Comparison of rate of canine retraction with conventional molar ...
Comparison of rate of canine retraction with conventional molar ...
Comparison of rate of canine retraction with conventional molar ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
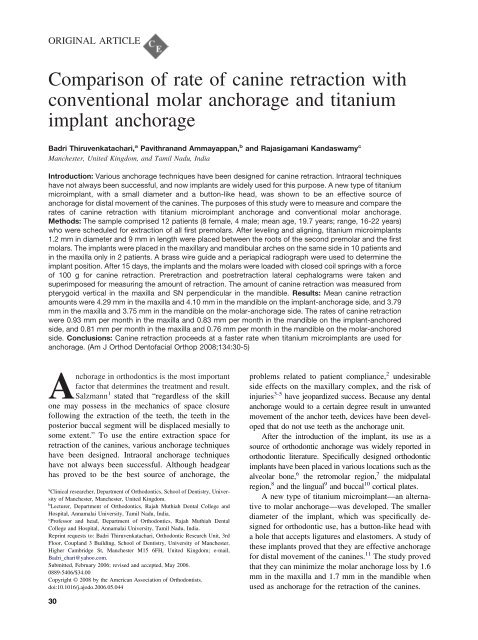
ORIGINAL ARTICLE<br />
<strong>Comparison</strong> <strong>of</strong> <strong>rate</strong> <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> <strong>with</strong><br />
<strong>conventional</strong> <strong>molar</strong> anchorage and titanium<br />
implant anchorage<br />
Badri Thiruvenkatachari, a Pavithranand Ammayappan, b and Rajasigamani Kandaswamy c<br />
Manchester, United Kingdom, and Tamil Nadu, India<br />
Introduction: Various anchorage techniques have been designed for <strong>canine</strong> <strong>retraction</strong>. Intraoral techniques<br />
have not always been successful, and now implants are widely used for this purpose. A new type <strong>of</strong> titanium<br />
microimplant, <strong>with</strong> a small diameter and a button-like head, was shown to be an effective source <strong>of</strong><br />
anchorage for distal movement <strong>of</strong> the <strong>canine</strong>s. The purposes <strong>of</strong> this study were to measure and compare the<br />
<strong>rate</strong>s <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> <strong>with</strong> titanium microimplant anchorage and <strong>conventional</strong> <strong>molar</strong> anchorage.<br />
Methods: The sample comprised 12 patients (8 female, 4 male; mean age, 19.7 years; range, 16-22 years)<br />
who were scheduled for extraction <strong>of</strong> all first pre<strong>molar</strong>s. After leveling and aligning, titanium microimplants<br />
1.2 mm in diameter and 9 mm in length were placed between the roots <strong>of</strong> the second pre<strong>molar</strong> and the first<br />
<strong>molar</strong>s. The implants were placed in the maxillary and mandibular arches on the same side in 10 patients and<br />
in the maxilla only in 2 patients. A brass wire guide and a periapical radiograph were used to determine the<br />
implant position. After 15 days, the implants and the <strong>molar</strong>s were loaded <strong>with</strong> closed coil springs <strong>with</strong> a force<br />
<strong>of</strong> 100 g for <strong>canine</strong> <strong>retraction</strong>. Pre<strong>retraction</strong> and post<strong>retraction</strong> lateral cephalograms were taken and<br />
superimposed for measuring the amount <strong>of</strong> <strong>retraction</strong>. The amount <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> was measured from<br />
pterygoid vertical in the maxilla and SN perpendicular in the mandible. Results: Mean <strong>canine</strong> <strong>retraction</strong><br />
amounts were 4.29 mm in the maxilla and 4.10 mm in the mandible on the implant-anchorage side, and 3.79<br />
mm in the maxilla and 3.75 mm in the mandible on the <strong>molar</strong>-anchorage side. The <strong>rate</strong>s <strong>of</strong> <strong>canine</strong> <strong>retraction</strong><br />
were 0.93 mm per month in the maxilla and 0.83 mm per month in the mandible on the implant-anchored<br />
side, and 0.81 mm per month in the maxilla and 0.76 mm per month in the mandible on the <strong>molar</strong>-anchored<br />
side. Conclusions: Canine <strong>retraction</strong> proceeds at a faster <strong>rate</strong> when titanium microimplants are used for<br />
