strong>airway</strong> <strong>in</strong> <strong>the</strong> ED has not<br />
been as well studied as that <strong>in</strong> <strong>the</strong> OR. Indeed, it is<br />
necessary to extrapolate from descriptive studies of <strong>airway</strong><br />
<strong>management</strong> <strong>in</strong> <strong>the</strong> ED, <strong>in</strong> which significant portions<br />
of <strong>the</strong> population under study are excluded from <strong>the</strong><br />
<strong>in</strong>vestigation for various reasons. Sakles et al., describe<br />
610 patients undergo<strong>in</strong>g <strong>in</strong>tubation <strong>in</strong> an urban ED over<br />
1 year, 84% of <strong>the</strong>se were rapid sequence <strong>in</strong>tubations<br />
(RSI) with a 99% success rate, and 1% required cricothyrotomy<br />
(25). Five percent of patients <strong>in</strong>itially received<br />
an esophageal <strong>in</strong>tubation; we can surmise, <strong>the</strong>n, that<br />
6% of <strong>the</strong>se patients had a difficult <strong>airway</strong>. Overall, 5%<br />
required three or more attempts at direct laryngoscopy,<br />
and <strong>the</strong>se could perhaps be added to <strong>the</strong> o<strong>the</strong>r 6% (if we<br />
presume no overlap between <strong>the</strong>se and <strong>the</strong> patients hav<strong>in</strong>g<br />
an esophageal tube), and thus some difficulty <strong>in</strong><br />
<strong>in</strong>tubation would range between 6% and 11%. However,<br />
some 16% of patients were deemed unfit for RSI, and <strong>the</strong><br />
reasons for this are not apparent <strong>in</strong> all cases.<br />
In <strong>the</strong> study of Tayal et al., <strong>the</strong> proportion of difficult<br />
<strong>airway</strong>s among patients <strong>in</strong>tubated is also somewhat obscure<br />
(26). Thirty percent of patients who were <strong>in</strong>tubated<br />
were not <strong>in</strong>cluded <strong>in</strong> <strong>the</strong> analysis because <strong>the</strong>y did not<br />
meet <strong>the</strong> <strong>in</strong>vestigators’ requirement for eligibility for<br />
RSI. Aga<strong>in</strong>, 1% required cricothyrotomy. Thus, <strong>the</strong> actual<br />
<strong>in</strong>cidence of difficult <strong>airway</strong>s lies somewhere between<br />
<strong>the</strong> extremes of 1% and 30%. Even if we choose <strong>the</strong><br />
lower figure, difficult <strong>airway</strong>s <strong>in</strong> <strong>the</strong> ED population will not<br />
be considered rare, and <strong>the</strong>y are probably much more<br />
commonly encountered <strong>in</strong> this sett<strong>in</strong>g than <strong>in</strong> <strong>the</strong> OR.<br />
More recently, a multicenter study of ED <strong>airway</strong><br />
<strong>management</strong> has been conducted (27). This <strong>in</strong>vestigation,<br />
a prospective, observational study of almost 6300<br />
cases, comprises <strong>the</strong> most comprehensive data regard<strong>in</strong>g<br />
<strong>emergency</strong> physician practices <strong>in</strong> <strong>management</strong> of <strong>the</strong><br />
<strong>airway</strong>. In a query of <strong>the</strong> National Emergency Airway<br />
Registry data, Li reported esophageal <strong>in</strong>tubation <strong>in</strong> 4%<br />
of cases, though only a small fraction of <strong>the</strong>se were not<br />
immediately recognized (28). Rapid sequence <strong>in</strong>tubation<br />
was <strong>the</strong> predom<strong>in</strong>ant method used to provide <strong>airway</strong>s <strong>in</strong><br />
this population, with over 98% success <strong>in</strong> over 4400<br />
patients. O<strong>the</strong>r methods <strong>in</strong>cluded oral <strong>in</strong>tubation with<br />
sedation only, oral <strong>in</strong>tubation with no medications, and<br />
bl<strong>in</strong>d nasal <strong>in</strong>tubation, all of which were significantly<br />
less successful techniques than RSI <strong>in</strong> secur<strong>in</strong>g <strong>the</strong> <strong>airway</strong>.<br />
Thus, RSI appears to be <strong>the</strong> most frequently used<br />
and most successful means of <strong>in</strong>tubat<strong>in</strong>g <strong>the</strong> trachea <strong>in</strong><br />
Emergency Medic<strong>in</strong>e.
34 S. L. Orebaugh<br />
As noted above, <strong>the</strong> very nature of <strong>emergency</strong> practice<br />
may contribute to difficulties <strong>in</strong> <strong>airway</strong> <strong>management</strong><br />
not encountered <strong>in</strong> more elective sett<strong>in</strong>gs. The <strong>in</strong>ability<br />
to ask <strong>the</strong> patient if he or she has encountered prior<br />
<strong>airway</strong> problems (<strong>in</strong>clud<strong>in</strong>g surgery or adverse anes<strong>the</strong>sia<br />
occurrences) due to confusion, extremis, or obtundation<br />
is common. Fur<strong>the</strong>r, hav<strong>in</strong>g <strong>the</strong> patient adopt a<br />
sitt<strong>in</strong>g position while exam<strong>in</strong><strong>in</strong>g <strong>the</strong> pharynx, thyromental<br />
distance, and cervical range of motion is frequently<br />
impossible due to <strong>the</strong> acute nature of <strong>the</strong> patient’s illness<br />
or <strong>the</strong> impracticality of adopt<strong>in</strong>g such positions. The<br />
presumption of a “full stomach” <strong>in</strong> all patients <strong>in</strong>tubated<br />
emergently dictates <strong>the</strong> use of <strong>the</strong> RSI technique. The<br />
imposition of cricoid pressure and laryngoscopy at <strong>the</strong><br />
earliest possible moment place <strong>in</strong>creased demands upon<br />
<strong>the</strong> physician prepar<strong>in</strong>g to <strong>in</strong>tubate <strong>the</strong> patient (29). The<br />
trauma patient places even more obstacles to <strong>in</strong>tubation<br />
<strong>in</strong> <strong>the</strong> path of <strong>the</strong> <strong>emergency</strong> physician. Facial distortion,<br />
secretions, swell<strong>in</strong>g, mandibular <strong>in</strong>jury, and potential<br />
cervical sp<strong>in</strong>e <strong>in</strong>jury all comb<strong>in</strong>e to make <strong>the</strong>se patients<br />
among <strong>the</strong> most challeng<strong>in</strong>g <strong>airway</strong>-<strong>management</strong> problems<br />
(30). Cervical collars and <strong>in</strong>-l<strong>in</strong>e immobilization<br />
impact glottic exposure adversely, and up to 20% of<br />
<strong>the</strong>se patients may have a Grade 3 or Grade 4 laryngoscopic<br />
view (31).<br />
In summary, <strong>the</strong> difficult <strong>airway</strong> can be def<strong>in</strong>ed <strong>in</strong><br />
different ways, and its exact <strong>in</strong>cidence <strong>in</strong> <strong>the</strong> ED is not<br />
clearly del<strong>in</strong>eated. Poor laryngoscopic grade is apparently<br />
more common <strong>in</strong> <strong>the</strong> ED population than <strong>in</strong> patients<br />
present<strong>in</strong>g for elective surgery, given <strong>the</strong> frequency of<br />
multiple attempts at <strong>in</strong>tubation and esophageal <strong>in</strong>tubation<br />
cited <strong>in</strong> <strong>the</strong> studies above. Never<strong>the</strong>less, failure to secure<br />
<strong>the</strong> <strong>airway</strong> by nonsurgical means is quite <strong>in</strong>frequent <strong>in</strong><br />
<strong>the</strong> ED, on <strong>the</strong> order of 1% of cases.<br />
Approach to <strong>the</strong> Recognized <strong>Difficult</strong> Airway<br />
In many cases, difficulty with glottic exposure may be<br />
predicted from even a cursory exam<strong>in</strong>ation of <strong>the</strong> patient.<br />
In o<strong>the</strong>rs, it is only apparent after a hypnotic and relaxant<br />
have been adm<strong>in</strong>istered, dur<strong>in</strong>g attempted direct laryngoscopy.<br />
This situation may quickly lead to multiple<br />
attempts to secure <strong>the</strong> <strong>airway</strong>, supraglottic swell<strong>in</strong>g and<br />
bleed<strong>in</strong>g, deterioration of ventilation, and hypoxemia<br />
with potential morbidity (32–34). Because of <strong>the</strong> potential<br />
for <strong>in</strong>jury and mortality when <strong>airway</strong> disasters occur,<br />
<strong>the</strong> American Society of Anes<strong>the</strong>siology (ASA) developed<br />
<strong>the</strong> ASA <strong>Difficult</strong> Airway Algorithm, which was<br />
<strong>in</strong>troduced to <strong>the</strong> anes<strong>the</strong>sia community <strong>in</strong> 1993 (Figure<br />
3) (4). S<strong>in</strong>ce its implementation <strong>in</strong> <strong>the</strong> United States,<br />
morbidity, mortality, and claims related to <strong>airway</strong> mis<strong>management</strong><br />
<strong>in</strong> <strong>the</strong> OR have fallen significantly (35).<br />
Unfortunately, <strong>the</strong> ASA algorithm has a number of<br />
characteristics that prevent direct application to <strong>the</strong> practice<br />
of Emergency Medic<strong>in</strong>e, because of dissimilarities <strong>in</strong><br />
<strong>airway</strong> <strong>management</strong> <strong>in</strong> <strong>the</strong> OR and <strong>the</strong> ED (Table 1). All<br />
<strong>airway</strong> <strong>management</strong> <strong>in</strong> <strong>the</strong> ED is urgent or emergent,<br />
often depriv<strong>in</strong>g <strong>the</strong> physician of <strong>the</strong> time necessary to<br />
evaluate <strong>the</strong> patient and plan this lifesav<strong>in</strong>g <strong>in</strong>tervention.<br />
Fur<strong>the</strong>rmore, each patient is presumed to have a full<br />
stomach <strong>in</strong> <strong>the</strong> ED, and <strong>the</strong>refore must undergo RSI, with<br />
its attendant time pressure and requirement for cricoid<br />
pressure, which may distort <strong>the</strong> view of <strong>the</strong> glottis. As<br />
noted above, <strong>the</strong> trauma patient presents unusual demands<br />
for <strong>airway</strong> <strong>management</strong>, <strong>in</strong>clud<strong>in</strong>g potential facial,<br />
cervical, and <strong>airway</strong> <strong>in</strong>jury, and cervical immobilization<br />
dur<strong>in</strong>g <strong>in</strong>tubation. In <strong>the</strong> ED, <strong>in</strong>tubation is<br />
conducted on <strong>the</strong> basis of patient need, whe<strong>the</strong>r for<br />
<strong>airway</strong> patency and protection or acute respiratory failure,<br />
whereas <strong>in</strong> <strong>the</strong> OR, patients are usually <strong>in</strong>tubated to<br />
guarantee <strong>airway</strong> protection and ventilation dur<strong>in</strong>g a<br />
reversible, pharmacologically ma<strong>in</strong>ta<strong>in</strong>ed unconscious<br />
state. This leads to a strong emphasis <strong>in</strong> <strong>the</strong> ASA algorithm<br />
on preserv<strong>in</strong>g <strong>the</strong> option of reemergence from<br />
anes<strong>the</strong>sia to resume spontaneous ventilation if difficulty<br />
is encountered (4). This approach is often impossible <strong>in</strong><br />
Emergency Medic<strong>in</strong>e because <strong>the</strong> patients’ pathology<br />
dictates that a def<strong>in</strong>itive <strong>airway</strong> be obta<strong>in</strong>ed by whatever<br />
means possible. F<strong>in</strong>ally, <strong>the</strong> orientation toward <strong>the</strong> surgical<br />
<strong>airway</strong> is different among anes<strong>the</strong>siologists and<br />
<strong>emergency</strong> physicians, as <strong>the</strong> latter generally have more<br />
tra<strong>in</strong><strong>in</strong>g <strong>in</strong> provision of cricothyrotomy (36).<br />
Can <strong>emergency</strong> physicians benefit from an algorithm<br />
similar to that of <strong>the</strong> ASA for <strong>management</strong> of <strong>the</strong> difficult<br />
<strong>airway</strong>? Perhaps. Walls, <strong>in</strong> his text on <strong>airway</strong> <strong>management</strong><br />
<strong>in</strong> <strong>the</strong> ED, recommends <strong>the</strong> use of a “Universal<br />
Algorithm” for emergent provision of <strong>the</strong> <strong>airway</strong>, along<br />
with several more specific algorithms for consideration<br />
<strong>in</strong> specific circumstances (“difficult <strong>airway</strong> algorithm,”<br />
“crash <strong>airway</strong> algorithm,” “failed <strong>airway</strong> algorithm”)<br />
(37). Although <strong>the</strong>se guidel<strong>in</strong>es lack prospective validation,<br />
<strong>the</strong>y represent a more appropriate application of<br />
pr<strong>in</strong>ciples and constra<strong>in</strong>ts to <strong>airway</strong> <strong>management</strong> <strong>in</strong> <strong>the</strong><br />
ED sett<strong>in</strong>g.<br />
Adjuncts for <strong>Difficult</strong> Airways<br />
Aside from <strong>the</strong> <strong>emergency</strong> surgical <strong>airway</strong> achieved by<br />
open or percutaneous cricothyrotomy, which has been<br />
effectively used by <strong>emergency</strong> physicians for difficult<br />
<strong>airway</strong> <strong>management</strong> for more than two decades, <strong>the</strong>re is<br />
a broad array of adjuncts to assist with ventilation or<br />
<strong>in</strong>tubation (34). When <strong>the</strong> patient can be ventilated by<br />
BVM, but not <strong>in</strong>tubated, <strong>the</strong>se adjuncts may be employed<br />
to facilitate placement of an endotracheal tube.<br />
Some of <strong>the</strong>se techniques are m<strong>in</strong>or modifications of
<strong>Difficult</strong> Airway Management 35<br />
Figure 3. American Society of Anes<strong>the</strong>siology <strong>Difficult</strong> Airway Management Guidel<strong>in</strong>e.<br />
direct laryngoscopy. There are non<strong>in</strong>vasive and <strong>in</strong>vasive<br />
techniques, bl<strong>in</strong>d techniques, and those <strong>in</strong>volv<strong>in</strong>g direct<br />
visualization. Some are effective for unforgiv<strong>in</strong>g anatomy,<br />
but less so for glottic or supraglottic pathology. A<br />
discussion of <strong>the</strong> various adjuncts, procedures, and devices<br />
follows, with particular emphasis on those most<br />
appropriate for <strong>the</strong> <strong>emergency</strong> practitioner. It is of paramount<br />
importance, however, that when ventilation by<br />
BVM fails after <strong>in</strong>ability to <strong>in</strong>tubate <strong>the</strong> trachea, one<br />
makes immediate preparations for provision of a surgical<br />
<strong>airway</strong> or transtracheal jet ventilation, because hypoxemia<br />
will rapidly occur (34,37,38).<br />
Blades for Direct Laryngoscopy<br />
A large variety of retraction blades for laryngoscopy are<br />
available. Although many variations of <strong>the</strong> curved and<br />
straight blade exist, <strong>the</strong> Miller and MacIntosh blades,<br />
<strong>in</strong>troduced about 50 years ago, rema<strong>in</strong> pre-em<strong>in</strong>ent
36 S. L. Orebaugh<br />
Table 1. Comparison of Airway Management <strong>in</strong> <strong>the</strong> ED and <strong>the</strong> OR<br />
Aspects of Airway<br />
Management Emergency Medic<strong>in</strong>e Anes<strong>the</strong>siology<br />
Goals Obta<strong>in</strong> def<strong>in</strong>itive <strong>airway</strong> Assure patent <strong>airway</strong> and ventilation while patient is unconscious<br />
Patient characteristics Always urgent or emergent Usually elective situation<br />
Frequent C-sp<strong>in</strong>e precautions Infrequent C-sp<strong>in</strong>e precautions<br />
Respiratory failure common Respiratory failure rare<br />
All presumed full stomach Usually NPO<br />
Usual preparatory time Seconds to m<strong>in</strong>utes Hours to days<br />
Alternatives for failed <strong>airway</strong> Must progress to def<strong>in</strong>itive <strong>airway</strong> Emphasis on awaken<strong>in</strong>g patient to secure awake <strong>airway</strong>,<br />
