

Eble JN, Sauter G., Epstein JI, Sesterhenn IA - iarc
Eble JN, Sauter G., Epstein JI, Sesterhenn IA - iarc
Eble JN, Sauter G., Epstein JI, Sesterhenn IA - iarc

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
A<br />
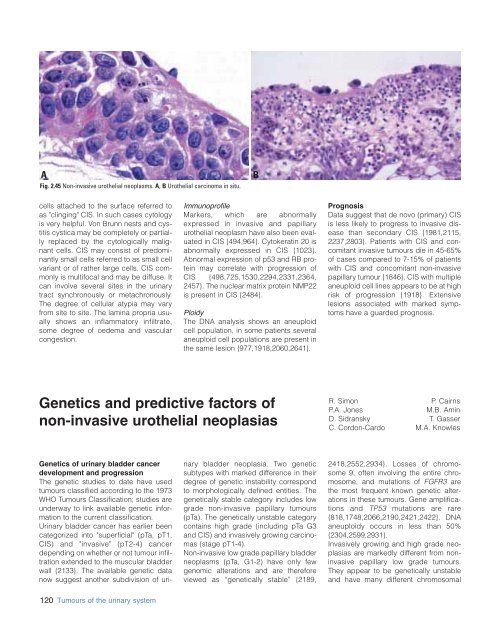
Fig. 2.45 Non-invasive urothelial neoplasms. A, B Urothelial carcinoma in situ.<br />
B<br />
cells attached to the surface referred to<br />
as "clinging" CIS. In such cases cytology<br />
is very helpful. Von Brunn nests and cystitis<br />
cystica may be completely or partially<br />
replaced by the cytologically malignant<br />
cells. CIS may consist of predominantly<br />
small cells referred to as small cell<br />
variant or of rather large cells. CIS commonly<br />
is multifocal and may be diffuse. It<br />
can involve several sites in the urinary<br />
tract synchronously or metachronously.<br />
The degree of cellular atypia may vary<br />
from site to site. The lamina propria usually<br />
shows an inflammatory infiltrate,<br />
some degree of oedema and vascular<br />
congestion.<br />
Immunoprofile<br />
Markers, which are abnormally<br />
expressed in invasive and papillary<br />
urothelial neoplasm have also been evaluated<br />
in CIS {494,964}. Cytokeratin 20 is<br />
abnormally expressed in CIS {1023}.<br />
Abnormal expression of p53 and RB protein<br />
may correlate with progression of<br />
CIS {498,725,1530,2294,2331,2364,<br />
2457}. The nuclear matrix protein NMP22<br />
is present in CIS {2484}.<br />
Ploidy<br />
The DNA analysis shows an aneuploid<br />
cell population, in some patients several<br />
aneuploid cell populations are present in<br />
the same lesion {977,1918,2060,2641}.<br />
Prognosis<br />
Data suggest that de novo (primary) CIS<br />
is less likely to progress to invasive disease<br />
than secondary CIS {1981,2115,<br />
2237,2803}. Patients with CIS and concomitant<br />
invasive tumours die in 45-65%<br />
of cases compared to 7-15% of patients<br />
with CIS and concomitant non-invasive<br />
papillary tumour {1846}. CIS with multiple<br />
aneuploid cell lines appears to be at high<br />
risk of progression {1918}. Extensive<br />
lesions associated with marked symptoms<br />
have a guarded prognosis.<br />
Genetics and predictive factors of<br />
non-invasive urothelial neoplasias<br />
R. Simon<br />
P.A. Jones<br />
D. Sidransky<br />
C. Cordon-Cardo<br />
P. Cairns<br />
M.B. Amin<br />
T. Gasser<br />
M.A. Knowles<br />
Genetics of urinary bladder cancer<br />
development and progression<br />
The genetic studies to date have used<br />
tumours classified according to the 1973<br />
WHO Tumours Classification; studies are<br />
underway to link available genetic information<br />
to the current classification.<br />
Urinary bladder cancer has earlier been<br />
categorized into "superficial" (pTa, pT1,<br />
CIS) and "invasive" (pT2-4) cancer<br />
depending on whether or not tumour infiltration<br />
extended to the muscular bladder<br />
wall {2133}. The available genetic data<br />
now suggest another subdivision of urinary<br />
bladder neoplasia. Two genetic<br />
subtypes with marked difference in their<br />
degree of genetic instability correspond<br />
to morphologically defined entities. The<br />
genetically stable category includes low<br />
grade non-invasive papillary tumours<br />
(pTa). The genetically unstable category<br />
contains high grade (including pTa G3<br />
and CIS) and invasively growing carcinomas<br />
(stage pT1-4).<br />
Non-invasive low grade papillary bladder<br />
neoplasms (pTa, G1-2) have only few<br />
genomic alterations and are therefore<br />
viewed as “genetically stable” {2189,<br />
2418,2552,2934}. Losses of chromosome<br />
9, often involving the entire chromosome,<br />
and mutations of FGFR3 are<br />
the most frequent known genetic alterations<br />
in these tumours. Gene amplifications<br />
and TP53 mutations are rare<br />
{818,1748,2066,2190,2421,2422}. DNA<br />
aneuploidy occurs in less than 50%<br />
{2304,2599,2931}.<br />
Invasively growing and high grade neoplasias<br />
are markedly different from noninvasive<br />
papillary low grade tumours.<br />
They appear to be genetically unstable<br />
and have many different chromosomal<br />
120 Tumours of the urinary system