anchorage. (Am J Orthod Dent<strong>of</strong>acial Orthop 2008;134:30-5)<br />
Anchorage in orthodontics is the most important<br />
factor that determines the treatment and result.<br />
Salzmann 1 stated that “regardless <strong>of</strong> the skill<br />
one may possess in the mechanics <strong>of</strong> space closure<br />
following the extraction <strong>of</strong> the teeth, the teeth in the<br />
posterior buccal segment will be displaced mesially to<br />
some extent.” To use the entire extraction space for<br />
<strong>retraction</strong> <strong>of</strong> the <strong>canine</strong>s, various anchorage techniques<br />
have been designed. Intraoral anchorage techniques<br />
have not always been successful. Although headgear<br />
has proved to be the best source <strong>of</strong> anchorage, the<br />
a Clinical researcher, Department <strong>of</strong> Orthodontics, School <strong>of</strong> Dentistry, University<br />
<strong>of</strong> Manchester, Manchester, United Kingdom.<br />
b Lecturer, Department <strong>of</strong> Orthodontics, Rajah Muthiah Dental College and<br />
Hospital, Annamalai University, Tamil Nadu, India.<br />
c Pr<strong>of</strong>essor and head, Department <strong>of</strong> Orthodontics, Rajah Muthiah Dental<br />
College and Hospital, Annamalai University, Tamil Nadu, India.<br />
Reprint requests to: Badri Thiruvenkatachari, Orthodontic Research Unit, 3rd<br />
Floor, Coupland 3 Building, School <strong>of</strong> Dentistry, University <strong>of</strong> Manchester,<br />
Higher Cambridge St, Manchester M15 6FH, United Kingdom; e-mail,<br />
Badri_chari@yahoo.com.<br />
Submitted, February 2006; revised and accepted, May 2006.<br />
0889-5406/$34.00<br />
Copyright © 2008 by the American Association <strong>of</strong> Orthodontists.<br />
doi:10.1016/j.ajodo.2006.05.044<br />
30<br />
problems related to patient compliance, 2 undesirable<br />
side effects on the maxillary complex, and the risk <strong>of</strong><br />
injuries 3-5 have jeopardized success. Because any dental<br />
anchorage would to a certain degree result in unwanted<br />
movement <strong>of</strong> the anchor teeth, devices have been developed<br />
that do not use teeth as the anchorage unit.<br />
After the introduction <strong>of</strong> the implant, its use as a<br />
source <strong>of</strong> orthodontic anchorage was widely reported in<br />
orthodontic literature. Specifically designed orthodontic<br />
implants have been placed in various locations such as the<br />
alveolar bone, 6 the retro<strong>molar</strong> region, 7 the midpalatal<br />
region, 8 and the lingual 9 and buccal 10 cortical plates.<br />
A new type <strong>of</strong> titanium microimplant—an alternative<br />
to <strong>molar</strong> anchorage—was developed. The smaller<br />
diameter <strong>of</strong> the implant, which was specifically designed<br />
for orthodontic use, has a button-like head <strong>with</strong><br />
a hole that accepts ligatures and elastomers. A study <strong>of</strong><br />
these implants proved that they are effective anchorage<br />
for distal movement <strong>of</strong> the <strong>canine</strong>s. 11 The study proved<br />
that they can minimize the <strong>molar</strong> anchorage loss by 1.6<br />
mm in the maxilla and 1.7 mm in the mandible when<br />
used as anchorage for the <strong>retraction</strong> <strong>of</strong> the <strong>canine</strong>s.