or cancel<br />
(39,40). Conventionally, <strong>the</strong> straight blade is <strong>in</strong>serted<br />
beneath <strong>the</strong> epiglottis and used to directly expose <strong>the</strong><br />
glottis, whereas <strong>the</strong> curved blade fits <strong>in</strong>to <strong>the</strong> vallecula,<br />
pull<strong>in</strong>g on <strong>the</strong> hypoepiglottic ligament as it is lifted, to<br />
flip <strong>the</strong> epiglottis out of <strong>the</strong> way, allow<strong>in</strong>g <strong>the</strong> operator to<br />
see <strong>the</strong> exposed glottis. Certa<strong>in</strong> situations, such as a very<br />
“deep” glottis, or protuberant “buck” teeth, seem to favor<br />
use of <strong>the</strong> straight blade (41). Some variants of <strong>the</strong> Miller<br />
blade, such as <strong>the</strong> Phillips blade, have a higher vertical<br />
profile, answer<strong>in</strong>g one of <strong>the</strong> deficiencies of this type of<br />
blade: excellent visualization but <strong>in</strong>adequate space for<br />
endotracheal tube <strong>in</strong>sertion (42). O<strong>the</strong>r varieties of laryngoscope<br />
blade that may prove useful <strong>in</strong> unusual situations<br />
<strong>in</strong>clude angled blades, blades with no vertical<br />
flange, and blades with mirrors (Table 2) (39,40,42–48).<br />
Most of <strong>the</strong>se are rarely used <strong>in</strong> cl<strong>in</strong>ical practice.<br />
Of recent <strong>in</strong>terest is a blade that can <strong>in</strong>corporate a<br />
prism for refraction, to improve <strong>the</strong> operator’s view of<br />
<strong>the</strong> larynx, and that also may be used without <strong>the</strong> prism<br />
for conventional laryngoscopy (45). Deemed <strong>the</strong> Belscope,<br />
it is a straight blade with a 45° angulation at its<br />
midpo<strong>in</strong>t, and is available <strong>in</strong> three sizes. This blade has<br />
been studied extensively by its orig<strong>in</strong>ator, for whom it is<br />
named, and applied successfully to normal anatomy and<br />
difficult <strong>airway</strong>s (49). The McCoy laryngoscope blade is<br />
Table 2. Selected Retraction Blades<br />
an articulat<strong>in</strong>g blade that allows one to lift <strong>the</strong> distal tip<br />
of <strong>the</strong> blade to improve <strong>the</strong> view of <strong>the</strong> glottis if <strong>the</strong><br />
epiglottis impedes visibility (47). This blade has been<br />
compared <strong>in</strong> several studies to <strong>the</strong> standard MacIntosh<br />
blade, and can improve <strong>the</strong> laryngoscopic grade significantly,<br />
but does not do so consistently (50,51). A doubleangled<br />
laryngoscope blade has been developed that comb<strong>in</strong>es<br />
features of both <strong>the</strong> straight and curved<br />
laryngoscope blade (46). Its utility rema<strong>in</strong>s unproven.<br />
Lastly, <strong>the</strong> “Improved View MacIntosh” blade allows an<br />
enhanced view of <strong>the</strong> larynx, due to a concavity <strong>in</strong> <strong>the</strong><br />
flat portion of <strong>the</strong> blade (48).<br />
Aids to Direct Laryngoscopy<br />
Aids to direct laryngoscopy <strong>in</strong>clude prisms, mirrors, and<br />
bougies, or Eschmann stylets. Initial use of <strong>the</strong> optical<br />
prism dates to <strong>the</strong> early 20th century, but little development<br />
of <strong>the</strong> technique occurred until <strong>the</strong> late 1960s, when<br />
Huffman described a prism made from Plexiglas for<br />
attachment to <strong>the</strong> vertical flange of <strong>the</strong> standard MacIntosh<br />
blade, which provides 20° of refraction (52). This<br />
helped <strong>the</strong> laryngoscopist ga<strong>in</strong> a view of <strong>the</strong> glottis when<br />
a grade 3 or grade 4 view was present, facilitat<strong>in</strong>g <strong>in</strong>tu-<br />
Blade Characteristics Uses/Advantages References<br />
Miller Straight, low vertical profile Normal <strong>airway</strong>s, long epiglottis<br />
Prom<strong>in</strong>ent <strong>in</strong>cisors, “deep” glottis<br />
39<br />
MacIntosh Curved blade Normal <strong>airway</strong>s 40<br />
Phillips Straight, higher vertical profile More room for ETT* placement than Miller<br />
blade offers<br />
42<br />
Bizzarri-Giuffrida Flangeless version of MacIntosh blade For small mouth or prom<strong>in</strong>ent teeth 44<br />
Siker Incorporates mirror <strong>in</strong>to blade Better visualization of anterior-situated<br />
larynx<br />
43<br />
Double-angle Blade has 20° and 30° angle bends Better exposure of anterior larynx 46<br />
Belscope Angulated, and has optional prism Can use for rout<strong>in</strong>e <strong>airway</strong>, or add prism 45<br />
McCoy Articulated, lever<strong>in</strong>g version of<br />
MacIntosh blade<br />
if poor visualization<br />
Moves fulcrum to lower pharynx to<br />
m<strong>in</strong>imize dental trauma <strong>in</strong> lift<strong>in</strong>g <strong>the</strong><br />
epiglottis<br />
Improved-view MacIntosh Concavity <strong>in</strong> blade Provides better view of anterior glottis 48<br />
* ETT, endotracheal tube<br />
47
<strong>Difficult</strong> Airway Management 37<br />
Figure 4. Gum elastic bougie, employed to facilitate <strong>in</strong>tubation<br />
of a poorly visualized glottic aperture (repr<strong>in</strong>ted with<br />
permission by Mosby-Year Book, Inc. (55)).<br />
bation. These prisms are available today at low cost and<br />
are easy to use, although fogg<strong>in</strong>g can be troublesome<br />
unless <strong>the</strong> device is warmed before use, and <strong>the</strong> prism<br />
reduces <strong>the</strong> room for manipulation of <strong>the</strong> endotrachael<br />
tube (ETT).<br />
Mirrors have been used to facilitate ETT placement<br />
when <strong>the</strong> glottis is difficult to visualize. These <strong>in</strong>clude<br />
blades with an <strong>in</strong>tegral mirror that provide an <strong>in</strong>verted<br />
view of <strong>the</strong> glottis, such as <strong>the</strong> Siker blade (43). The<br />
Neuste<strong>in</strong> blade <strong>in</strong>volves a mirrored attachment to <strong>the</strong><br />
MacIntosh balde that <strong>in</strong>cludes a guide channel for a<br />
stylet, over which <strong>the</strong> ETT is passed after <strong>the</strong> blade is<br />
removed (53). Both of <strong>the</strong>se devices result <strong>in</strong> an <strong>in</strong>verted<br />
image as viewed by <strong>the</strong> laryngoscopist, with some degree<br />
of <strong>in</strong>itial unfamiliarity mak<strong>in</strong>g <strong>the</strong>ir use cumbersome.<br />
Nei<strong>the</strong>r is frequently used <strong>in</strong> cl<strong>in</strong>ical practice.<br />
At times, it is beneficial to <strong>in</strong>sert a guid<strong>in</strong>g ca<strong>the</strong>ter, or<br />
bougie, <strong>in</strong>to <strong>the</strong> glottis, <strong>the</strong>n slide an ETT over it. The<br />
device thus provides a means to <strong>in</strong>tubate bl<strong>in</strong>dly dur<strong>in</strong>g<br />
direct laryngoscopy, when <strong>the</strong> glottis is not well visualized<br />
(54–56). The malleable Eschmann stylet, with its<br />
stiff, angulated end, lends itself to this task because it is<br />
small enough to be maneuverable <strong>in</strong> <strong>the</strong> pharynx, where<br />
it is used to “probe” for <strong>the</strong> glottic open<strong>in</strong>g, and its end<br />
is firm enough to rattle aga<strong>in</strong>st <strong>the</strong> tracheal r<strong>in</strong>gs as it is<br />
placed <strong>in</strong> <strong>the</strong> trachea, provid<strong>in</strong>g <strong>the</strong> <strong>in</strong>tubator a sense of<br />
correct placement (Figure 4). It is frequently used for<br />
difficult <strong>airway</strong> <strong>management</strong> <strong>in</strong> <strong>the</strong> ED <strong>in</strong> <strong>the</strong> U.K. (57).<br />
Little comparative data exist to support <strong>the</strong> use of <strong>the</strong><br />
Eschmann stylet <strong>in</strong> preference to o<strong>the</strong>r means of manag<strong>in</strong>g<br />
<strong>the</strong> <strong>airway</strong> <strong>in</strong> <strong>the</strong> ED, but numerous case reports and<br />
case series attest to its value <strong>in</strong> difficult <strong>in</strong>tubation <strong>in</strong> <strong>the</strong><br />
OR, and more recently <strong>in</strong> <strong>emergency</strong> practice (54–56).<br />
Interest <strong>in</strong> this low-cost, simple device appears to be<br />
<strong>in</strong>creas<strong>in</strong>g among <strong>emergency</strong> physicians. Moscati reported<br />
<strong>the</strong> efficacy of this device <strong>in</strong> three cases <strong>in</strong> <strong>the</strong> ED<br />
<strong>in</strong> which <strong>the</strong> glottic <strong>in</strong>let could not be visualized and<br />
<strong>in</strong>tubation by direct laryngoscopy had repeatedly failed<br />
(58).<br />
The recently <strong>in</strong>troduced Frova <strong>in</strong>tubat<strong>in</strong>g stylet (Cook<br />
Critical Care, Bloom<strong>in</strong>gton, IN, USA) similarly allows<br />
bl<strong>in</strong>d <strong>in</strong>tubation and passage of an ETT over <strong>the</strong> device,<br />
but is hollow and has an adaptor allow<strong>in</strong>g jet ventilation<br />
or oxygen <strong>in</strong>sufflation dur<strong>in</strong>g <strong>the</strong> <strong>in</strong>tubation. O<strong>the</strong>r devices<br />
also can be used as stylets, <strong>in</strong>clud<strong>in</strong>g <strong>airway</strong>exchange<br />
ca<strong>the</strong>ters, which permit attachment to an anes<strong>the</strong>tic<br />
circuit, resuscitation bag, or jet ventilation system.<br />
Use of a laryngotracheal anes<strong>the</strong>sia kit, with its plastic<br />
stylet, likewise has been described for this purpose (59).<br />
Bl<strong>in</strong>d Nasotracheal Intubation<br />
Bl<strong>in</strong>d nasotracheal <strong>in</strong>tubation (BNTI) rema<strong>in</strong>s a viable<br />
option for <strong>in</strong>tubation <strong>in</strong> <strong>the</strong> ED, <strong>in</strong> rout<strong>in</strong>e <strong>in</strong>tubation and<br />
difficult <strong>airway</strong> <strong>management</strong>. In <strong>the</strong> National Emergency<br />
Airway Registry study, this method was utilized <strong>in</strong> about<br />
5% of all <strong>in</strong>tubations, with a success rate of 85.7% with<strong>in</strong><br />
three attempts. In Dronen’s comparison of BNTI to direct<br />
laryngoscopy for <strong>in</strong>tubation, <strong>the</strong> rate of successful<br />
<strong>in</strong>tubation was significantly lower at 68%, <strong>in</strong> comparison<br />
to direct laryngoscopy with <strong>the</strong> use of succ<strong>in</strong>ylchol<strong>in</strong>e<br />
for muscle relaxation, with which <strong>the</strong>re were no failures<br />
(60). In addition, complication rates, mostly nasal bleed<strong>in</strong>g<br />
and emesis, were much higher with BNTI. When<br />
paramedics utilized BNTI <strong>in</strong> 219 <strong>in</strong>tubations, <strong>the</strong> rate of<br />
appropriate ETT placement improved from 58% to 72%<br />
when a directional tip control tube was utilized (61).<br />
Lighted and Optical Stylets<br />
Stylets have evolved <strong>in</strong> function, cost, and complexity. In<br />
<strong>the</strong> late 1950s, Yamamura described transillum<strong>in</strong>ation<br />
for use <strong>in</strong> nasotracheal <strong>in</strong>tubation (62). Use of <strong>the</strong> lighted<br />
stylet, or lightwand, has been well described s<strong>in</strong>ce <strong>the</strong>n,<br />
as a bl<strong>in</strong>d technique <strong>in</strong> <strong>the</strong> face of difficult <strong>in</strong>tubation, as<br />
well as for rout<strong>in</strong>e <strong>airway</strong> <strong>management</strong> (63–65). Early<br />
commercial lightwands suffered from poor illum<strong>in</strong>ation<br />
and misdirection of <strong>the</strong> light, so that a darkened room<br />
was necessary to see <strong>the</strong> halo produced <strong>in</strong> <strong>the</strong> glottic area<br />
dur<strong>in</strong>g <strong>in</strong>sertion <strong>in</strong>to <strong>the</strong> <strong>airway</strong>. The lamp switch was
38 S. L. Orebaugh<br />
often placed <strong>in</strong> an awkward position. Fur<strong>the</strong>r, an overly<br />
rigid stylet could cause retraction of <strong>the</strong> ETT out of <strong>the</strong><br />
glottis when <strong>the</strong> lightwand was withdrawn (63). Newer<br />
models have improved upon visibility of <strong>the</strong> light as well<br />
as <strong>the</strong> ergonomics of <strong>the</strong> device (66). The Trachlite<br />
(Laerdahl, Long Beach, CA, USA), a two-piece lighted<br />
stylet, allows <strong>the</strong> ETT to be placed without dislodg<strong>in</strong>g it<br />
when <strong>the</strong> device is withdrawn, due to a retractable wire<br />
stylet. A lock<strong>in</strong>g device for <strong>the</strong> proximal portion of <strong>the</strong><br />
ETT and an adjustable length stylet also represent significant<br />
improvements of <strong>the</strong> Trachlite over earlier<br />
lighted stylets (66).<br />
In <strong>the</strong> OR, lighted stylet <strong>in</strong>tubation has proven reliable<br />
and highly successful. A<strong>in</strong>sworth described <strong>in</strong>tubation <strong>in</strong><br />
200 patients under general anes<strong>the</strong>sia with<strong>in</strong> 60 sec,<br />
whereas Weiss reported a series of 250 patients with<br />
99% success <strong>in</strong> <strong>in</strong>tubation us<strong>in</strong>g <strong>the</strong> lighted stylet<br />
(65,67). In 950 surgical patients, use of <strong>the</strong> Trachlite<br />
illum<strong>in</strong>at<strong>in</strong>g stylet was compared to direct laryngoscopy<br />
for efficacy <strong>in</strong> tracheal <strong>in</strong>tubation (66). Direct laryngoscopy<br />
was found to require more time, produce more<br />
complications, and result <strong>in</strong> a higher failure rate (3% vs.<br />
1%). In 186 documented or suspected difficult <strong>airway</strong>s,<br />
Hung utilized <strong>the</strong> lighted sylet for <strong>in</strong>tubation at <strong>the</strong><br />
<strong>in</strong>duction of anes<strong>the</strong>sia with success <strong>in</strong> 99% of <strong>the</strong>se<br />
patients (68). In a series of 28 trauma patients with<br />
suspected cervical sp<strong>in</strong>e <strong>in</strong>jury, <strong>the</strong> lightwand was employed<br />
for <strong>in</strong>tubation with 100% success as reported by<br />
Weiss (69). In prehospital care, Vollmer reported <strong>the</strong> use<br />
of <strong>the</strong> lighted stylet by Emergency Medic<strong>in</strong>e residents <strong>in</strong><br />
24 patients with 88% success <strong>in</strong> less than 45 sec (70).<br />
In Emergency Medic<strong>in</strong>e, lighted stylets have also<br />
proven useful for <strong>airway</strong> managment <strong>in</strong> facial trauma,<br />
and appear to facilitate <strong>in</strong>tubation while preserv<strong>in</strong>g immobility<br />
of <strong>the</strong> cervical sp<strong>in</strong>e (70,71). The device has<br />
been adapted for nasotracheal <strong>in</strong>tubation as well as orotracheal<br />
use (70). Complications are <strong>in</strong>frequent with use<br />
of <strong>the</strong> lighted stylet (63).<br />
Stylets have been modified to <strong>in</strong>clude optical view<strong>in</strong>g<br />
fibers as well as light<strong>in</strong>g. Such stylets may be used for<br />
rout<strong>in</strong>e or difficult tracheal <strong>in</strong>tubation (73–75). These<br />
devices allow direct visualization of structures at <strong>the</strong> tip<br />
of <strong>the</strong> endotracheal tube as it is <strong>in</strong>serted, simplify<strong>in</strong>g<br />
