Preparing the Wound Bed – Debridement, Bacterial Balance, and ...
Preparing the Wound Bed – Debridement, Bacterial Balance, and ...
Preparing the Wound Bed – Debridement, Bacterial Balance, and ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
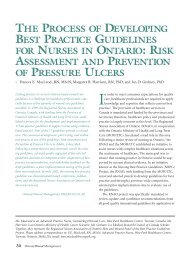
Safe <strong>and</strong> Effective<br />
Selected Use<br />
Caution<br />
Cadexomer iodine<br />
Ionized silver<br />
Silver sulphadiazine<br />
Polymyxin B sulphate<br />
<strong>–</strong> Bacitracin<br />
zinc<br />
Mupirocin<br />
Metronidazole<br />
Benzoyl peroxide<br />
Gentamicin<br />
Fucidin<br />
Polymyxin B sulphate<br />
<strong>–</strong> Bacitracin<br />
zinc neomycin<br />
+ = effective against bacteria<br />
strong enough for cytoxicity. It should be used with caution<br />
in patients with thyroid disease <strong>and</strong> iodine allergy. If cadexomer<br />
iodine is used on large areas or for long periods, monitoring<br />
of thyroid function is advised.<br />
Ionized silver dressing (Acticoat ; Westaim Biomedical,<br />
Exeter, NH, Fort Saskatchewan, Alberta, Canada) has a slow<br />
release of silver, combined with an absorptive polyester pad.<br />
The silver has a broad spectrum of antibacterial coverage<br />
<strong>and</strong> can be used very successfully to decrease friable exudative<br />
tissue on <strong>the</strong> wound surface. Acticoat must be used<br />
with sterile water because <strong>the</strong> chloride in saline precipitates<br />
<strong>the</strong> silver to inactive silver chloride. Acticoat contains no<br />
sulfa, which may be present in o<strong>the</strong>r silver preparations.<br />
Topical antibacterials will only treat <strong>the</strong> wound surface<br />
<strong>and</strong> not deeper infection. Their use should be re-evaluated<br />
after 2 weeks or if symptoms or signs of deeper infection<br />
occur. 40<br />
Recommendation 10<br />
Use Systemic Antibiotics if Symptoms or Signs of<br />
28 Ostomy<strong>Wound</strong> Management<br />
TABLE 7<br />
CHOOSING APPROPRIATE ANTIMICROBIALS<br />
Staphylococcus<br />
aureus<br />
+<br />
+<br />
+<br />
+<br />
Weak<br />
+<br />
+<br />
+<br />
MRSA Streptococcus Pseudomonas Anaerobes<br />
+<br />
+<br />
+<br />
+<br />
+<br />
Weak<br />
+<br />
+<br />
+<br />
+<br />
+<br />
Weak<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
+<br />
Weak<br />
+<br />
Comments<br />
Good autolytic debridement;<br />
limited potential for bacterial<br />
resistance. Caution with<br />
thyroid disease<br />
Use with water, not saline.<br />
Limited potential for bacterial<br />
resistance<br />
Not for use in sulfa<strong>–</strong>sensitive<br />
patients<br />
Reserve for MRSA <strong>and</strong> o<strong>the</strong>r<br />
resistant Gram-positive<br />
organisms<br />
Reserve for anaerobes <strong>and</strong><br />
odor control<br />
For use on large wounds. Can<br />
cause irritation/allergies<br />
Reserve for oral/IV use<br />
Ointment contains lanolin,<br />
which can sensitize to cause<br />
allergic contact dermatitis<br />
Contains neomycin, which<br />
causes an allergic contact<br />
dermatitis, may cross sensitize<br />
to aminoglycosides<br />
Infection Extend Beyond <strong>Wound</strong> Margin or <strong>the</strong><br />
Ulcer Probes to Bone<br />
Systemic antibiotics should be used if infection extends<br />
beyond <strong>the</strong> ulcer margin. Ulcers of less than 1-month duration<br />
require primary Gram-positive coverage primarily for at<br />
least 2 weeks or until clinical symptoms <strong>and</strong> signs resolve. If<br />
immunosuppression is an issue, broad spectrum agents,<br />
including Gram-negatives <strong>and</strong> anaerobes, should be included.<br />
A semiquantitative swab is often helpful when patients<br />
fail to respond to <strong>the</strong> initial <strong>the</strong>rapy. In complex cases, an<br />
infectious disease consult is advised.<br />
If an ulcer probes to bone, osteomyelitis must be suspected.<br />
Antibiotics for longer periods are necessary, usually for at<br />
least 4 to 6 weeks. Treatment progress can be monitored<br />
with x-rays, erythrocyte sedimentation rate, C reactive protein,<br />
<strong>and</strong>, rarely, nuclear scans. Nonhealing ulcers may<br />
require surgical debridement. For a more detailed discussion<br />
on this topic, see Recommendation 8 of Best Practices for <strong>the</strong><br />
Prevention, Diagnosis, <strong>and</strong> Treatment of Diabetic Foot Ulcers<br />
by Inlow et al on page 63.