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
Volume 134, Number 1<br />
Fig 1. Implants in position: A, implant anchorage; B, <strong>molar</strong> anchorage.<br />
The purposes <strong>of</strong> this study were to measure the<br />
amount <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> and to compare and measure<br />
the <strong>rate</strong>s <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> <strong>with</strong> implant anchorage<br />
and <strong>conventional</strong> <strong>molar</strong> anchorage.<br />
MATERIAL AND METHODS<br />
In this study, we chose subjects from the patients at<br />
the Department <strong>of</strong> Orthodontics, Annamalai University, in<br />
Tamil Nadu, India, for orthodontic treatment. Twelve<br />
patients were selected (mean age, 19.7 years; range, 16-22<br />
years; 8 female, 4 male). This study was reviewed and<br />
approved by the Institutional Review Board.<br />
The patients were chosen according to the following<br />
criteria: (1) comprehensive medical and dental history<br />
ruling out systemic illness, (2) therapeutic extraction <strong>of</strong><br />
the first pre<strong>molar</strong>s required, (3) leveling and aligning<br />
completed, and (4) maximum anchorage needed, <strong>with</strong><br />
75% to100% <strong>of</strong> space closure used for <strong>retraction</strong> <strong>of</strong> the<br />
anterior segment. 12 All subjects had an arch length-basal<br />
bone discrepancy <strong>of</strong> more than 5 mm. Patients <strong>with</strong> Angle<br />
Class I malocclusion and an ANB angle between 2° and<br />
4° were selected for implant placement in both the maxilla<br />
and the mandible; for patients <strong>with</strong> Angle Class II malocclusion<br />
and an ANB angle above 5°, implant placement<br />
was restricted to the maxilla, as a part <strong>of</strong> camouflage<br />
treatment. No anchorage preservation methods were used<br />
until the end <strong>of</strong> the study for any patient.<br />
After initial leveling and aligning, a 0.016 0.022-in<br />
stainless steel archwire was placed. Informed consent was<br />
obtained for all patients before placement <strong>of</strong> the implants.<br />
Routine blood studies ruled out any blood<br />
dyscrasias. The titanium microimplants <strong>of</strong> 1.2 mm in<br />
diameter and 9 mm in length were positioned at the<br />
maximum thickness <strong>of</strong> interdental bone between the roots<br />
<strong>of</strong> the second pre<strong>molar</strong> and the first <strong>molar</strong> on the selected<br />
quadrant 13 (Fig 1). Orthodontic forces were applied 15<br />
days after implant placement. Nickel-titanium closed-coil<br />
springs <strong>with</strong> a force <strong>of</strong> 100 g (measured <strong>with</strong> the Dontix<br />
gauge; American Orthodontics, Sheboygan, Wis) were<br />
stretched between the implant and the <strong>canine</strong> on the<br />
Thiruvenkatachari, Ammayappan, and Kandaswamy 31<br />
Fig 2. Schematic diagram showing the L-shaped wire<br />
in the buccal tube for differentiating the <strong>molar</strong>s on<br />
lateral cephalograms.<br />
implant-anchored side and between the <strong>molar</strong> and the<br />
<strong>canine</strong> on the <strong>molar</strong>-anchored side. The period <strong>of</strong> the<br />
study was 4 to 6 months.<br />
Two sets <strong>of</strong> records were taken; the first was before<br />
implant placement, and other when <strong>canine</strong> <strong>retraction</strong><br />
was complete in accordance <strong>with</strong> the patient’s treatment<br />
plan. These included study models, cephalometric<br />
radiographs, orthopantomograms, and photographs.<br />
To differentiate the right and left sides on the lateral<br />
cephalogram, a 0.0175 0.025-in stainless steel wire<br />
in an L-shape <strong>with</strong> 0.5 cm <strong>of</strong> vertical length and 1 cm<br />