<strong>in</strong>tubation when a poor laryngoscopic grade is encountered,<br />
and facilitat<strong>in</strong>g confirmation of tube placement.<br />
Some of <strong>the</strong> available <strong>in</strong>struments display <strong>the</strong> image on<br />
a video screen at <strong>the</strong> bedside, while o<strong>the</strong>rs require <strong>the</strong><br />
operator to look through an objective lens as <strong>the</strong> device<br />
is <strong>in</strong>serted <strong>in</strong>to <strong>the</strong> <strong>airway</strong> (73,74). These <strong>in</strong>struments are<br />
best used <strong>in</strong> conjunction with a laryngoscope or <strong>the</strong> hand<br />
of an assistant to elevate <strong>the</strong> mandible and soft tissues<br />
out of <strong>the</strong> way for optimum visualization. Limitations<br />
<strong>in</strong>clude potential fogg<strong>in</strong>g and <strong>in</strong>terference with <strong>the</strong> view<br />
by secretions, <strong>the</strong> need to become familiar with view<strong>in</strong>g<br />
characteristics, and <strong>the</strong> cost of <strong>the</strong> devices, which is<br />
considerable.<br />
The <strong>in</strong>tubat<strong>in</strong>g fiberoptic stylet has not been subjected<br />
to controlled, comparative studies <strong>in</strong> <strong>the</strong> <strong>management</strong> of<br />
<strong>the</strong> difficult <strong>airway</strong>. However, <strong>in</strong> small series, it has<br />
proven useful for <strong>airway</strong> <strong>management</strong> <strong>in</strong> <strong>the</strong> OR. In 32<br />
patients undergo<strong>in</strong>g general anes<strong>the</strong>sia for surgery, 94%<br />
of cases were <strong>in</strong>tubated successfully on <strong>the</strong> first attempt<br />
and <strong>the</strong> rema<strong>in</strong>der on <strong>the</strong> second attempt us<strong>in</strong>g this<br />
device (74). Gravenste<strong>in</strong> compared <strong>the</strong> fiberoptic stylet<br />
with direct laryngoscopy and with bronchoscopic <strong>in</strong>tubation<br />
<strong>in</strong> 75 patients under general anes<strong>the</strong>sia, evaluat<strong>in</strong>g<br />
<strong>the</strong> time required for <strong>in</strong>tubation, <strong>the</strong> quality of <strong>the</strong> view<br />
of <strong>the</strong> glottis, and <strong>the</strong> frequency of complications (75).<br />
The authors reported a shorter time for <strong>in</strong>tubation us<strong>in</strong>g<br />
<strong>the</strong> fiberoptic stylet than for <strong>the</strong> bronchoscope, and a<br />
lower rate of postoperative sore throat than direct laryngoscopy,<br />
but also noted that <strong>the</strong> least favorable laryngoscopic<br />
view occurred with <strong>the</strong> fiberoptic stylet. When<br />
compared to conventional <strong>in</strong>tubation with direct laryngoscopy<br />
utiliz<strong>in</strong>g an Eschman stylet <strong>in</strong> simulated grade 3<br />
laryngoscopy <strong>in</strong> a mannequ<strong>in</strong> model, Biro described<br />
100% success us<strong>in</strong>g <strong>the</strong> fiberoptic <strong>in</strong>tubat<strong>in</strong>g stylet <strong>in</strong><br />
tracheal tube placement by 45 anes<strong>the</strong>tists <strong>in</strong> 225 <strong>in</strong>tubations,<br />
whereas <strong>the</strong>re was a 40% rate of tube misplacement<br />
(20% esophageal, 20% endobronchial) utiliz<strong>in</strong>g<br />
direct laryngoscopy under <strong>the</strong>se circumstances (76).<br />
Aids to Ventilation<br />
Occasionally, <strong>the</strong> <strong>emergency</strong> physician will attempt RSI,<br />
only to f<strong>in</strong>d that <strong>in</strong>tubation is impossible due to abnormal<br />
anatomy, pathology, or poor visibility. Much less frequently,<br />
ventilation by mask will fail <strong>in</strong> <strong>the</strong> same patient,<br />
despite attempts to optimize it (17). When both of <strong>the</strong>se<br />
conditions are met, desaturation and hypercarbia will<br />
occur with<strong>in</strong> m<strong>in</strong>utes, or possibly seconds, depend<strong>in</strong>g on<br />
<strong>the</strong> degree of preoxygenation, <strong>the</strong> patient’s body mass,<br />
current oxygen utilization, and associated cardiopulmonary<br />
pathology (34). Cricothyrotomy or transtracheal jet<br />
ventilation should be quickly carried out, but an adjunct<br />
to ventilation may be utilized to temporize while preparations<br />
for <strong>the</strong> more <strong>in</strong>vasive procedure are made. Aids to<br />
ventilation are placed <strong>in</strong> ei<strong>the</strong>r <strong>the</strong> supraglottic or <strong>in</strong>fraglottic<br />
<strong>airway</strong>, depend<strong>in</strong>g upon <strong>the</strong> cl<strong>in</strong>ical situation.<br />
The laryngeal mask <strong>airway</strong> (LMA) (LMA of North<br />
America) has been <strong>in</strong> widespread use by anes<strong>the</strong>siologists<br />
<strong>in</strong> Europe s<strong>in</strong>ce <strong>the</strong> 1980s, when it was developed<br />
by Bra<strong>in</strong> (77). It was <strong>in</strong>troduced <strong>in</strong> <strong>the</strong> U.S. <strong>in</strong> <strong>the</strong> early<br />
1990s, and is utilized worldwide for <strong>the</strong> conduct of<br />
anes<strong>the</strong>sia. The device is composed of a semirigid tube<br />
attached to an <strong>in</strong>flatable “mask” that is placed <strong>in</strong>to <strong>the</strong><br />
hypopharynx, and advanced over <strong>the</strong> larynx. When <strong>in</strong>-
<strong>Difficult</strong> Airway Management 39<br />
flated, this mask provides a seal around <strong>the</strong> glottic aperture<br />
(78). The LMA is available as a reusable device as<br />
well as a disposable one, <strong>in</strong> sizes rang<strong>in</strong>g from those for<br />
neonates to those for large adults.<br />
LMA <strong>in</strong>sertion requires skill, practice, and familiarity<br />
with <strong>the</strong> conformation of <strong>the</strong> device (77). However, it<br />
may be <strong>in</strong>serted without muscle relaxants, and lends<br />
itself to <strong>emergency</strong> ventilation, because it provides a<br />
greater degree of <strong>airway</strong> patency than does a face mask.<br />
The LMA has been utilized as an <strong>emergency</strong> ventilation<br />
adjunct <strong>in</strong> a variety of circumstances (78–80). It also can<br />
be used effectively as a “bridge” to fiberoptic <strong>in</strong>tubation,<br />
because an ETT of size 6.0 or smaller may be passed<br />
through <strong>the</strong> LMA and over <strong>the</strong> fiberscope, while <strong>the</strong><br />
lumen of <strong>the</strong> device effectively guides <strong>the</strong> bronchoscopist<br />
to <strong>the</strong> laryngeal open<strong>in</strong>g (79–81). Limitations <strong>in</strong>clude<br />
a seal that is unreliable at high peak <strong>in</strong>spiratory<br />
<strong>airway</strong> pressures: about one-third of <strong>the</strong> tidal volume is<br />
lost dur<strong>in</strong>g positive pressure ventilation with <strong>the</strong> LMA<br />
when <strong>the</strong> peak <strong>in</strong>spiratory pressure reaches 30 cm of<br />
H 2O, and <strong>the</strong> effectiveness of ventilation deteriorates<br />
fur<strong>the</strong>r as peak <strong>airway</strong> pressures <strong>in</strong>crease (82). Failure to<br />
protect <strong>the</strong> patient aga<strong>in</strong>st aspiration of gastric contents is<br />
ano<strong>the</strong>r concern. Mucosal trauma may occur on <strong>in</strong>sertion<br />
of <strong>the</strong> LMA, and placement is occasionally difficult,<br />
particularly for <strong>the</strong> unfamiliar operator (77–80). A new<br />
version of <strong>the</strong> LMA, which soon will be <strong>in</strong>troduced <strong>in</strong> <strong>the</strong><br />
U.S., will have a port for gastric empty<strong>in</strong>g (83).<br />
The LMA has proven useful both as an alternative to<br />
BVM <strong>in</strong> cardiopulmonary arrest and as a rescue device <strong>in</strong><br />
difficult <strong>airway</strong> <strong>management</strong>. Among <strong>in</strong>tensive care unit<br />
nurses, Mart<strong>in</strong> found that <strong>the</strong> LMA proved easier to use,<br />
and provided a better tidal volume with less likelihood of<br />
<strong>airway</strong> obstruction than BVM ventilation with or without<br />
an oral <strong>airway</strong> (84). When untra<strong>in</strong>ed volunteers were<br />
assessed for <strong>the</strong> ability to ventilate patients under general<br />
anes<strong>the</strong>sia, Alexander described marked improvement <strong>in</strong><br />
success of ventilation and oxygenation when <strong>the</strong> LMA<br />
was used, compared to BVM ventilation (85). He reported<br />
a 43% rate of failure to ventilate effectively with<br />
<strong>the</strong> latter device, whereas <strong>the</strong> LMA was successful <strong>in</strong> all<br />
but 13% of cases. Likewise, Smith found that anes<strong>the</strong>tists<br />
were better able to ma<strong>in</strong>ta<strong>in</strong> oxygen saturation and a<br />
patent <strong>airway</strong> <strong>in</strong> 64 patients under general anes<strong>the</strong>sia<br />
randomly assigned to ventilation us<strong>in</strong>g <strong>the</strong> LMA as opposed<br />
to a face mask (86).<br />
In an evaluation of LMA utility <strong>in</strong> prehospital care,<br />
Pennant described placement of LMA by paramedics <strong>in</strong><br />
100% of cases <strong>in</strong> less than 40 sec, whereas endotracheal<br />
tube placement required more than twice that long and<br />
resulted <strong>in</strong> 31% misplacement (87). Davies described<br />
placement of an ETT or LMA <strong>in</strong> a mannequ<strong>in</strong> by paramedics<br />
with little tra<strong>in</strong><strong>in</strong>g: 94% of LMA <strong>in</strong>sertions were<br />
successful, compared to only 51% of ETT <strong>in</strong>sertions<br />
(88).<br />
Little comparative cl<strong>in</strong>ical data exist to support use of<br />
<strong>the</strong> LMA <strong>in</strong> <strong>the</strong> ED. It has been well established dur<strong>in</strong>g<br />
difficult <strong>airway</strong> <strong>management</strong> and rescue ventilation <strong>in</strong><br />
<strong>the</strong> OR (79–81). Experienced practitioners can usually<br />
<strong>in</strong>sert <strong>the</strong> LMA with<strong>in</strong> 20 s, with a success rate of<br />
ventilation of 98% (89). Parnet described <strong>the</strong> use of <strong>the</strong><br />
device as <strong>the</strong> adjunct of first choice by academic anes<strong>the</strong>siologists<br />
fac<strong>in</strong>g difficult-<strong>in</strong>tubation or difficult-ventilation<br />
situations <strong>in</strong> 17 cases over 2 years, with a 94%<br />
success rate, whereas o<strong>the</strong>r modalities were significantly<br />
less successful (90). Only one case report has been<br />
published to date describ<strong>in</strong>g failure of <strong>the</strong> LMA <strong>in</strong> a<br />
cannot-<strong>in</strong>tubate/cannot-ventilate situation (91). Thus, <strong>the</strong><br />
considerable experience with <strong>the</strong> LMA <strong>in</strong> unexpected<br />
difficult <strong>airway</strong> <strong>management</strong> <strong>in</strong> <strong>the</strong> OR may substantiate<br />
an attempt at its use when consider<strong>in</strong>g a surgical <strong>airway</strong><br />
for <strong>the</strong> failed <strong>airway</strong> <strong>in</strong> <strong>the</strong> ED because it can be <strong>in</strong>serted<br />
so quickly and with high expectation of success (92). Its<br />
use may allow <strong>the</strong> conduct of an orderly, composed<br />
surgical <strong>airway</strong>, as opposed to a very hastened procedure<br />
<strong>in</strong> a desaturat<strong>in</strong>g patient.<br />
In a meta-analysis of <strong>the</strong> literature, Brimacombe<br />
found that <strong>the</strong> <strong>in</strong>cidence of reported aspiration of gastric<br />
contents dur<strong>in</strong>g use of <strong>the</strong> LMA is exceed<strong>in</strong>gly low, on<br />
<strong>the</strong> order of 2/10,000 cases, a rate similar to that encountered<br />
with general anes<strong>the</strong>sia with <strong>the</strong> use of a cuffed<br />
endotracheal tube (93). A new model of <strong>the</strong> LMA, recently<br />
<strong>in</strong>troduced, <strong>in</strong>corporates a dorsal cuff, a dra<strong>in</strong>age<br />
tube for <strong>in</strong>sertion of a gastric tube, a double cuff configuration,<br />
and an <strong>in</strong>troducer device. The Proseal LMA<br />
(Laryngeal Mask Company, Henley-on-Thames, UK)<br />
has been evaluated <strong>in</strong> a randomized, crossover study <strong>in</strong><br />
anes<strong>the</strong>tized patients, <strong>in</strong> which it was compared to <strong>the</strong><br />
LMA (94). The authors reported 100% success with<br />
both devices, but noted that <strong>the</strong> LMA was judged<br />
easier to <strong>in</strong>sert, and could be placed more quickly,<br />
with higher success on <strong>the</strong> first attempt. A gastric tube<br />
was placed successfully through <strong>the</strong> Proseal LMA <strong>in</strong><br />
all cases.<br />
The <strong>in</strong>tubat<strong>in</strong>g laryngeal mask <strong>airway</strong> (ILMA) (Fastrach,<br />
LMA of North America, Long Beach, CA, USA)<br />
is a derivation of <strong>the</strong> LMA that facilitates endotracheal<br />
<strong>in</strong>tubation after placement of a laryngeal mask and which<br />
has some features dist<strong>in</strong>ct from <strong>the</strong> conventional one.<br />
The laryngeal mask is attached to a rigid sta<strong>in</strong>less-steel<br />
<strong>airway</strong> tube, which has a larger <strong>in</strong>ternal diameter than <strong>the</strong><br />
standard adult LMAs, and which has a handle to ease<br />
placement. This tube admits a flexible, re<strong>in</strong>forced endotracheal<br />
tube specially manufactured for this laryngeal<br />
mask. The mask and tracheal tubes come <strong>in</strong> three sizes<br />
for adults.<br />
The ILMA has received significant study <strong>in</strong> anes<strong>the</strong>-
40 S. L. Orebaugh<br />
siology, but little <strong>in</strong> <strong>the</strong> ED. None<strong>the</strong>less, <strong>the</strong> device has<br />
promise for manag<strong>in</strong>g <strong>the</strong> difficult <strong>airway</strong> <strong>in</strong> ei<strong>the</strong>r sett<strong>in</strong>g.<br />
The enormous popularity of <strong>the</strong> LMA <strong>in</strong> Europe and<br />
o<strong>the</strong>r areas around <strong>the</strong> world has led to ready acceptance<br />
of <strong>the</strong> ILMA. In Australia, Agro described its use <strong>in</strong> 110<br />
patients slated for general anes<strong>the</strong>sia, with 95% success<br />
<strong>in</strong> establish<strong>in</strong>g ventilation through <strong>the</strong> laryngeal mask<br />
(95). However, <strong>the</strong> authors encountered resistance to<br />
ETT <strong>in</strong>sertion, requir<strong>in</strong>g some form of adjustment of <strong>the</strong><br />
apparatus, <strong>in</strong> 60% of patients, with an <strong>in</strong>tubation time<br />
averag<strong>in</strong>g 79 s. In a multicenter study from <strong>the</strong> U.K.,<br />
Baskett assessed <strong>the</strong> efficacy of <strong>the</strong> ILMA <strong>in</strong> <strong>in</strong>tubation<br />
of 500 patients undergo<strong>in</strong>g general anes<strong>the</strong>sia, aga<strong>in</strong> with<br />
95% success <strong>in</strong> ventilation through <strong>the</strong> mask portion of<br />
<strong>the</strong> device (96). The authors had 80% success on <strong>the</strong><br />
first <strong>in</strong>tubation attempts, with 4% of patients requir<strong>in</strong>g<br />