<strong>of</strong> horizontal length was placed in the buccal tube <strong>of</strong><br />
<strong>molar</strong>s 11 (Fig 2). The right and left <strong>canine</strong>s were<br />
identified by tracing them along the archwire from the
32 Thiruvenkatachari, Ammayappan, and Kandaswamy<br />
respective <strong>molar</strong>s to the archwire-bracket junction in<br />
the <strong>canine</strong> bracket.<br />
The amount <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> was measured by<br />
using a stable landmark in the cranium as a reference.<br />
In the maxilla, the pre<strong>retraction</strong> and post<strong>retraction</strong><br />
lateral cephalometric tracings were superimposed by<br />
McNamara’s method. 14 The horizontal distance from<br />
the pterygoid vertical to the tip <strong>of</strong> the <strong>canine</strong> hook on<br />
both sides was calculated. 14<br />
In the mandible, the cephalograms were superimposed<br />
according to Bjork’s method. 15 The horizontal<br />
distance was calculated from sella vertical to the tip <strong>of</strong><br />
the <strong>canine</strong> hook on both sides. 16<br />
The <strong>rate</strong> <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> was calculated by<br />
dividing the amount <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> by time taken<br />
for <strong>retraction</strong>.<br />
The data obtained were subjected to statistical analysis.<br />
Means, standard errors, and standard deviations were<br />
tabulated, <strong>with</strong> the Student t test used to determine the<br />
level <strong>of</strong> significance and correlation <strong>of</strong> the <strong>rate</strong> <strong>of</strong> <strong>canine</strong><br />
<strong>retraction</strong> between implant anchorage and <strong>conventional</strong><br />
<strong>molar</strong> anchorage in the maxilla and the mandible.<br />
RESULTS<br />
The <strong>canine</strong>s were successfully retracted in all subjects<br />
(Figs 3-6). Canine <strong>retraction</strong> was considered<br />
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
July 2008<br />
Fig 3. Canine <strong>retraction</strong> using closed-coil springs on implant anchored side: A, before <strong>retraction</strong>;<br />
B, after <strong>retraction</strong>.<br />
Fig 4. Canine <strong>retraction</strong> using closed-coil springs on <strong>molar</strong> anchored side: A, before <strong>retraction</strong>;<br />
B, after <strong>retraction</strong>.<br />
complete when the extraction space was closed on the<br />
<strong>molar</strong>-anchored side. The duration <strong>of</strong> the study was 4 to<br />
6 months (Tables I and II).<br />
The amounts <strong>of</strong> distal movement <strong>of</strong> <strong>canine</strong>s <strong>with</strong><br />
implants as anchorage were 4.29 mm in the maxilla and<br />
4.10 mm in the mandible (Table III). The distal<br />
movements <strong>of</strong> the <strong>canine</strong>s <strong>with</strong> <strong>conventional</strong> <strong>molar</strong><br />
anchorage were 3.79 mm in the maxilla and 3.75 mm in<br />
mandible (Table III). The average differences were 0.6<br />
mm in the maxilla and 0.35 mm in the mandible. These<br />
values were statistically significant (P 0.01).<br />
The <strong>rate</strong>s <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> were 0.93 mm per<br />
month in the maxilla and 0.83 mm per month in the<br />
mandible on the implant-anchored side, and 0.81 mm<br />
per month in the maxilla and 0.76 mm per month in the<br />
mandible on the <strong>molar</strong>-anchored side (Table IV). The<br />
mean differences in the <strong>rate</strong> <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> were<br />
0.12 mm per month in the maxilla and 0.07 mm per<br />
month in the mandible. These values were statistically<br />
significant (P 0.01).<br />
DISCUSSION<br />
Canine <strong>retraction</strong> is a common treatment procedure<br />
in orthodontics. Various appliances are used for <strong>retraction</strong><br />
<strong>of</strong> the <strong>canine</strong>s to close extraction spaces. The<br />
<strong>retraction</strong> <strong>of</strong> <strong>canine</strong>s depends on various factors: the
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
Volume 134, Number 1<br />
Fig 5. Lateral cephalometric tracing before <strong>canine</strong><br />
<strong>retraction</strong>.<br />
appliance used, the force applied, the technique used,<br />
and the periodontal ligament area.<br />
Although various studies deal <strong>with</strong> the relationship<br />
between optimum force magnitude and <strong>rate</strong> <strong>of</strong> <strong>canine</strong><br />
<strong>retraction</strong>, few human studies have been reported. The<br />
first such study for comparing this relationship was by<br />
Story and Smith, 17 who reported an optimum force <strong>of</strong><br />
150 to 200 g for <strong>retraction</strong> <strong>of</strong> the mandibular <strong>canine</strong>s.<br />
Iwasaki et al 18 reported that forces as low as 18 g could<br />
cause effective tooth movement and recommended that<br />
optimum pressure should be less than 100 g. Ricketts 19<br />
advocated 75 g, and Lee 20 recommended 150 to 200 g<br />
as the optimum pressure value for <strong>canine</strong> <strong>retraction</strong>.<br />
Boester and Johnston 21 reported 140 to 300 g, and<br />
Paulsen et al 22 used 50 to 75 g for <strong>canine</strong> <strong>retraction</strong>.<br />
Huffman and Way 23 advocated 200 g as the optimum<br />
force. Hixon et al 24 reported that higher forces produce<br />
more effective tooth movement. In an experimental study<br />
on mini-implants, Buchter et al 25 showed that immediate<br />
loading <strong>of</strong> implants <strong>with</strong> a force <strong>of</strong> 100 cN had a high<br />
success <strong>rate</strong>. It is generally thought that light forces are<br />
more biologic and less painful. Because reports have<br />
shown effective tooth movement <strong>with</strong> light forces, a force<br />
<strong>of</strong> 100 g was applied <strong>with</strong> nickel-titanium closed-coil<br />
springs in this study for <strong>retraction</strong> <strong>of</strong> the <strong>canine</strong>s into the<br />
pre<strong>molar</strong> extraction spaces. 18,19,22<br />
Studies have dealt <strong>with</strong> <strong>canine</strong> <strong>retraction</strong> <strong>with</strong><br />
various techniques and appliances. The reported <strong>rate</strong>s<br />
<strong>of</strong> <strong>canine</strong> <strong>retraction</strong> have varied from 0.35 to 1.55 mm<br />
per month. Paulsen et al 22 showed an average <strong>canine</strong><br />
Thiruvenkatachari, Ammayappan, and Kandaswamy 33<br />
Fig 6. Lateral cephalometric tracing after <strong>canine</strong><br />
<strong>retraction</strong>.<br />
<strong>retraction</strong> <strong>rate</strong> <strong>of</strong> 1 mm per month. That value is<br />
comparable <strong>with</strong> our study. In the study <strong>of</strong> Sonis et al, 26<br />
the <strong>rate</strong>s <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> were 0.99 to 1.51 mm in<br />
3 weeks. The differences in their <strong>retraction</strong> <strong>rate</strong>s and<br />
ours were probably due to the high force levels used in<br />
their study. In a randomized clinical trial by Dixon<br />
et al, 27 the mean <strong>rate</strong> <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> <strong>with</strong> nickeltitanium<br />
coil springs was 0.81 mm per month. Darendelier<br />
et al 28 compared pull coil springs and drum<br />
springs in adults and reported an average <strong>rate</strong> <strong>of</strong> <strong>canine</strong><br />
<strong>retraction</strong> <strong>of</strong> 0.87 mm per month <strong>with</strong> pull coil springs.<br />
Those results were similar to ours. Boester and<br />