three attempts and a failure rate of 4%. In ano<strong>the</strong>r report<br />
from Brita<strong>in</strong>, Bra<strong>in</strong> used <strong>the</strong> ILMA to attempt <strong>in</strong>tubation<br />
of 150 patients undergo<strong>in</strong>g general anes<strong>the</strong>sia, with success<br />
<strong>in</strong> ventilat<strong>in</strong>g all of <strong>the</strong> patients with <strong>the</strong> laryngeal<br />
mask (97). In half of patients, resistance to ETT placement<br />
was encountered, requir<strong>in</strong>g one of several adjust<strong>in</strong>g<br />
maneuvers before <strong>in</strong>tubation was successful. The study<br />
<strong>in</strong>cluded 13 patients with “potential or known” <strong>airway</strong><br />
difficulty, all of whom were <strong>in</strong>tubated successfully. A<br />
slate of four different adjust<strong>in</strong>g maneuvers is described,<br />
based upon <strong>the</strong> level at which resistance to ETT advancement<br />
is encountered (97). In 38 patients with known<br />
difficult <strong>airway</strong>s, based on historical failure of laryngoscopy<br />
or physical exam<strong>in</strong>ation features predict<strong>in</strong>g difficulty,<br />
Joo assessed <strong>the</strong> utility of <strong>the</strong> ILMA compared to<br />
awake <strong>in</strong>tubation with <strong>the</strong> fiberoptic bronchoscope<br />
(FOB) (98). All awake FOB attempts were successful,<br />
but only half of patients could be <strong>in</strong>tubated bl<strong>in</strong>dly with<br />
<strong>the</strong> ILMA. The o<strong>the</strong>r half required <strong>the</strong> use of a bronchoscope,<br />
and 10% required <strong>in</strong>volvement of a second operator<br />
to place <strong>the</strong> ETT.<br />
Less data exist that evaluate <strong>the</strong> ILMA for <strong>airway</strong><br />
<strong>management</strong> <strong>in</strong> <strong>the</strong> ED. Asai, simulat<strong>in</strong>g trauma resuscitation<br />
with manual <strong>in</strong>-l<strong>in</strong>e immobilization of <strong>the</strong> cervical<br />
sp<strong>in</strong>e <strong>in</strong> anes<strong>the</strong>tized patients, evaluated <strong>the</strong> ILMA<br />
for <strong>in</strong>tubation <strong>in</strong> 40 cases (99). The ILMA was used <strong>in</strong><br />
conjunction with FOB to ensure correct placement, and<br />
this tandem was compared to direct laryngoscopy with<br />
use of an Eschmann stylet. The authors reported 85%<br />
success of <strong>in</strong>tubation with <strong>the</strong> ILMA under <strong>the</strong>se circumstances,<br />
but less than half of <strong>the</strong> patients <strong>in</strong> <strong>the</strong> laryngoscopy<br />
group were successfully <strong>in</strong>tubated with <strong>the</strong>se restrictions.<br />
Rosenblatt reported three cases of successful<br />
<strong>in</strong>tubation with <strong>the</strong> ILMA <strong>in</strong> patients <strong>in</strong> whom direct<br />
laryngoscopy had failed <strong>in</strong> <strong>the</strong> ED (100). The authors<br />
commented of <strong>the</strong> ILMA that “proficiency <strong>in</strong> its use<br />
requires practice under controlled conditions,” and suggested<br />
that “<strong>the</strong> <strong>emergency</strong> physician seek out elective<br />
practice” before assum<strong>in</strong>g it can be used successfully<br />
under emergent circumstances.<br />
Some authors have attempted to study <strong>the</strong> utility of<br />
<strong>the</strong> ILMA <strong>in</strong> <strong>the</strong> hands of unskilled or <strong>in</strong>experienced<br />
operators, as might occur among paramedics or nurses<br />
dur<strong>in</strong>g resuscitation attempts. When use of <strong>the</strong> ILMA<br />
was evaluated among untra<strong>in</strong>ed <strong>airway</strong> operators, and<br />
compared with <strong>the</strong>ir ability to perform direct laryngoscopy<br />
and <strong>in</strong>tubation <strong>in</strong> a random cross-over trial <strong>in</strong>volv<strong>in</strong>g<br />
anes<strong>the</strong>tized patients, Avidan found that <strong>the</strong> participants<br />
performed poorly with each device, with a 35–40%<br />
overall success <strong>in</strong> <strong>in</strong>tubation (101). In a cadaver study,<br />
medical students were assessed <strong>in</strong> <strong>the</strong>ir ability to ventilate<br />
with <strong>the</strong> ILMA or <strong>the</strong> LMA (102). The authors found<br />
that <strong>the</strong> students could more effectively ventilate with <strong>the</strong><br />
ILMA than <strong>the</strong> LMA (92% vs. 76%, respectively). However,<br />
<strong>the</strong>y could <strong>in</strong>tubate successfully with <strong>the</strong> ILMA <strong>in</strong><br />
only 67% of cases. Thus, <strong>the</strong> ILMA may be preferred to<br />
<strong>the</strong> LMA for <strong>emergency</strong> ventilation <strong>in</strong> <strong>the</strong> ED, given its<br />
higher success rate and its potential for convert<strong>in</strong>g ventilation<br />
to <strong>in</strong>tubation of <strong>the</strong> trachea. However, <strong>in</strong>tubation<br />
through <strong>the</strong> device requires practice and familiarity, and<br />
is not met with a high degree of success <strong>in</strong> <strong>the</strong> neophyte.<br />
Fur<strong>the</strong>rmore, <strong>the</strong> device is much more expensive than <strong>the</strong><br />
disposable LMA.<br />
The esophageal-tracheal combitube (ETC) (Sheridan<br />
Ca<strong>the</strong>ter Corporation, Argyle, NY, USA) is ano<strong>the</strong>r <strong>airway</strong><br />
rescue device that facilitates ventilation by br<strong>in</strong>g<strong>in</strong>g<br />
<strong>the</strong> source of oxygen closer to <strong>the</strong> glottis than does <strong>the</strong><br />
standard face mask. This dual lumen tube is generally<br />
<strong>in</strong>serted bl<strong>in</strong>dly <strong>in</strong>to <strong>the</strong> pharynx, and is <strong>the</strong>n advanced<br />
<strong>in</strong>to ei<strong>the</strong>r <strong>the</strong> esophagus (95–99% of cases) or <strong>the</strong> trachea<br />
(103). Ventilation through <strong>the</strong> color-coded, numbered<br />
tubes is <strong>the</strong>n employed to determ<strong>in</strong>e <strong>the</strong> position of<br />
<strong>the</strong> tube. The ETC enjoys more popularity <strong>in</strong> <strong>the</strong> <strong>emergency</strong><br />
sett<strong>in</strong>g than <strong>the</strong> LMA <strong>in</strong> <strong>the</strong> U.S. (104,105).<br />
The ETC has been used effectively <strong>in</strong> rout<strong>in</strong>e and<br />
emergent <strong>airway</strong> <strong>management</strong> <strong>in</strong> anes<strong>the</strong>sia, <strong>in</strong> prehospital<br />
<strong>airway</strong> <strong>management</strong>, <strong>in</strong> cardiopulmonary resuscitation,<br />
and <strong>in</strong> <strong>the</strong> ED <strong>management</strong> of difficult <strong>airway</strong>s<br />
(103,105–107). The ETC has been shown to be a reliable<br />
device for prolonged mechanical ventilation <strong>in</strong> ICU patients<br />
(108). Dur<strong>in</strong>g cardiac arrest, this device has proven<br />
efficacious to provide adequate ventilation with shorter<br />
<strong>in</strong>tubation times than standard direct laryngoscopy (109).<br />
Critical care nurses were able to ventilate with <strong>the</strong> ETC<br />
dur<strong>in</strong>g resuscitations as effectively as physicians <strong>in</strong>tubat<strong>in</strong>g<br />
<strong>the</strong>se patients (107). Among prehospital providers<br />
not tra<strong>in</strong>ed to <strong>in</strong>tubate <strong>the</strong> trachea, a modified, randomized,<br />
cross-over study design was used to compare <strong>the</strong><br />
ease of <strong>in</strong>sertion and adequacy of ventilation among <strong>the</strong><br />
ETC, LMA, and pharyngeal tracheal lumen <strong>airway</strong><br />
(105). Successful <strong>in</strong>sertion and ventilation occurred more
<strong>Difficult</strong> Airway Management 41<br />
frequently with <strong>the</strong> ETC than with <strong>the</strong> o<strong>the</strong>r two devices,<br />
and was preferred by this group of providers.<br />
Indications for use of <strong>the</strong> ETC <strong>in</strong>clude predicted difficult<br />
<strong>airway</strong> and <strong>in</strong>ability to visualize <strong>the</strong> glottis dur<strong>in</strong>g<br />
direct laryngoscopy (103,104,106). This adjunct may be<br />
<strong>in</strong>serted with <strong>the</strong> use of a laryngoscope as well as bl<strong>in</strong>dly.<br />
Advantages of <strong>the</strong> ETC <strong>in</strong>clude <strong>the</strong> potential for reduced<br />
risk of aspiration when compared to a face mask or <strong>the</strong><br />
LMA, preservation of cervical sp<strong>in</strong>e immobilization, and<br />
<strong>the</strong> ability to <strong>in</strong>sert <strong>the</strong> device when a laryngoscope is not<br />
available (103–106). The relatively large size of <strong>the</strong> ETC<br />
and its <strong>in</strong>herent stiffness predispose to esophageal dilatation,<br />
and lacerations of <strong>the</strong> piriform s<strong>in</strong>us and esophagus<br />
have been reported (110,111).<br />
Transtracheal Jet Ventilation<br />
At times, <strong>the</strong> ETC and LMA are rendered <strong>in</strong>effectual by<br />
supraglottic or glottic pathology, such as swell<strong>in</strong>g, abscess,<br />
tumor or foreign body, or by unfavorable anatomy<br />
that precludes <strong>the</strong>ir placement, such as limited mouth<br />
open<strong>in</strong>g. Under such circumstances, an approach to<br />
emergent ventilation that utilizes an <strong>in</strong>fraglottic, percutaneous<br />
route is an alternative. Transtracheal “jet” ventilation<br />
(TTJV) requires <strong>the</strong> placement of a large-bore<br />
i.v. or o<strong>the</strong>r ca<strong>the</strong>ter through <strong>the</strong> cricothyroid membrane,<br />
or even directly <strong>in</strong>to <strong>the</strong> trachea (12,113). This is connected,<br />
preferably by a tight-fitt<strong>in</strong>g luer-lock connection,<br />
to a high-pressure oxygen source, which is used to oxygenate<br />
and ventilate <strong>the</strong> patient (114,115). The ca<strong>the</strong>ter<br />
also may be attached to a resuscitation bag via <strong>the</strong><br />
connector of a size 3 ETT or to wall oxygen from a<br />
regulator at its highest flow, utiliz<strong>in</strong>g a hole cut <strong>in</strong> <strong>the</strong><br />
tub<strong>in</strong>g to control flow of oxygen by periodic occlusion<br />
with <strong>the</strong> thumb or f<strong>in</strong>ger (116,117). These arrangements<br />
do not provide ventilation as effectively as does a high<br />
pressure (50 PSI) oxygen source, which may be delivered<br />
ei<strong>the</strong>r by an oxygen tank with a “step down” regulator<br />
or directly by <strong>the</strong> hospital’s wall oxygen system<br />
(112,118). A variety of components can be assembled<br />
piecemeal to create such a system, but commercially<br />
available systems are more reliable and are reasonably<br />
priced (112,119).<br />
When oxygen at high pressure (20–50 PSI) and high<br />
flow (0.5–1.0 L/sec) is delivered by TTJV, air may be<br />
entra<strong>in</strong>ed at <strong>the</strong> ca<strong>the</strong>ter tip, augment<strong>in</strong>g <strong>the</strong> tidal volume<br />
and <strong>in</strong>creas<strong>in</strong>g <strong>the</strong> risk of barotrauma. Given <strong>the</strong> low<br />
rates and high pressures <strong>in</strong>volved, adequate tidal volume<br />
for an adult usually can be delivered <strong>in</strong> 0.5–1 sec. Utiliz<strong>in</strong>g<br />
a lung model with a set compliance of 50 mL/cm<br />
H 20, a 1-sec <strong>in</strong>spiratory time and a 50 PSI oxygen<br />
source, tidal volumes generated vary from about 600 mL<br />
with an 18-gauge i.v. ca<strong>the</strong>ter to over 1200 mL with a<br />
14-gauge ca<strong>the</strong>ter (112).<br />
TTJV was demonstrated to be successful <strong>in</strong> provid<strong>in</strong>g<br />
adequate ventilation <strong>in</strong> cardiac arrest patients as early as<br />
1972, when Jacobs described its use <strong>in</strong> 40 cases (116).<br />
While utiliz<strong>in</strong>g a high-pressure oxygen source, <strong>the</strong> author<br />
was able to ma<strong>in</strong>ta<strong>in</strong> an average pO 2 of 300 mm Hg, and<br />
a pCO 2 of 22 mm Hg with peak <strong>airway</strong> pressures of<br />
15–25 cm H 2O. Smith <strong>in</strong> 1975 described <strong>the</strong> use of TTJV<br />
<strong>in</strong> 80 patients who underwent <strong>airway</strong> surgery under anes<strong>the</strong>sia<br />
(120). Fifty-two of <strong>the</strong>se cases <strong>in</strong>volved elective<br />
use of <strong>the</strong> technique, while 28 of <strong>the</strong> patients were<br />
managed while <strong>in</strong> respiratory distress. Provided that adequate<br />
pressures are utilized to provide necessary flow<br />
rates, numerous <strong>in</strong>vestigators have demonstrated that<br />
normocarbia can be ma<strong>in</strong>ta<strong>in</strong>ed while ventilat<strong>in</strong>g patients<br />
with this technique (115,116). Most of <strong>the</strong> patients described<br />
<strong>in</strong> <strong>the</strong>se <strong>in</strong>vestigations were under general anes<strong>the</strong>sia,<br />
<strong>in</strong> contrast to patients <strong>in</strong> acute respiratory failure<br />
who are frequently encountered <strong>in</strong> <strong>the</strong> ED. TTJV also has<br />
been useful <strong>in</strong> high-grade upper <strong>airway</strong> obstruction, as <strong>in</strong><br />
<strong>the</strong> case of a patient with a large carc<strong>in</strong>oma at <strong>the</strong> base of<br />
<strong>the</strong> tongue who susta<strong>in</strong>ed a respiratory arrest (120).<br />
TTJV has been used effectively as a ventilation strategy<br />
<strong>in</strong> cannot-<strong>in</strong>tubate and cannot-ventilate (“failed <strong>airway</strong>”)<br />
situations (112,118,119). The technique has also proven<br />
useful <strong>in</strong> pediatric <strong>airway</strong> emergencies (122).<br />
When TTJV is utilized, ample time must be allowed<br />
for <strong>the</strong> passive recoil of <strong>the</strong> lungs to force exhalation of<br />
<strong>the</strong> <strong>in</strong>sufflated gas (2–3 sec), or “stack<strong>in</strong>g” of breaths,<br />
and barotrauma may result. Pneumothorax, pneumomediast<strong>in</strong>um,<br />
and subcutaneous (s.c.) air have all occurred<br />
as a result of TTJV (120,123). Contra<strong>in</strong>dicatons to TTJV<br />
<strong>in</strong>clude distorted anatomy that would make placement of<br />
<strong>the</strong> ca<strong>the</strong>ter difficult or impossible, bleed<strong>in</strong>g dia<strong>the</strong>sis,<br />
and complete <strong>airway</strong> obstruction (112). Adverse effects<br />
<strong>in</strong>clude barotrauma, as described above, bleed<strong>in</strong>g at <strong>the</strong><br />
site of <strong>in</strong>sertion, and loss of position of <strong>the</strong> ca<strong>the</strong>ter if it<br />
is not held firmly dur<strong>in</strong>g ventilation (115,118,119).<br />
Retrograde Intubation<br />
Retrograde <strong>in</strong>tubation (RI) was first reported <strong>in</strong> 1960<br />
(124). This <strong>in</strong>vasive technique allows for bl<strong>in</strong>d placement<br />
of an endotracheal tube over a guidewire or ca<strong>the</strong>ter<br />
that is <strong>in</strong>serted percutaneously at <strong>the</strong> level of <strong>the</strong><br />
cricothyroid membrane or cricotracheal ligament and<br />
directed “retrograde” through <strong>the</strong> pharynx to <strong>the</strong> mouth<br />
or nose. The procedure was orig<strong>in</strong>ally described with use<br />