Johnston 21 showed <strong>canine</strong> <strong>retraction</strong> <strong>rate</strong>s <strong>of</strong> 3.24 and<br />
2.05 mm in 2 months in the maxilla and the mandible,<br />
respectively. Their results were higher than in our study<br />
and can be attributed to the difference in force levels<br />
used. Sleichter 29 showed a <strong>canine</strong> <strong>retraction</strong> <strong>rate</strong> <strong>of</strong><br />
1 mm per month; this is close to the value we obtained.<br />
Hixon et al 24 obtained a <strong>rate</strong> <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> <strong>of</strong> 0.17<br />
mm per week for a force <strong>of</strong> 100 g, a similar result to<br />
this study.<br />
Not many human studies report the <strong>rate</strong> <strong>of</strong> <strong>canine</strong><br />
<strong>retraction</strong>, and no study reports the <strong>rate</strong> <strong>of</strong> <strong>canine</strong><br />
<strong>retraction</strong> against a stable anchorage unit. In this study,<br />
the movement <strong>of</strong> the <strong>canine</strong> against the stable anchorage<br />
unit, the titanium microimplant, was analyzed.<br />
Canines were retracted faster <strong>with</strong> implant anchors, and<br />
the differences in average amount <strong>of</strong> <strong>canine</strong> <strong>retraction</strong><br />
were 0.6 mm in the maxilla and 0.35 mm in the<br />
mandible. The difference in the <strong>rate</strong>s <strong>of</strong> <strong>retraction</strong>
34 Thiruvenkatachari, Ammayappan, and Kandaswamy<br />
Table I. Amount, <strong>rate</strong>, and period <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> in the maxilla<br />
Subject Age/sex<br />
Amount <strong>of</strong> <strong>canine</strong> <strong>retraction</strong><br />
(mm)<br />
Rate <strong>of</strong> <strong>canine</strong> <strong>retraction</strong><br />
(mm/mo)<br />
Implant side Molar side Period <strong>of</strong> study (mo) Implant side Molar side<br />
1 21/F 4.5 4.0 5 0.9 0.8<br />
2 18/M 3.5 3.5 4 0.875 0.875<br />
3 18/F 4.5 3.5 5 0.9 0.7<br />
4 21/F 4 3.5 5 0.8 0.7<br />
5 19/F 4.5 4.5 4.5 1 1<br />
6 20/M 5 4 4.5 1.11 0.88<br />
7 21/F 4 3.5 5 0.9 0.7<br />
8 21/F 5 4.5 4 1.25 1.125<br />
9 20/F 4 4 4.5 0.88 0.88<br />
10 19/M 4.5 4 5.5 0.81 0.727<br />
11 21/F 4 3.5 5 0.8 0.7<br />
12 19/M 4 3 4.5 0.88 0.66<br />
F, Female; M, male.<br />
Table II. Amount, <strong>rate</strong>, and period <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> in the mandible<br />
Subject Age/sex<br />
Amount <strong>of</strong> <strong>canine</strong> <strong>retraction</strong><br />
(mm)<br />
Rate <strong>of</strong> <strong>canine</strong> <strong>retraction</strong><br />
(mm/mo)<br />
Implant side Molar side Period <strong>of</strong> study (mo) Implant side Molar side<br />
1 21/F 4 4 5 0.8 0.8<br />
2 18/M 3.5 3.5 4 0.875 0.875<br />
3 18/F 4.5 4 5 0.9 0.8<br />
4 21/F 4 3.5 6 0.666 0.58<br />
5 19/F 4.5 4 4.5 1 0.88<br />
6 20/M 4.5 4 5 0.9 0.8<br />
7 21/F 3.5 3.5 5 0.636 0.636<br />
8 21/F 4.5 4 5.5 0.818 0.727<br />
9 21/F 4 3.5 5 0.8 0.7<br />
10 19/M 4 3.5 4.5 0.88 0.77<br />
F, Female; M, male.<br />
Table III. <strong>Comparison</strong> <strong>of</strong> amounts <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> between sides in the maxilla and the mandible<br />
Implant-anchored side Molar-anchored side<br />
Mean (mm) SD Mean (mm) SD<br />
Canine <strong>retraction</strong>, maxilla (n 12) 4.2917 0.45017 3.7917 0.45017 *<br />
Canine <strong>retraction</strong>, mandible (n 10) 4.1000 0.39441 3.7500 0.26352 *<br />
*P 0.01.<br />
Table IV. <strong>Comparison</strong> <strong>of</strong> <strong>rate</strong>s <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> between sides in the maxilla and the mandible<br />
Implant-anchored side Molar-anchored side<br />
Mean (mm/mo) SD Mean (mm/mo) SD<br />
Canine <strong>retraction</strong>, maxilla (n 12) 0.9254 0.13429 0.8128 0.14314 *<br />
Canine <strong>retraction</strong>, mandible (n 10) 0.8275 0.11037 0.7568 0.09712 *<br />
*P 0.01.<br />
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
July 2008<br />
P<br />
P
American Journal <strong>of</strong> Orthodontics and Dent<strong>of</strong>acial Orthopedics<br />
Volume 134, Number 1<br />
between the <strong>molar</strong> and the implant anchorage might be<br />
because <strong>of</strong> the anchorage loss on the <strong>molar</strong>-anchorage<br />
side, and thus forces are reduced as the <strong>canine</strong>s are<br />
retracted. The results prove that implants are efficient<br />
anchors and produce faster <strong>canine</strong> <strong>retraction</strong>.<br />
At the end <strong>of</strong> the study, the asymmetric <strong>molar</strong>anchorage<br />
loss was managed by allowing mesial movement<br />
<strong>of</strong> the <strong>molar</strong>s on the implant-anchored side.<br />
The main reason for this study was to validate the<br />
<strong>rate</strong> <strong>of</strong> <strong>canine</strong> <strong>retraction</strong> <strong>with</strong> titanium implant anchors.<br />
This method evolved from the desire to achieve the best<br />
result for an important and necessary stage for many<br />
orthodontic patients, <strong>with</strong> minimal undesirable tooth<br />
changes. Implants produce effective <strong>canine</strong> <strong>retraction</strong><br />
by using the entire extraction space. 13 With increasing<br />
demands on orthodontists to treat more patients in<br />
shorter times, attention to quality <strong>of</strong> treatment is essential.<br />
Titanium microimplants can bring about more<br />
effective <strong>canine</strong> <strong>retraction</strong> in a shorter time.<br />
CONCLUSIONS<br />
Implant anchorage produced more <strong>canine</strong> <strong>retraction</strong><br />
than <strong>conventional</strong> <strong>molar</strong> anchorage. The <strong>rate</strong> <strong>of</strong> <strong>canine</strong><br />
<strong>retraction</strong> was faster <strong>with</strong> implant anchorage than <strong>with</strong><br />
<strong>molar</strong> anchorage. The use <strong>of</strong> implants as anchorage for<br />
the <strong>retraction</strong> <strong>of</strong> <strong>canine</strong>s is a viable alternative to<br />
<strong>conventional</strong> <strong>molar</strong> anchorage.<br />
We thank Pr<strong>of</strong> Kevin O’Brien for his valuable<br />
insights in preparing this manuscript and Dr Hee Moon<br />
Kyung for providing the implants.<br />
REFERENCES<br />
1. Salzmann JA. Principles <strong>of</strong> orthodontics. 2nd ed. Philadelphia:<br />
Lippincott; 1966.<br />
2. Clemmer EJ, Hayes EW. Patient cooperation in wearing headgear.<br />
Am J Orthod 1979;75:517-24.<br />
3. Samuels RH, Willner F, Knox J, Jones ML. A national survey <strong>of</strong><br />
orthodontic facebow injuries in the UK and Eire. Br J Orthod<br />
1996;23:11-20.<br />
4. Holland GN, Wallace DA, Mondino BJ, Cole SH, Ryan SJ.<br />
Severe ocular injuries from orthodontic headgear. Arch Ophthalmol<br />
1985;103:649-51.<br />
5. Dickson G. Contact dermatitis and cervical headgear. Br Dent J<br />
1983;155:112.<br />
6. Odman J, Lekholm U, Jemt T, Thilander B. Osseointeg<strong>rate</strong>d<br />
implants as orthodontic anchorage in the treatment <strong>of</strong> partially<br />
edentulous adult patients. Eur J Orthod 1997;31:<br />
763-7.<br />
7. Roberts WE, Marshall KJ, Mozsary PG. Rigid endosseous<br />
implant utilized as anchorage to protract <strong>molar</strong>s and close an<br />
atrophic extraction site. Angle Orthod 1990;60:135-52.<br />
8. Block MS, H<strong>of</strong>fman DR. A new device for absolute anchorage<br />
for orthodontics. Am J Orthod Dent<strong>of</strong>acial Orthop 1995;107:<br />
251-8.<br />
Thiruvenkatachari, Ammayappan, and Kandaswamy 35<br />
9. Lee JS, Park HS, Kyung HM. Micro-implant anchorage for<br />