of a red-rubber ca<strong>the</strong>ter <strong>in</strong>troduced through a tracheostomy,<br />
and has evolved to <strong>in</strong>clude <strong>the</strong> use of a guidewire<br />
placed percutaneously through <strong>the</strong> lumen or Murphy Eye<br />
of an endotracheal tube (Figure 5) (125,126). Because an
42 S. L. Orebaugh<br />
Figure 5. Retrograde <strong>in</strong>tubation, compar<strong>in</strong>g <strong>the</strong> technique of<br />
guidewire-through-lumen of ETT (A) to <strong>the</strong> technique of<br />
guidewire-through-Murphy eye of ETT (B). Use of <strong>the</strong> Murphy<br />
eye permits fur<strong>the</strong>r advancement of <strong>the</strong> endotracheal<br />
tube <strong>in</strong>to <strong>the</strong> <strong>airway</strong> before wire is removed (repr<strong>in</strong>ted with<br />
permission by Mosby-Year Book (35)).<br />
ETT has <strong>the</strong> potential to move laterally about <strong>the</strong> wire,<br />
and impact on <strong>the</strong> aryepiglottic fold or arytenoid cartilages,<br />
<strong>the</strong> technique frequently <strong>in</strong>corporates a guide ca<strong>the</strong>ter<br />
placed over <strong>the</strong> wire before <strong>the</strong> ETT is <strong>in</strong>serted<br />
(127). Available commercial kits frequently <strong>in</strong>clude this<br />
ca<strong>the</strong>ter as well.<br />
The technique of retrograde <strong>in</strong>tubation has been used<br />
effectively <strong>in</strong> <strong>the</strong> traumatized patient as <strong>the</strong> presence of<br />
blood or secretions <strong>in</strong> <strong>the</strong> pharynx does not detract from<br />
successful <strong>in</strong>tubation via this route (125,128). Retrograde<br />
<strong>in</strong>tubation also has been useful <strong>in</strong> difficult <strong>airway</strong><br />
<strong>management</strong> <strong>in</strong> both anes<strong>the</strong>siology and Emergency<br />
Medic<strong>in</strong>e (125,129,130). However, this technique has<br />
not been widely applied <strong>in</strong> Emergency Medic<strong>in</strong>e. Data<br />
regard<strong>in</strong>g its application are limited to case reports and<br />
case series. RI has been described anecdotally <strong>in</strong> a number<br />
of difficult <strong>airway</strong> situations, <strong>in</strong>clud<strong>in</strong>g <strong>management</strong><br />
of patients with large oral cancers, sp<strong>in</strong>al cord <strong>in</strong>jury,<br />
oral <strong>in</strong>fections, pharyngeal edema, laryngeal carc<strong>in</strong>omas,<br />
and <strong>airway</strong> anomalies (126). Barriot described its use by<br />
<strong>emergency</strong> physicians <strong>in</strong> <strong>the</strong> field, where it was employed<br />
successfully <strong>in</strong> 13 patients with severe maxillofacial<br />
trauma who could not be <strong>in</strong>tubated by direct laryngoscopy<br />
<strong>in</strong> <strong>the</strong> prehospital sett<strong>in</strong>g, and <strong>in</strong> ano<strong>the</strong>r six<br />
patients <strong>in</strong> whom <strong>the</strong> technique was used electively<br />
(128). In <strong>the</strong> hands of those who use <strong>the</strong> technique<br />
frequently, RI appears to have a high success rate. Of 383<br />
applications described <strong>in</strong> <strong>the</strong> literature by 1996, <strong>the</strong> technique<br />
was effective <strong>in</strong> 98.5% of cases (126).<br />
However, preparation and adm<strong>in</strong>istration of retrograde<br />
<strong>in</strong>tubation usually requires over 2 m<strong>in</strong> to complete,<br />
and sometimes considerably longer (126,128). This<br />
means of manag<strong>in</strong>g <strong>the</strong> difficult <strong>airway</strong> may <strong>the</strong>refore be<br />
useful when a patient presents with an obvious or suspected<br />
difficult <strong>airway</strong>, yet has relatively well-preserved<br />
oxygenation and ventilation (as <strong>in</strong> head or facial trauma).<br />
RI also could be employed when RSI fails, but mask<br />
ventilation is still possible, allow<strong>in</strong>g time to complete <strong>the</strong><br />
procedure.<br />
RI is a reasonably safe procedure. Adverse effects<br />
<strong>in</strong>clude bleed<strong>in</strong>g and, rarely, hematoma formation<br />
(99–101). Subcutaneous emphysema or pneumomediast<strong>in</strong>um<br />
may occur but <strong>the</strong>se complications are usually<br />
transient and self-limited (97,102,103). Bleed<strong>in</strong>g dia<strong>the</strong>sis<br />
is a relative contra<strong>in</strong>dication to <strong>the</strong> technique, as<br />
are distorted neck anatomy and laryngeal <strong>in</strong>jury<br />
(93,104,105).<br />
Variations on <strong>the</strong> technique of RI <strong>in</strong>clude <strong>the</strong> use of an<br />
epidural ca<strong>the</strong>ter <strong>in</strong>stead of a guide wire, and its use <strong>in</strong><br />
comb<strong>in</strong>ation with fiberoptic bronchoscopy (136,138,139).<br />
The guide wire may be placed through <strong>the</strong> suction channel<br />
of <strong>the</strong> fiberscope, lead<strong>in</strong>g <strong>the</strong> endoscopist directly to<br />
<strong>the</strong> laryngeal open<strong>in</strong>g despite secretions or unfavorable<br />
anatomy. The wire is <strong>the</strong>n removed and <strong>the</strong> <strong>in</strong>tubation<br />
carried out with direct visualization through <strong>the</strong> fiberscope.<br />
Fiberoptic Bronchoscopic Intubation<br />
Introduced <strong>in</strong> <strong>the</strong> 1960s, FOBs are available <strong>in</strong> a variety<br />
of sizes, depend<strong>in</strong>g upon <strong>the</strong>ir use, and are usually 55 or<br />
60 cm <strong>in</strong> length (140). Instruments used solely for <strong>in</strong>tubation<br />
tend to be smaller <strong>in</strong> diameter (1.8–4.0 mm) than<br />
those used for diagnosis and <strong>the</strong>rapy of pulmonary disease,<br />
which feature a larger work<strong>in</strong>g channel to admit<br />
biopsy forceps and o<strong>the</strong>r <strong>in</strong>struments. The fiberscope<br />
consists of a universal cord, which carries light <strong>in</strong> fiberoptic<br />
bundles from <strong>the</strong> light source; a handle conta<strong>in</strong><strong>in</strong>g<br />
an eyepiece, control lever for bend<strong>in</strong>g <strong>the</strong> distal tip of <strong>the</strong><br />
scope, suction button and access port to <strong>the</strong> work<strong>in</strong>g<br />
channel; and an <strong>in</strong>sertion cord that conta<strong>in</strong>s light bundles<br />
and <strong>the</strong> image transmission bundle, along with <strong>the</strong> tip<br />
control wires to allow bend<strong>in</strong>g of <strong>the</strong> tip forward or<br />
backward (141).<br />
Awake <strong>in</strong>tubation with a fiberscope requires ample<br />
time and preparation of <strong>the</strong> patient. Even <strong>in</strong> emergent<br />
circumstances, bronchoscopy requires 5–6 m<strong>in</strong> to perform,<br />
and, ideally, with such preparatory measures as
<strong>Difficult</strong> Airway Management 43<br />
patient sedation, topical and regional anes<strong>the</strong>sia of <strong>the</strong><br />
<strong>airway</strong>, and adm<strong>in</strong>istration of an antichol<strong>in</strong>ergic preparation<br />
to dry secretions, 15–20 m<strong>in</strong> is required (130,140).<br />
While controlled studies or comparisons of efficacy<br />
are few, case reports and series abound <strong>in</strong> <strong>the</strong> anes<strong>the</strong>sia<br />
literature of <strong>the</strong> utility of FOB <strong>in</strong> <strong>management</strong> of <strong>the</strong><br />
difficult <strong>airway</strong> (142–148). The effectiveness of FOB for<br />
<strong>in</strong>tubation of <strong>the</strong> patient with a cervical sp<strong>in</strong>e <strong>in</strong>jury is<br />
well established (143,146,148). The <strong>in</strong>tubat<strong>in</strong>g bronchoscope<br />
plays a very important role <strong>in</strong> awake <strong>in</strong>tubation of<br />
<strong>the</strong> patient with a suspected or known difficult <strong>airway</strong><br />
(130). Under <strong>the</strong>se circumstances, <strong>the</strong> success rate of <strong>the</strong><br />
procedure is almost 99%. The simultaneous use of direct<br />
laryngoscopy with FOB may improve <strong>the</strong> success rate of<br />
<strong>the</strong> technique by displac<strong>in</strong>g soft tissues that can impede<br />
<strong>the</strong> fiberscopic view of <strong>the</strong> glottis (149).<br />
The nasotracheal approach to <strong>the</strong> <strong>airway</strong> with FOB is<br />
often simpler than <strong>the</strong> oral approach because <strong>the</strong> <strong>in</strong>strument<br />
is aimed directly at <strong>the</strong> glottis as it emerges from<br />
<strong>the</strong> nasopharynx <strong>in</strong>to <strong>the</strong> hypopharynx (140). Intubation<br />
over <strong>the</strong> bronchoscope can be successfully performed<br />
through an LMA and around <strong>the</strong> ETC (130,150). There<br />
are many advantages to <strong>the</strong> technique, <strong>in</strong>clud<strong>in</strong>g applicability<br />
to all age groups, excellent <strong>airway</strong> visualization,<br />
ability to <strong>in</strong>sufflate oxygen dur<strong>in</strong>g <strong>the</strong> procedure, high<br />
success rate, and immediate confirmation of ETT placement<br />
(146).<br />
There are significant limitations to bronchoscopic <strong>in</strong>tubation.<br />
In <strong>the</strong> presence of uncontrolled secretions, mucus,<br />
or bleed<strong>in</strong>g <strong>in</strong> <strong>the</strong> <strong>airway</strong>, visibility is difficult or<br />
impossible. Suction through <strong>the</strong>se <strong>in</strong>struments is relatively<br />
<strong>in</strong>effective, but by attach<strong>in</strong>g an oxygen source to<br />
<strong>the</strong> suction channel of <strong>the</strong> <strong>in</strong>strument, oxygen <strong>in</strong>sufflation<br />
may be used to blow offend<strong>in</strong>g matter away from <strong>the</strong><br />
lens to improve visibility. Fur<strong>the</strong>rmore, <strong>the</strong> natural compression<br />
of soft tissues of <strong>the</strong> oropharynx and hypopharynx<br />
<strong>in</strong> <strong>the</strong> sup<strong>in</strong>e, anes<strong>the</strong>tized patient can make <strong>the</strong><br />
approach to <strong>the</strong> <strong>airway</strong> difficult due to physical obstruction<br />
and poor visibility. This is a greater problem <strong>in</strong> oral<br />
<strong>in</strong>tubation than nasal <strong>in</strong>tubation. Effective means to address<br />
this concern <strong>in</strong>clude use of a specialized oral <strong>airway</strong><br />
such as <strong>the</strong> Ovassapian <strong>airway</strong> or Williams <strong>airway</strong>,<br />
a jaw thrust by an assistant, or direct laryngoscopy provided<br />
by an assistant (130,140,141). F<strong>in</strong>ally, advancement<br />
of <strong>the</strong> endotracheal tube over <strong>the</strong> FOB is difficult <strong>in</strong><br />
up to 25% of cases, as <strong>the</strong> bevel of <strong>the</strong> tube may catch on<br />
<strong>the</strong> arytenoid cartilages or aryepiglottic folds. Withdraw<strong>in</strong>g<br />
<strong>the</strong> endotracheal tube, and rotat<strong>in</strong>g it 90° <strong>in</strong> ei<strong>the</strong>r<br />
direction usually solves this problem, but about 10% of<br />
<strong>the</strong> time one cannot advance <strong>the</strong> tube, requir<strong>in</strong>g a change<br />
to a smaller tube or a different approach to <strong>the</strong> <strong>airway</strong><br />
(140). Barriers to facility <strong>in</strong>clude an <strong>in</strong>itial tra<strong>in</strong><strong>in</strong>g period,<br />
a relatively slow learn<strong>in</strong>g curve, and failure to<br />
reta<strong>in</strong> skills when <strong>the</strong> procedure is <strong>in</strong>frequently utilized<br />
(140).<br />
In <strong>the</strong> ED, little systematic study has accrued on <strong>the</strong><br />
utility and efficacy of FOB <strong>in</strong> <strong>airway</strong> <strong>management</strong>.<br />
Delaney reported a series of 57 <strong>in</strong>tubations carried out by<br />
two <strong>emergency</strong> physicians tra<strong>in</strong>ed on a mannequ<strong>in</strong> <strong>in</strong> <strong>the</strong><br />
use of a 50-cm fiberoptic scope (151). The cases were<br />
selected for <strong>the</strong> skill level of <strong>the</strong> physicians (more than<br />
half were overdose patients). The authors reported a 13%<br />
failure rate, and 22% of <strong>the</strong> patients had significant<br />
bleed<strong>in</strong>g with <strong>the</strong> nasotracheal approach. In ano<strong>the</strong>r<br />
study of fiberoptic <strong>in</strong>tubation <strong>in</strong> <strong>the</strong> ED, <strong>the</strong> authors<br />
reported that only 75% of 39 patients were successfully<br />
<strong>in</strong>tubated by use of <strong>the</strong> fiberscope, whereas 95% of a<br />
comparable group of patients were managed successfully<br />
with direct laryngoscopy (152). Levitan, <strong>in</strong> a study of ED<br />
practices at U.S. teach<strong>in</strong>g hospitals, found that <strong>the</strong> FOB<br />
was seldom employed as a means of <strong>management</strong> of <strong>the</strong><br />
difficult <strong>airway</strong> (2).<br />
Rigid Fiberoptic Laryngoscopes<br />
Several rigid fiberoptic laryngoscopes are available. The<br />
oldest, and most familiar, is <strong>the</strong> Bullard laryngoscope<br />
(Circon, ACMI, Stamford, CT, USA). The operator <strong>in</strong>serts<br />
<strong>the</strong> scope <strong>in</strong>to <strong>the</strong> hypopharynx, and under <strong>in</strong>direct<br />
vision through <strong>the</strong> eyepiece, advances <strong>the</strong> blade <strong>in</strong>to<br />
position cephalad to <strong>the</strong> glottis. The endotracheal tube<br />
can <strong>the</strong>n be pushed forward off <strong>the</strong> stylet, <strong>in</strong>to <strong>the</strong> glottis<br />
dur<strong>in</strong>g visualization. The Bullard laryngoscope is <strong>in</strong>dicated<br />
for <strong>airway</strong> <strong>management</strong> when <strong>the</strong> glottis is difficult<br />
to visualize due to unfavorable anatomy, and when preservation<br />
of cervical sp<strong>in</strong>e immobilization is essential. It<br />
also may be used for rout<strong>in</strong>e laryngoscopy and <strong>in</strong>tubation.<br />
O<strong>the</strong>r rigid fiberoptic scopes <strong>in</strong>clude <strong>the</strong> Upsherscope<br />
(<strong>the</strong> Upsher Laryngoscope Corporation, Foster<br />
City, CA, USA) and <strong>the</strong> WuScope (Actis Corporation,<br />
Dubl<strong>in</strong>, CA, USA).<br />
None of <strong>the</strong>se devices has undergone rigorous trials <strong>in</strong><br />
<strong>the</strong> ED to compare <strong>the</strong>m with conventional means of<br />
manag<strong>in</strong>g <strong>the</strong> <strong>airway</strong>. Watts described a comparison of<br />
<strong>the</strong> time required for <strong>in</strong>tubation and <strong>the</strong> degree of cervical<br />
extension utiliz<strong>in</strong>g <strong>the</strong> Bullard scope and direct laryngoscopy,<br />
both with and without <strong>in</strong>-l<strong>in</strong>e cervical immobilization,<br />
<strong>in</strong> patients under general anes<strong>the</strong>sia (154).<br />
The degree of sp<strong>in</strong>e extension and <strong>the</strong> time to <strong>in</strong>tubation<br />
were similar, except when cervical immobilization was<br />
imposed, at which time <strong>the</strong> average duration required for<br />
<strong>in</strong>tubation with <strong>the</strong> Bullard laryngoscope was significantly<br />