lingual treatment <strong>of</strong> a skeletal Class II malocclusion. J Clin<br />
Orthod 2001;35:643-7.<br />
10. Kyung HM, Park HS, Bae SM, Sung VH, Bongkim IL. Development<br />
<strong>of</strong> orthodontic microimplants for intraoral anchorage.<br />
J Clin Orthod 2003;37:321-8.<br />
11. Thiruvenkatachari B, Pavithranand A, Rajasigamani K, Kyung<br />
HM. <strong>Comparison</strong> and measurement <strong>of</strong> the amount <strong>of</strong> anchorage<br />
loss <strong>of</strong> the <strong>molar</strong>s <strong>with</strong> and <strong>with</strong>out the use <strong>of</strong> implant anchorage<br />
during <strong>canine</strong> <strong>retraction</strong>. Am J Orthod Dent<strong>of</strong>acial Orthop<br />
2006;129:551-4.<br />
12. Nanda R. Biomechanics in clinical orthodontics. Philadelphia:<br />
W. B Saunders; 1997.<br />
13. Park HS, Bae SM, Kyung HM, Sung JH. Micro-implant anchorage<br />
for treatment <strong>of</strong> skeletal bialveolar protrusion. J Clin Orthod<br />
2001;35:417-22.<br />
14. McNamara JA. A method <strong>of</strong> cephalometric evaluation. Am J<br />
Orthod 1984;86:449-69.<br />
15. Bjork A. Prediction <strong>of</strong> mandibular growth rotation. Am J Orthod<br />
1969;75:39-53.<br />
16. Pancherz H, Ruf S, Kohlhas P. “Effective condylar growth” and<br />
chin position in Herbst treatment: a cephalometric roentgenographic<br />
long-term study. Am J Orthod Dent<strong>of</strong>acial Orthop<br />
1998;114:437-46.<br />
17. Storey E, Smith R. Force in orthodontics and its relations to tooth<br />
movement. Aust J Dent 1952;56:11-8.<br />
18. Iwasaki L, Haack JE, Nickel JC, Morton J. Human tooth<br />
movement in response to continuous stress <strong>of</strong> low magnitude.<br />
Am J Orthod Dent<strong>of</strong>acial Orthop 2000;117:175-83.<br />
19. Ricketts RM. Development <strong>of</strong> <strong>retraction</strong> sections. Foundations <strong>of</strong><br />
Orthodontic Research Newsletter 1974;5:41-4.<br />
20. Lee BW. Relationship between tooth-movement <strong>rate</strong> and estimated<br />
pressure applied. J Dent Res 1965;44:1053.<br />
21. Boester CH, Johnston LE. A clinical investigation <strong>of</strong> the concepts<br />
<strong>of</strong> differential and optimum force in <strong>canine</strong> <strong>retraction</strong>.<br />
Angle Orthod 1972;44:113-9.<br />
22. Paulsen RC, Speidel TM, Isaacson RJ. A laminographic study <strong>of</strong><br />
cuspid <strong>retraction</strong> versus <strong>molar</strong> anchorage loss. Angle Orthod<br />
1970;40:20-7.<br />
23. Huffman DJ, Way DC. A clinical evaluation <strong>of</strong> tooth movement<br />
along arch wires <strong>of</strong> two different sizes. Am J Orthod 1983;83:<br />
453-9.<br />
24. Hixon EH, Atikian H, Callow GE, McDonald HW, Tacy RJ.<br />
Optimal force, differential force, and anchorage. Am J Orthod<br />
1969;55:437-57.<br />
25. Buchter A, Wiechmann D, Koerdt S, Wiesmann HP, Piffko J,<br />
Meyer U. Load-related implant reaction <strong>of</strong> mini-implants used for<br />
orthodontic anchorage. Clin Oral Implants Res 2005;16:473-9.<br />
26. Sonis AL, Van der Plas E, Gianelly A. A comparison <strong>of</strong><br />
elastomeric auxiliaries versus elastic thread on pre<strong>molar</strong><br />
extraction site closure: an in vivo study. Am J Orthod<br />
1986;89:73-8.<br />
27. Dixon V, Read MFJ, O’Brien KD, Worthington HV, Mandall<br />
NA. A randomized clinical trial to compare three methods <strong>of</strong><br />
orthodontic space closure. J Orthod 2002;29:31-6.<br />
28. Darendeliler MA, Darendeliler H, Uner O. The drum spring (DS)<br />
retractor: a constant and continuous force for <strong>canine</strong> <strong>retraction</strong>.<br />
Eur J Orthod 1997;19:115-30.<br />
29. Sleichter CG. A clinical assessment <strong>of</strong> light and heavy forces<br />
in the closure <strong>of</strong> extraction spaces. Angle Orthod 1971;41:<br />
66-75.