prolonged, from 25–40 sec. However, Schulman<br />
reported <strong>in</strong> a randomized trial <strong>in</strong> 50 patients under anes<strong>the</strong>sia<br />
that, <strong>in</strong> compar<strong>in</strong>g <strong>the</strong> Bullard scope to a flexible<br />
fiberscope dur<strong>in</strong>g <strong>in</strong>-l<strong>in</strong>e cervical immobilization, <strong>in</strong>tu-
44 S. L. Orebaugh<br />
bation was significantly easier to accomplish, and required<br />
less time with <strong>the</strong> rigid apparatus (155).<br />
The Upsherscope, a relatively new rigid scope <strong>in</strong>corporat<strong>in</strong>g<br />
a C-shaped steel blade with enclosed fiberoptic<br />
bundles and an <strong>in</strong>tubation channel, proved to have no<br />
advantage over direct laryngoscopy <strong>in</strong> enabl<strong>in</strong>g <strong>in</strong>tubation<br />
<strong>in</strong> a group of 300 patients randomly assigned to<br />
<strong>airway</strong> <strong>management</strong> <strong>in</strong> <strong>the</strong> OR by ei<strong>the</strong>r technique (156).<br />
In fact, <strong>the</strong> authors reported a 15% failure rate with <strong>the</strong><br />
Upsherscope, compared to only 3% with direct laryngoscopy.<br />
Yet ano<strong>the</strong>r rigid fiberoptic scope, <strong>the</strong> WuScope,<br />
was compared to direct laryngoscopy <strong>in</strong> 87 patients randomized<br />
to ei<strong>the</strong>r form of <strong>airway</strong> <strong>management</strong> dur<strong>in</strong>g<br />
<strong>in</strong>-l<strong>in</strong>e cervical immobilization to simulate potential cervical<br />
<strong>in</strong>jury dur<strong>in</strong>g anes<strong>the</strong>sia for elective surgery (157).<br />
The authors found similar rates of <strong>in</strong>tubation success, but<br />
longer times to <strong>in</strong>tubation and lower glottic visualization<br />
scores us<strong>in</strong>g <strong>the</strong> WuScope.<br />
Surgical Airway<br />
The time-honored means of obta<strong>in</strong><strong>in</strong>g a rapid def<strong>in</strong>itive<br />
<strong>airway</strong> when both <strong>in</strong>tubation and ventilation fail is <strong>the</strong><br />
<strong>in</strong>sertion of a tracheal tube through an <strong>in</strong>cision <strong>in</strong> <strong>the</strong><br />
neck. Although discouraged <strong>in</strong> <strong>the</strong> early part of <strong>the</strong> 20 th<br />
century because of complications occurr<strong>in</strong>g after <strong>the</strong><br />
procedure, chiefly subglottic stenosis, cricothyrotomy<br />
was reestablished as a safe technique for <strong>airway</strong> <strong>management</strong><br />
after <strong>the</strong> paper by Brantigan appeared, document<strong>in</strong>g<br />
a much lower complication rate than expected<br />
(158). The technique <strong>in</strong>volves a vertical <strong>in</strong>cision <strong>in</strong> <strong>the</strong><br />
midl<strong>in</strong>e over <strong>the</strong> palpable laryngeal cartilages, followed<br />
by a transverse <strong>in</strong>cision <strong>in</strong> <strong>the</strong> cricothyroid membrane, or<br />
a s<strong>in</strong>gle transverse <strong>in</strong>cision through <strong>the</strong> sk<strong>in</strong>, s.c. tissue,<br />
and cricothyroid membrane if <strong>the</strong> <strong>in</strong>terval is palpable<br />
(158,159). Recent studies have focused on <strong>the</strong> “rapid<br />
four-step technique” for cricothyrotomy (160). Holmes<br />
described its use <strong>in</strong> cadavers by <strong>in</strong>experienced personnel,<br />
and compared this method to <strong>the</strong> standard technique<br />
(161). The authors reported equal success with each<br />
method (88% vs. 94%, respectively), with identical complication<br />
rates of 38%, but more rapid tracheal tube<br />
<strong>in</strong>sertion with <strong>the</strong> rapid four-step technique, which required<br />
an average of only 43 sec compared to an average<br />
of 134 sec for <strong>the</strong> conventional method. In ano<strong>the</strong>r cadaver<br />
model, Davis described a significantly higher <strong>in</strong>cidence<br />
of complications with <strong>the</strong> rapid four-step technique,<br />
primarily cricoid cartilage fracture (162).<br />
Cricothyrotomy also may be accomplished with a<br />
wire-guided technique, similar to <strong>the</strong> Seld<strong>in</strong>ger technique<br />
for cannulat<strong>in</strong>g blood vessels. After puncture of <strong>the</strong><br />
cricothyroid membrane with a th<strong>in</strong>-walled needle and<br />
aspiration of air to confirm position, a wire is advanced<br />
through <strong>the</strong> needle, which is <strong>the</strong>n removed. After a small<br />
<strong>in</strong>cision <strong>in</strong> <strong>the</strong> sk<strong>in</strong> and <strong>in</strong>sertion of a dilator, <strong>the</strong> <strong>airway</strong><br />
is <strong>in</strong>serted over <strong>the</strong> dilator and wire. In a randomized,<br />
cross-over trial performed on cadavers, Chan et al. compared<br />
<strong>the</strong> standard technique of cricothyrotomy to <strong>the</strong><br />
Melker wire-guided method (164). The authors found<br />
that 14 of 15 physicians participat<strong>in</strong>g preferred <strong>the</strong> wireguided<br />
technique, while overall success was similar for<br />
both methods. Eisenberger reported that <strong>in</strong>experienced<br />
cl<strong>in</strong>icians attempt<strong>in</strong>g to perform cricothyrotomy on cadavers<br />
had a low success rate of only 60–70%, with<br />
ei<strong>the</strong>r <strong>the</strong> standard or wire-guided technique (165).<br />
Whatever method is chosen to perform cricothyrotomy<br />
by <strong>the</strong> <strong>emergency</strong> physician, this procedure rema<strong>in</strong>s<br />
<strong>the</strong> most reliable and time-honored def<strong>in</strong>itive <strong>airway</strong><br />
procedure <strong>in</strong> a “failed <strong>airway</strong>” scenario (37). The<br />
morbidity and mortality of this technique, when carried<br />
out for long-term <strong>airway</strong> <strong>management</strong>, appears to be<br />
similar to that of tracheostomy (158,166).<br />
In <strong>the</strong> prehospital realm, surgical <strong>airway</strong>s generally<br />
have been employed for massively <strong>in</strong>jured patients with<br />
significant facial trauma. Spaite described attempted cricothyrotomy<br />
<strong>in</strong> 16 patients with an 88% success rate, and<br />
a complication rate of 31% (167). Boyle, <strong>in</strong> a retrospective<br />
study of cricothyrotomy by flight nurses <strong>in</strong> a teach<strong>in</strong>g<br />
hospital helicopter program, described 69 attempts of<br />
this procedure among 2108 patients transported. The<br />
procedure was accomplished successfully <strong>in</strong> 98.5% of<br />
cases with only one failure, and a low complication rate<br />
of 8.7% (168).<br />
Prevent<strong>in</strong>g <strong>the</strong> “Failed Airway”<br />
Perhaps <strong>the</strong> best means of cop<strong>in</strong>g with <strong>the</strong> problem of<br />
difficult <strong>in</strong>tubation or failed <strong>airway</strong> is to prevent <strong>the</strong>ir<br />
occurrence altoge<strong>the</strong>r. This requires that <strong>the</strong> <strong>in</strong>itial attempt<br />
at direct laryngoscopy is optimized, <strong>in</strong> order to<br />
avoid repeated attempts at <strong>in</strong>tubation that may cause<br />
bleed<strong>in</strong>g and swell<strong>in</strong>g <strong>in</strong> <strong>the</strong> pharynx and supraglottic<br />
area, and <strong>the</strong>n a vicious cycle <strong>in</strong> which each attempt<br />
leads to a greater likelihood of failed <strong>in</strong>tubation and<br />
ventilation with potentially disastrous consequences<br />
(41). Optimiz<strong>in</strong>g laryngoscopy requires appropriate position<strong>in</strong>g<br />
of <strong>the</strong> patient to align <strong>the</strong> pharyngeal, oral, and<br />
laryngeal axes for visualization of <strong>the</strong> glottis; effective<br />
muscle relaxation with an appropriate dose of succ<strong>in</strong>ylchol<strong>in</strong>e<br />
or a nondepolariz<strong>in</strong>g agent; <strong>the</strong> use of a laryngoscope<br />
blade type and size which best fits <strong>the</strong> situation;<br />
and <strong>the</strong> use of optimal external laryngeal pressure by <strong>the</strong><br />
laryngoscopist (41,169). In this maneuver, laryngeal<br />
pressure is exerted by <strong>the</strong> right hand dur<strong>in</strong>g laryngoscopy,<br />
to maneuver <strong>the</strong> larynx <strong>in</strong>to a position <strong>in</strong> which <strong>the</strong><br />
glottis can be best seen. An assistant <strong>the</strong>n ma<strong>in</strong>ta<strong>in</strong>s this
<strong>Difficult</strong> Airway Management 45<br />
Figure 6. Optimal external laryngeal pressure requires laryngoscopist<br />
to utilize right hand to manipulate <strong>the</strong> larynx while<br />
view<strong>in</strong>g <strong>the</strong> glottis with <strong>the</strong> laryngoscope, before grasp<strong>in</strong>g<br />
<strong>the</strong> ETT, and <strong>the</strong>n request<strong>in</strong>g an assistant to ma<strong>in</strong>ta<strong>in</strong> this<br />
directed pressure while <strong>the</strong> tube is placed <strong>in</strong> <strong>the</strong> <strong>airway</strong> by<br />
<strong>the</strong> now-liberated right hand (repr<strong>in</strong>ted with permission by<br />
Mosby Year-Book (36)).<br />
directed pressure while <strong>the</strong> laryngoscopist accepts and<br />
places <strong>the</strong> ETT with <strong>the</strong> right hand. The maneuver,<br />
which <strong>in</strong>itially seems awkward, is rapidly learned, and<br />
has been shown to substantially improve <strong>the</strong> laryngoscopic<br />
view <strong>in</strong> most patients (Figure 6) (170). Alternately,<br />
<strong>the</strong> assistant may apply pressure “backwards,<br />
upwards and rightwards” (BURP maneuver) (169).<br />
When all of <strong>the</strong>se factors are taken <strong>in</strong>to account, <strong>the</strong> first<br />
attempt at laryngoscopy is likely to be <strong>the</strong> best attempt,<br />
without loss of precious seconds to correct suboptimal<br />
aspects of <strong>the</strong> procedure after a poor view of <strong>the</strong> glottis<br />
becomes evident.<br />
CONCLUSIONS<br />
Emergency physicians manage <strong>the</strong> <strong>airway</strong> with great<br />
efficacy for <strong>the</strong> vast majority of cases that present to <strong>the</strong><br />
ED requir<strong>in</strong>g such <strong>in</strong>tervention. However, a small subset<br />
of patients will cause difficulty <strong>in</strong> laryngoscopy, <strong>in</strong>tubation,<br />
and BVM ventilation, because of ei<strong>the</strong>r unfavorable<br />
anatomy or facial, <strong>airway</strong> or cervical pathology. This is<br />
more likely <strong>in</strong> <strong>the</strong> ED than elsewhere <strong>in</strong> <strong>the</strong> hospital<br />
because of <strong>the</strong> emergent nature of most <strong>airway</strong> <strong>management</strong><br />
and <strong>the</strong> <strong>in</strong>ability to assess <strong>the</strong> patient ahead of time.<br />
A large variety of adjuncts are available for assistance<br />
with both <strong>in</strong>tubation and ventilation. Identify<strong>in</strong>g a set of<br />
tools and techniques with which <strong>the</strong> practitioner is familiar<br />
and comfortable can serve to alleviate anxiety and<br />
improve efficiency when direct laryngoscopy is <strong>in</strong>sufficient<br />
to manage <strong>the</strong> <strong>airway</strong>. Optimiz<strong>in</strong>g direct laryngoscopy<br />
with attention to patient position<strong>in</strong>g, muscle relaxation,<br />
type of laryngoscope blade, and external laryngeal<br />
pressure serves to reduce <strong>the</strong> <strong>in</strong>cidence of poor laryngoscopic<br />
visualization. For those situations <strong>in</strong> which adjuncts<br />
are not useful or <strong>in</strong> which ventilation by BVM is<br />
impossible, direct access to <strong>the</strong> larynx via a surgical<br />
<strong>airway</strong> or transtracheal jet ventilation is necessary.<br />
REFERENCES<br />
1. Ma OJ, Bentley B, DeBehnke DJ. Airway <strong>management</strong> practices<br />
<strong>in</strong> <strong>emergency</strong> medic<strong>in</strong>e residencies. Am J Emerg Med 1995;13:<br />
501–4.<br />
2. Levitan RM, Kush S, Hollender JE. Devices for difficult <strong>airway</strong><br />
<strong>management</strong> <strong>in</strong> academic <strong>emergency</strong> <strong>department</strong>s. Ann Emerg<br />
Med 1999;33:694–8.<br />
3. Chang RS, Hamilton RJ, Carter WA. Decl<strong>in</strong><strong>in</strong>g rate of cricothyrotomy<br />
<strong>in</strong> trauma patients with an <strong>emergency</strong> medic<strong>in</strong>e residency.<br />
Acad Emerg Med 1998;5:247–51.<br />
4. Caplan RA, Benumof JL, Berry FA, et al. Practice Guidel<strong>in</strong>es for<br />
<strong>management</strong> of <strong>the</strong> difficult <strong>airway</strong>: a report by <strong>the</strong> ASA Task<br />
Force on Management of <strong>the</strong> difficult <strong>airway</strong>. Anesth 1993;78:<br />
597–602.<br />
5. Cormack RS, Lehane J. <strong>Difficult</strong> tracheal <strong>in</strong>tubation <strong>in</strong> obstetrics.<br />
Anesth 1984;39:1105–11.<br />
6. Levitan R, Ochtroch EA, Kush S. Validation of <strong>the</strong> Percentage of<br />
Glottic Open<strong>in</strong>g (POGO) Score. Acad Emerg Med 1998;5:482.<br />
7. Adnet F, Borron SW, Rac<strong>in</strong>e SX, et al. The Intubation <strong>Difficult</strong>y<br />
Scale (IDS). Anesth 1997;87:1273–4.<br />
8. Mallampati SR. Cl<strong>in</strong>ical signs to predict difficult tracheal <strong>in</strong>tubation<br />
(hypo<strong>the</strong>sis). Can Anaesth Soc J 1983;30:316–8.<br />
9. Samsoon GLT, Young JRB. <strong>Difficult</strong> tracheal <strong>in</strong>tubation. Anaesth<br />
1987;42:487–90.<br />
10. Mallampati SR, Gatt SP, Gug<strong>in</strong>o LD, et al. A cl<strong>in</strong>ical sign to<br />
predict difficult tracheal <strong>in</strong>tubation: a prospective study. Can<br />
Anaesth Soc J 1985;32:429–34.<br />
11. Wilson ME, Spiegelhalter D, Robertson JA, et al. Predict<strong>in</strong>g<br />
difficult <strong>in</strong>tubation. Br J Anaesth 1988;61:211–6.<br />
12. Chou HC, Wu TL. Mandibulohyoid distance <strong>in</strong> difficult laryngoscopy.<br />
Br J Anaesth 1993;71:335–9.<br />
13. Bellhouse CP, Dore C. Criteria for estimat<strong>in</strong>g likelihood of endotracheal<br />
<strong>in</strong>tubation with MacIntosh laryngoscope. Anaesth Int<br />
Care 1988;16:329–37.<br />
14. Frerk CM, Till CB, Bradley AJ. <strong>Difficult</strong> <strong>in</strong>tubation: temporomandibular<br />
distance and atlantooccipital gap. Anaes<strong>the</strong>sia 1996;<br />
51:738–40.<br />
15. Watson CB. Prediction of difficult <strong>in</strong>tubation. Resp Care 1999;<br />
44:777–98.<br />
16. Randell T. Prediction of difficult <strong>in</strong>tubation. Acta Anaesth Scand<br />
1996;40:1016–23.<br />
17. Langeron O, Masso E, Huraux C, et al. Prediction of difficult<br />
mask ventilation. Anesth 2000;92:1229–36.<br />
18. Williams KN, Carli F, Cormack RS. Unexpected difficult laryngoscopy.<br />
Br J Anesth 1991;66:38–44.<br />
19. Cohen SM, Laurito C, Segil LJ. Oral exam to predict difficult<br />
<strong>in</strong>tubation. Anesth 1989;71:A937.<br />
20. Glassenberg R, Vaisrub N, Albright G. Incidence of failed <strong>in</strong>tubation<br />
<strong>in</strong> obstetrics. Anesth 1991;73:A1061.<br />
21. Benumof JL, Scheller MS. Importance of transtracheal jet ventilation<br />
<strong>in</strong> <strong>the</strong> <strong>management</strong> of <strong>the</strong> difficult <strong>airway</strong>. Anesth 1982;<br />
71:769–78.
46 S. L. Orebaugh<br />
22. Tunstall ME. Failed <strong>in</strong>tubation <strong>in</strong> <strong>the</strong> parturient. Can J Anaesth<br />
1989;36:611–2.<br />
23. Keenan RL, Bousan CP. Decreas<strong>in</strong>g frequency of anes<strong>the</strong>tic<br />
cardiac arrest. J Cl<strong>in</strong> Anesth 1991;3:354–7.<br />
24. Eichorn JH. Document<strong>in</strong>g improved anes<strong>the</strong>tic outcome. J Cl<strong>in</strong><br />
Anesth 1991;3:351–4.<br />
25. Sakles JC, Laur<strong>in</strong> EG, Rantapaa AA, et al. Airway <strong>management</strong><br />
<strong>in</strong> <strong>the</strong> <strong>emergency</strong> <strong>department</strong>: a one year study of 610 tracheal<br />
<strong>in</strong>tubations. Ann Emerg Med 1998;31:325–32.<br />
26. Tayal VS, Riggs RW, Marx JA, et al. Rapid-sequence <strong>in</strong>tubation<br />
at an <strong>emergency</strong> medic<strong>in</strong>e residency. Acad Emerg Med 1999;6:<br />
31–7.<br />
27. Walls RM, Gurr DE, Kulkarni RG, et al. 6294 Emergency <strong>department</strong><br />
<strong>in</strong>tubations: second report of <strong>the</strong> Ongo<strong>in</strong>g National<br />
Emergency Airway Registry (NEAR) II study. Ann Emerg Med<br />
2000;36:S51.<br />
28. Li J. Capnography alone is imperfect for endotracheal tube placment<br />
confirmation dur<strong>in</strong>g <strong>emergency</strong> <strong>in</strong>tubation. J Emerg Med<br />
2001;20:223–9.<br />
29. DuFour DG, Larose DL, Clement SC. Rapid sequence <strong>in</strong>tubation<br />
<strong>in</strong> <strong>the</strong> <strong>emergency</strong> <strong>department</strong>. J Emerg Med 1995;13:705–10.<br />
30. Walls RM. Management of difficult <strong>airway</strong> <strong>in</strong> <strong>the</strong> trauma patient.<br />
Emerg Med Cl<strong>in</strong> N Am 1998;16:45–61.<br />
31. Nolan JP, Wilson ME. Orotracheal <strong>in</strong>tubation <strong>in</strong> patients with<br />
potential c-sp<strong>in</strong>e <strong>in</strong>juries. Anesth 1993;48:630–3.<br />
32. Caplan RA, Posner KL, Ward RJ, et al. Adverse respiratory<br />
events <strong>in</strong> anes<strong>the</strong>sia: a closed claims analysis. Anesth 1990;72:<br />
828–33.<br />
33. Benumof JL. Management of <strong>the</strong> difficult <strong>airway</strong>. Anesth 1991;<br />
75:1087–110.<br />
34. Benumof JL, Dagg R, Benumof R. Critical hemoglob<strong>in</strong> desaturation<br />
will occur before return to an unparalyzed state follow<strong>in</strong>g<br />
1 mg/kg of <strong>in</strong>travenous succ<strong>in</strong>ylchol<strong>in</strong>e. Anesth 1997;87:979–<br />
82.<br />
35. Cheney FW. Committee on professional liability. Am Soc Anesth<br />
Newslett 1994;58:7–10.<br />
36. Melker RJ, Florete OG. Percutaneous dilational cricothyrotomy<br />
and tracheostomy. In: Benumof JL, ed. Airway <strong>management</strong>. St.<br />
Louis: Mosby; 1996:484–512.<br />
37. Walls RM. The <strong>emergency</strong> <strong>airway</strong> algorithms. In: Walls RM, ed.<br />
Manual of <strong>airway</strong> <strong>management</strong>. Philadelphia: Lipp<strong>in</strong>cott, William<br />
and Wilk<strong>in</strong>s, 2000:16–25.<br />
38. Mulder DS, Marelli D. Evolution of <strong>airway</strong> control <strong>in</strong> <strong>the</strong> <strong>management</strong><br />
of <strong>in</strong>jured patients. J Trauma 1992;33:856–62.<br />
39. Miller RA. A new laryngoscope. Anesth 1941;2:317–20.<br />
40. MacIntosh RR. A new laryngoscope. Lancet 1943;1:205.<br />
41. Benumof JL. <strong>Difficult</strong> laryngoscopy: obta<strong>in</strong><strong>in</strong>g <strong>the</strong> best view. Can<br />
J Anaesth 1994;41:361–5.<br />
42. Phillips OC, Duerksen RL. Endotracheal <strong>in</strong>tubation: a new blade<br />
for direct laryngoscopy. Anesth Analg 1973;52:691–7.<br />
43. Siker ES. A mirror laryngoscope. Anesth 1956;17:38–42.<br />
44. Bizzarri DV, Giuffrida JG. Improved laryngoscope design for<br />
ease of manipulation and reduction of trauma. Anesth Analg<br />
1958;37:231–2.<br />
45. Bellhouse CP. An angulated laryngoscope for rout<strong>in</strong>e and difficult<br />
tracheal <strong>in</strong>tubation. Anesth 1988;69:126–9.<br />
46. Choi JJ. An angulated laryngoscope for rout<strong>in</strong>e and difficult<br />
tracheal <strong>in</strong>tubation. Anesth 1990;72:576.<br />
47. McCoy ED, Mirakhur RK. The Lever<strong>in</strong>g laryngoscope. Anaesth<br />
1993;48:516–8.<br />
48. Racz GB. Improved vision modification of <strong>the</strong> MacIntosh laryngoscope.<br />
Anaesth 1984;39:1249–50.<br />
49. Mayall RM. The belscope for <strong>management</strong> of <strong>the</strong> difficult <strong>airway</strong>.<br />
Anesth 1992;76:1059–60.<br />
50. Cook TM, Tuckey JP. A comparison between <strong>the</strong> MacIntosh and<br />
<strong>the</strong> McCoy laryngoscope blades. Anaesth 1996;51:977–80.<br />
51. Tuckey JP, Cook TM. An evaluation of <strong>the</strong> Lever<strong>in</strong>g laryngoscope.<br />
Anaesth 1996;51:71–3.<br />
52. Huffman JP. The application of prisms to curved laryngoscopes.<br />
J Am Assoc Nurse Anesth 1968;36:138–9.<br />
53. Neuste<strong>in</strong> SM. The Neuste<strong>in</strong> laryngoscope: a new solution to <strong>the</strong><br />
difficult <strong>in</strong>tubation. Anesth Rev 1992;19:54–9.<br />
54. McCarroll SM, Lamont BJ, Buckland MR, et al. The gum elastic<br />
bougie: old but still useful. Anesth 1988;68:643–4.<br />
55. Nocera A. A flexible solution for <strong>emergency</strong> <strong>in</strong>tubation difficulties.<br />
Ann Emerg Med 1996;27:665–7.<br />
56. Dogra S, Falconer R, Latto IP. Successful difficult <strong>in</strong>tubation.<br />
Anaesth 1990;45:774–6.<br />
57. Morton T, Brady S, Clancy M. <strong>Difficult</strong> <strong>airway</strong> equipment <strong>in</strong><br />
English <strong>emergency</strong> <strong>department</strong>s. Anaesth 2000;55:485–8.<br />
58. Moscati R, Jehle D, Christiansen G, et al. Endotracheal tube<br />
<strong>in</strong>troducer for failed <strong>in</strong>tubations: a variant of <strong>the</strong> gum elastic<br />
bougie. Ann Emerg Med 2000;36:52–6.<br />
59. Rosenberg MB, Levesque PR, Bourke DL. Use of <strong>the</strong> laryngotracheal<br />
anese<strong>the</strong>sia kit as a guide for endotracheal <strong>in</strong>tubation.<br />
Anesth Analg 1977;56:287–8.<br />
60. Dronen SC, Merigian DS, Hedges JR, et al. A comparison of<br />
bl<strong>in</strong>d nasotracheal and succ<strong>in</strong>ylchol<strong>in</strong>e assisted <strong>in</strong>tubation <strong>in</strong> <strong>the</strong><br />
poisoned patient. Ann Emerg Med 1987;16:650–2.<br />
61. O’Connor RE, Megargel RE, Schnyder ME, et al. Paramedic<br />
success rate for bl<strong>in</strong>d nasotracheal <strong>in</strong>tubation is improved with <strong>the</strong><br />
use of an endotracheal tube with directional tip control. Ann<br />
Emerg Med 2000;36:328–32.<br />
62. Yamamura H. Device for bl<strong>in</strong>d nasal <strong>in</strong>tubation. Anesth 1959;20:<br />
221.<br />
63. Davis L, Cook–Sa<strong>the</strong>r SD, Schre<strong>in</strong>er MS. Lighted stylet tracheal<br />
<strong>in</strong>tubation. Anesth Analg 2000;90:745–56.<br />
64. Vollmer TP, Stewart RD, Paris PM, et al. Use of a lighted stylet<br />
for guided orotracheal <strong>in</strong>tubation <strong>in</strong> <strong>the</strong> prehospital sett<strong>in</strong>g. Ann<br />
Emerg Med 1985;14:324–8.<br />
65. A<strong>in</strong>sworth QP, Howells TH. Transillum<strong>in</strong>ated tracheal <strong>in</strong>tubation.<br />
Br J Anaesth 1989;62:494–7.<br />
66. Hung OR, Pytka S, Morris I, et al. Cl<strong>in</strong>ical trial of a new<br />
lightwand device to <strong>in</strong>tubate <strong>the</strong> trachea. Anesth 1995;83:509–<br />
14.<br />
67. Weis FR. Intubation by use of a lightwand. J Oral Maxil Surg<br />
1989;47:577–81.<br />
68. Hung OR, Stevens SC, Pytka S, et al. Cl<strong>in</strong>ical trial of a new<br />
lightwand device for <strong>in</strong>tubat<strong>in</strong> <strong>in</strong> patients with difficult <strong>airway</strong>s.<br />
Anesth 1998;79:A498.<br />
69. Weis FR. Lightwand <strong>in</strong>tubation for cervical sp<strong>in</strong>e <strong>in</strong>juries. Anesth<br />
Analg 1992;74:619–23.<br />
70. Verdile VP, Heller MB, Paris PM, et al. Nasotracheal <strong>in</strong>tubation<br />
<strong>in</strong> traumatic craniofacial dislocation. Am J Emerg Med 1988;6:<br />
39–41.<br />
71. Hauswald M, Sklar DP, Tandberg D, et al. Cervical sp<strong>in</strong>e movement<br />
dur<strong>in</strong>g <strong>airway</strong> <strong>management</strong>. Am J Emerg Med 1991;9:<br />
535–8.<br />
72. Verdile VP, Chiang JL, Bedger R, et al. Nasotracheal <strong>in</strong>tubation<br />
us<strong>in</strong>g a flexible lighted stylet. Ann Emerg Med 1990;19:506–10.<br />
73. Weiss M. Video <strong>in</strong>tuboscopy: a new aid to rout<strong>in</strong>e and difficult<br />
tracheal <strong>in</strong>tubation. Br J Anaesth 1998;80:525–7.<br />
74. Kitamura T, Yamada Y, Du H-L, et al. Efficiency of a new<br />
fiberoptic stylet scope <strong>in</strong> tracheal <strong>in</strong>tubation. Anesth 1999;91:<br />
1628–32.<br />
75. Gravenste<strong>in</strong> D, Melker R, Lampotang S. Cl<strong>in</strong>ical assessment of a<br />
plastic optical fiber stylet for human tracheal <strong>in</strong>tubation. Anesth<br />
1999;91:648–53.<br />
76. Biro P, Weiss M, Gerber A, et al. Comparison of a new videooptical<br />
<strong>in</strong>tubation stylet versus <strong>the</strong> convent<strong>in</strong>al malleable stylet <strong>in</strong><br />
simulated difficult tracheal <strong>in</strong>tubation. Anesth 2000;55:886–9.<br />
77. Bra<strong>in</strong> AIJ. The laryngeal mask <strong>airway</strong>. Br J Anaesth 1983;55:<br />
801–4.<br />
78. Pennant JH. Laryngeal mask <strong>airway</strong>. Anesth 1993;79:144–63.<br />
79. Benumof JL. Use of <strong>the</strong> laryngeal mask <strong>airway</strong> to facilitate<br />
fiberoptic bronchoscopic <strong>in</strong>tubation. Anesth Analg<br />
1992;74:313–5.<br />
80. Benumof JL. Laryngeal mask <strong>airway</strong> and <strong>the</strong> ASA difficult <strong>airway</strong><br />
algorithm. Anesth 1996;84:686–99.<br />
81. Heath ML, Allaga<strong>in</strong> J. Intubation through <strong>the</strong> laryngeal mask.<br />
Anesth 1991;46:545–8.
<strong>Difficult</strong> Airway Management 47<br />
82. Devitt JH, Wenstone R, Noel AG, et al. The laryngeal mask<br />
<strong>airway</strong> and positive pressure ventilation. Anesth 1994;80:550–5.<br />
83. Brimacombe J, Keller C. The ProSeal laryngeal mask <strong>airway</strong>.<br />
Anesth 2000;93:104–9.<br />
84. Mart<strong>in</strong> PD, Cyna AM, Hunter WAH, et al. Tra<strong>in</strong><strong>in</strong>g nurs<strong>in</strong>g staff<br />
<strong>in</strong> <strong>airway</strong> <strong>management</strong> for resuscitation. Anesth 1993;448:33–7.<br />
85. Alexander R, Hodgson P, Lomax D, et al. A comparison of <strong>the</strong><br />
laryngeal mask <strong>airway</strong> and Guedel <strong>airway</strong>, bag and facemask for<br />
manual ventilation follow<strong>in</strong>g formal tra<strong>in</strong><strong>in</strong>g. Anesth 1993;48:<br />
231–4.<br />
86. Smith I, White PF. Use of <strong>the</strong> laryngeal mask <strong>airway</strong> as an<br />
alternative to a face mask dur<strong>in</strong>g outpatient arthroscopy. Anesth<br />
1992;77:850–5.<br />
87. Pennant JH, Walker MB. Comparison of <strong>the</strong> endotracheal tube<br />
and laryngeal mask <strong>in</strong> <strong>airway</strong> <strong>management</strong> by paramedical personnel.<br />
Anesth Analg 1992;74:531–4.<br />
88. Davies PRF, Tighe SQM, Greenslade GL, et al. Laryngeal mask<br />
<strong>airway</strong> and endotracheal tube <strong>in</strong>sertion by unskilled personnel.<br />
Lancet 1990;336:977–9.<br />
89. Brimacombe JR, Berry A. Mallampati class and laryngeal mask<br />
<strong>in</strong>sertion. Anaesth 1993;48:347–51.<br />
90. Parmet JL, Colonna–Romano P, Horrow JC, et al. The laryngeal<br />
mask <strong>airway</strong> reliably provides rescue ventilation <strong>in</strong> cases of<br />
unanticipated difficult tracheal <strong>in</strong>tubation along with difficult<br />
mask ventilation. Anesth Analg 1998;87:661–5.<br />
91. Patel SK, Whitten CW, Ivy R, et al. Failure of <strong>the</strong> laryngeal mask<br />
<strong>airway</strong>: an undiagnosed laryngeal carc<strong>in</strong>oma. Anesth Analg 1998;<br />
86:438–9.<br />
92. Pollack CV Jr. The laryngeal mask <strong>airway</strong>: a comprehensive<br />
review for <strong>the</strong> <strong>emergency</strong> physician. J Emerg Med 2001;20:53–6.<br />
93. Brimacombe JR, Berry A. The <strong>in</strong>cidence of aspiration associated<br />
with <strong>the</strong> laryngeal mask <strong>airway</strong>. J Cl<strong>in</strong> Anesth 1995;7:297–305.<br />
94. Brimacombe J, Keller C. The ProSeal laryngeal mask <strong>airway</strong>.<br />
Anesth 2000;93:104–9.<br />
95. Agro F, Brimacombe J, Carassiti M, et al. The <strong>in</strong>tubat<strong>in</strong>g laryngeal<br />
mask. Anesth 1998;53:1084–90.<br />
96. Baskett PJF, Parr MJA, Nolan JP. The <strong>in</strong>tubat<strong>in</strong>g laryngeal mask.<br />
Anesth 1998;53:1174–9.<br />
97. Bra<strong>in</strong> AIJ, Verghese C, Addy EV, et al. The <strong>in</strong>tubat<strong>in</strong>g laryngeal<br />
mask II. A prelim<strong>in</strong>ary cl<strong>in</strong>ical report of a new means of <strong>in</strong>tubat<strong>in</strong>g<br />
<strong>the</strong> trachea. Br J Anaesth 1997;79:704–9.<br />
98. Joo HS, Kapoor S, Rose DK, et al. The <strong>in</strong>tubat<strong>in</strong>g laryngeal mask<br />
<strong>airway</strong> after <strong>in</strong>duction of general anes<strong>the</strong>sia versus awake fiberoptic<br />
<strong>in</strong>tubation <strong>in</strong> patients with difficult <strong>airway</strong>s. Anesth Analg<br />
2001;92:1342–6.<br />
99. Asai T, Murao K, Tsutsumi T, et al. Ease of tracheal <strong>in</strong>tubation<br />
through <strong>the</strong> <strong>in</strong>tubationg laryngeal mask dur<strong>in</strong>g manual <strong>in</strong>-l<strong>in</strong>e<br />
head and neck stabilization. Anesth 2000;55:82–5.<br />
100. Rosenblatt WH, Murphy M. The <strong>in</strong>tubat<strong>in</strong>g laryngeal mask: use<br />
of a new ventilat<strong>in</strong>g-<strong>in</strong>tubat<strong>in</strong>g device <strong>in</strong> <strong>the</strong> <strong>emergency</strong> <strong>department</strong>.<br />
Ann Emerg Med 1999;33:234–8.<br />
101. Avidan MS, Harvey A, Chitkara N, et al. The <strong>in</strong>tubat<strong>in</strong>g laryngeal<br />
mask <strong>airway</strong> compared with direct laryngoscopy. Br J Anaesth<br />
1999;83:615–7.<br />
102. Choyce A, Avidan MS, Patel C, et al. Comparison of laryngeal<br />
mask and <strong>in</strong>tubat<strong>in</strong>g laryngeal mask <strong>in</strong>sertion by <strong>the</strong> naïve <strong>in</strong>tubator.<br />
Br J Anaesth 2000:84:103–5.<br />
103. Frass M, Johnson JC, A<strong>the</strong>rton GL, et al. Esophageal tracheal<br />
combitube for <strong>emergency</strong> <strong>in</strong>tubation. Resuscitation 1989;18:95–<br />
102.<br />
104. Pepe PE, Zachariah BD, Chandra NC. Invasive <strong>airway</strong> techniques<br />
<strong>in</strong> resuscitation. Ann Emerg Med 1993;22:393–403.<br />
105. Rumball CJ, MacDonald D. The PTL, combitube, laryngeal mask<br />
and oral <strong>airway</strong>. Prehospital Emerg Care 1997;1:1–10.<br />
106. Wissler RN. Esophageal tracheal combitube. Anesth Rev 1993;<br />
20:147–52.<br />
107. Staud<strong>in</strong>ger MD, Brugger S, Watsch<strong>in</strong>ger B. Emergency <strong>in</strong>tubation<br />
with <strong>the</strong> combitube. Ann Emerg Med 1993;22:1573–5.<br />
108. Frass M. Mechanical ventilation with <strong>the</strong> esophageal tracheal<br />
combitube <strong>in</strong> <strong>the</strong> <strong>in</strong>tensive care unit. Arch Emerg Med 1987;4:<br />
219–23.<br />
109. Frass M. Ventilation with <strong>the</strong> esophageal tracheal combitube <strong>in</strong><br />
cardiopulmonary resuscitation. Chest 1988;93:781–6.<br />
110. Vez<strong>in</strong>a D, Lessard MR, Bussieres J, et al. Complications associated<br />
with <strong>the</strong> use of <strong>the</strong> esophageal-tracheal combitube. Can J<br />
Anaesth 1998;45:76–80.<br />
111. Richards CF. Piriform s<strong>in</strong>us perforation dur<strong>in</strong>g esophageal-tracheal<br />
combitube placement. J Emerg Med 1999;17:37–9.<br />
112. Benumof JL, Scheller MS. The importance of transtracheal jet<br />
ventilation <strong>in</strong> <strong>the</strong> <strong>management</strong> of <strong>the</strong> difficult <strong>airway</strong>. Anesth<br />
1989;71:769–78.<br />
113. Jacobs HB, Smyth NPD, Witorsch P. Transtracheal ca<strong>the</strong>ter ventilation.<br />
Chest 1974;65:36–40.<br />
114. Kla<strong>in</strong> M, Smith RB. High frequency percutaneous transtracheal<br />
jet ventilation. Crit Care Med 1977;5:280–7.<br />
115. Weymuller EA, Paugh D, Pavl<strong>in</strong> EG, et al. Management of<br />
difficult <strong>airway</strong> problems with percutaneous transtracheal jet ventilation.<br />
Ann Otol Rh<strong>in</strong>ol Laryngol 1987;96:34–7.<br />
116. Jacobs HB. Needle ca<strong>the</strong>ter br<strong>in</strong>gs oxygen to <strong>the</strong> trachea. JAMA<br />
1972;222:1231–3.<br />
117. Dunlap LB. A modified, simple device for <strong>the</strong> <strong>emergency</strong> adm<strong>in</strong>istration<br />
of percutaneous transtracheal jet ventilation. J Am Coll<br />
Emerg Physicians 1978;7:42–6.<br />
118. Delisser EA, Muravchick S. Emergency transtracheal ventilation.<br />
Anesth 1981;55:606–7.<br />
119. Scuderi PE, McLeskey CH, Comer PB. Emergency percutaneous<br />
transtracheal ventilation dur<strong>in</strong>g anes<strong>the</strong>sia us<strong>in</strong>g readily available<br />
equipment. Anesth Analg 1982;61:867–70.<br />
120. Smith RB, Schaer WB, Pfaeffle H. Percutaneous transtracheal<br />
ventilation for anes<strong>the</strong>sia. Can J Anaesth 1975;22:607–9.<br />
121. Biro P, Moe KS. Emergency transtracheal jet ventilation <strong>in</strong> high<br />
grade <strong>airway</strong> obstruction. J Cl<strong>in</strong> Anesth 1997;9:604–6.<br />
122. Ravuss<strong>in</strong> P, Bayer–Berger M, Monnier P, et al. Percutaneous<br />
transtracheal ventilation for laser endoscopic procedures <strong>in</strong> <strong>in</strong>fants<br />
and small children with laryngeal obstruction. Report of two<br />
cases. Can J Anaesth 1987;34:83–86.<br />
123. Egol A, Culpepper JA, Snyder JV. Barotrauma and hypotension<br />
result<strong>in</strong>g from jet ventilation <strong>in</strong> critically ill patients. Chest 1985;<br />
88:98–102.<br />
124. Butler FS, Cirillo AA. Retrograde tracheal <strong>in</strong>tubation. Anesth<br />
Analg 1960;39:333–9.<br />
125. McNamara RM. Retrograde <strong>in</strong>tubation of <strong>the</strong> trachea. Ann Emerg<br />
Med 1987;16:680–3.<br />
126. Sanchez A, Pallares V. Retrograde <strong>in</strong>tubation technique. In Benumof<br />
JL, ed. Airway <strong>management</strong>. St. Louis: Mosby; 1996 pp.<br />
320–341.<br />
127. H<strong>in</strong>es MH, Meredith JW. Modified retrograde <strong>in</strong>tubation technique<br />
for rapid <strong>airway</strong> access. Am J Surg 1990;159:597–9.<br />
128. Barriott P, Riou B. Retrograde technique for tracheal <strong>in</strong>tubation <strong>in</strong><br />
trauma patients. Crit Care Med 1988;16:712–3.<br />
129. Yealy D. Recent advances <strong>in</strong> <strong>airway</strong> <strong>management</strong>. Emerg Med<br />
Cl<strong>in</strong> N Am 1989;7:83–93.<br />
130. Benumof JL. Management of <strong>the</strong> difficult adult <strong>airway</strong>. Anesth<br />
1991;75:1087–110.<br />
131. Casmely PA, Landesman S, Fynaman PN. Retrograde <strong>in</strong>tubation<br />
of patients undergo<strong>in</strong>g open heart surgery. Can Anaesth Soc J<br />
1985;32:661–5.<br />
132. Abou–Madi MN, Trop D. Pull<strong>in</strong>g vs. guid<strong>in</strong>g: a modification of<br />
retrograde guided <strong>in</strong>tubation. Can J Anaesth 1989;36:336–8.<br />
133. Ak<strong>in</strong>yemi OO. Complications of guided bl<strong>in</strong>d endotracheal <strong>in</strong>tubation.<br />
Anesth 1979;34:590–2.<br />
134. Poon YK. Case history: a life threaten<strong>in</strong>g complication of cricothyroid<br />
puncture. Anesth Analg 1976;55:298–300.<br />
135. Powell WF, Ozdil T. A translaryngeal guide for tracheal <strong>in</strong>tubation.<br />
Anesth Analg 1967;46:231–4.<br />
136. Stern Y, Spitzer T. Retrograde <strong>in</strong>tubation of <strong>the</strong> trachea. J Laryng<br />
Otolaryngol 1991;105:746–7.<br />
137. Guggenberger H, Lenz G, Heumann H. Success rate and complications<br />
of a modified, guided bl<strong>in</strong>d technique for <strong>in</strong>tubation <strong>in</strong> 36<br />
patients. Anaes<strong>the</strong>tist 1987;36:703–7.<br />
138. Lechman MJ, Donahoo JS, Macvaugh H. Endotracheal <strong>in</strong>tubation<br />
us<strong>in</strong>g percutaneous retrograde guidewire <strong>in</strong>sertion followed by
48 S. L. Orebaugh<br />
antegrade fiberoptic bronchoscopy. Crit Care Med 1986;14:589–<br />
90.<br />
139. Tobias R. Increased success with retrograde guide for endotracheal<br />
<strong>in</strong>tubation. Anesth Analg 1983;62:366–7.<br />
140. Ovassapian A. Fiberoptic <strong>airway</strong> endoscopy <strong>in</strong> critical care. In<br />
Ovassapian A, ed. Fiberoptic <strong>airway</strong> endoscopy <strong>in</strong> anes<strong>the</strong>sia and<br />
critical care. New York: Raven, 1990 pp. 105–128.<br />
141. Ovassapian A, Wheeler M. Fiberoptic endoscopy-aided techniques.<br />
In Benumof JL, ed. Airway <strong>management</strong>. St. Louis,<br />
Mosby; 1996 pp. 282–319.<br />
142. Ovassapian A, Doka JC, Romsa DE. Acromegaly. Use of fiberoptic<br />
laryngoscope to avoid tracheostomy. Anesth 1981;54:429–<br />
30.<br />
143. Edens ET, Sia RL. Flexible fiberoptic endoscopy <strong>in</strong> difficult<br />
<strong>in</strong>tubations. Ann Otol Rh<strong>in</strong>ol Laryngol 1981;90:307–9.<br />
144. Keenan MA, Stiles CM, Kaufman RL. Acquired laryngeal deviation<br />
associated with cervical sp<strong>in</strong>e disease <strong>in</strong> erosive, polyarticular<br />
arthritis. Anesth 1983;58:441–9.<br />
145. Ovassapian A, Yelian SJ, Dykes HM, et al. Fiberoptic nasotracheal<br />
<strong>in</strong>tubation. Anesth Anal 1983;62:692–5.<br />
146. Ovassapian A., Schreaker SC. Fiberoptic aided bronchial <strong>in</strong>tubation.<br />
Sem<strong>in</strong> Anesth 1987;6:133–45.<br />
147. Nakayama M, Kataoka N, Usui Y, et al. Techniques of nasotracheal<br />
<strong>in</strong>tubation with <strong>the</strong> fiberoptic bronchoscope. J Emerg Med<br />
1992;10:729–34.<br />
148. Mulder DS, Wallace DH, Woolhouse FM. The use of fiberoptic<br />
bronchoscope to facilitate endotracheal <strong>in</strong>tubation follow<strong>in</strong>g head<br />
and neck trauma. J Trauma 1975;15:638–40.<br />
149. Russell SH. Simultaneous use of two laryngoscopes. Anaesth<br />
1993;48:918.<br />
150. Ovassapian A. Fiberoptic tracheal <strong>in</strong>tubation with <strong>the</strong> esophagealtracheal<br />
combitube <strong>in</strong> place. Anesth Analg 1993;75:S315.<br />
151. Delaney KA, Hessler R. Emergency flexible nasotracheal <strong>in</strong>tubation:<br />
a report of 60 cases. Ann Emerg Med 1988;17:919–25.<br />
152. Schafermeyer RW. Fiberoptic laryngoscopy <strong>in</strong> <strong>the</strong> <strong>emergency</strong><br />
<strong>department</strong>. Am J Emerg Med 1983;2:160–3.<br />
153. Ml<strong>in</strong>ek EJ Jr, Cl<strong>in</strong>ton JE, Plummer D, et al. Fiberoptic <strong>in</strong>tubation<br />
<strong>in</strong> <strong>the</strong> <strong>emergency</strong> <strong>department</strong>. Ann Emerg Med 1990;19:359–62.<br />
154. Watts AD, Gelb AW, Bach DB, et al. Comparison of <strong>the</strong> Bullard<br />
and MacIntosh laryngoscopes for endotracheal <strong>in</strong>tubation of patients<br />
with a potential cervical sp<strong>in</strong>e <strong>in</strong>jury. Anesth 1997;87:<br />
1335–42.<br />
155. Shulman GB, Connelly NR. A comparison of <strong>the</strong> Bullard laryngoscope<br />
versus <strong>the</strong> flexible fiberoptic bronchoscope dur<strong>in</strong>g <strong>in</strong>tubation<br />
<strong>in</strong> patients afforded <strong>in</strong>-l<strong>in</strong>e stabilization. J Cl<strong>in</strong> Anesth<br />
2001;13:182–5.<br />
156. Fridrich P, Frass M, Krenn CG, et al. The Upsherscope <strong>in</strong> rout<strong>in</strong>e<br />
and difficult <strong>airway</strong> <strong>management</strong>: a randomized, controlled cl<strong>in</strong>ical<br />
trial. Anesth Analg 1997;85:1377–81.<br />
157. Smith CE, P<strong>in</strong>chak AB, Sidhu TS, et al. Evaluation of tracheal<br />
<strong>in</strong>tubation difficulty <strong>in</strong> patients with cervical sp<strong>in</strong>e immobilization.<br />
Anesth 1999;91:1253–9.<br />
158. Brantigan CO, Grow JB. Cricothyoidotomy: elective use <strong>in</strong> respiratory<br />
problems requir<strong>in</strong>g tracheostomy. J Thor Cardiovasc<br />
Surg 1976;71:72–80.<br />
159. Brantigan CO, Grow JB. Cricothyroidotomy revisited aga<strong>in</strong>. Ear<br />
Nose Throat J 1980;59:289–95.<br />
160. Brofeldt BT, Panacek EA, Richards JR. An easy cricothyrotomy<br />
approach: <strong>the</strong> rapid four step technique. Acad Emerg Med 1996;<br />
3:1060–3.<br />
161. Holmes JF, Panacek EA, Sakles JC, et al. Comparison of two<br />
cricothyotomy techniques. Ann Emerg Med 1998;32:442–7.<br />
162. Davis DP, Bramwell KJ, Vilke GM, et al. Cricothyrotomy technique:<br />
standard versus <strong>the</strong> rapid four-step technique. J Emerg<br />
Med 1999;17:1071–3.<br />
163. Melker RJ, Florete OG Jr. Percutaneous dilational cricothyrotomy<br />
and tracheostomy. In: Airway <strong>management</strong>. Benumof JL,<br />
ed. St. Louis: Mosby; 1996: pp. 484–512.<br />
164. Chan TC, Vilke GM, Bramwell KJ, et al. Comparison of wireguided<br />
cricothyrotomy versus standard surgical cricothyrotomy<br />
technique. J Emerg Med 1999;17:957–62.<br />
165. Eisenberger P, Laczika K, List M, et al. Comparison of conventional<br />
surgical versus Seld<strong>in</strong>ger technique <strong>emergency</strong> cricothyrotomy<br />
performed by <strong>in</strong>experienced cl<strong>in</strong>icians. Anesth 2000;92:<br />
687–90.<br />
166. Sise MJ, Shackford SR, Cruickshank JC, et al. cricothyrotomy for<br />
long-term tracheal access. Ann Surg 1984;200:13–9.<br />
167. Spaite DW, Maralee J. Prehospital cricothyrotomy: an <strong>in</strong>vestigation<br />
of <strong>in</strong>dications, technique, complications, and patient outcome.<br />
Ann Emerg Med 1990;19:279–85.<br />
168. Boyle MF, Hatton D, Sheets C. Surgical cricothyrotomy performed<br />
by air ambulance flight nurses: a 5-year experience.<br />
J Emerg Med 1993;11:41–5.<br />
169. Knill RL. <strong>Difficult</strong> laryngoscopy made easy with a “BURP.” Can<br />
J Anaesth 1993;40:279–82.<br />
170. Benumof JL, Cooper SL. Quantitative improvement <strong>in</strong> laryngoscopic<br />
view by optimal external laryngeal pressure. J Cl<strong>in</strong> Anesth<br />
1996;8:136–40.<br />
171. Henderson JJ. The use of paraglossal straight blade laryngoscopy<br />
<strong>in</strong> difficult tracheal <strong>in</strong>tubation. Anaesth 1997;52:552–60.