Round Table Report - UCT Main - University of Cape Town
Round Table Report - UCT Main - University of Cape Town
Round Table Report - UCT Main - University of Cape Town

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
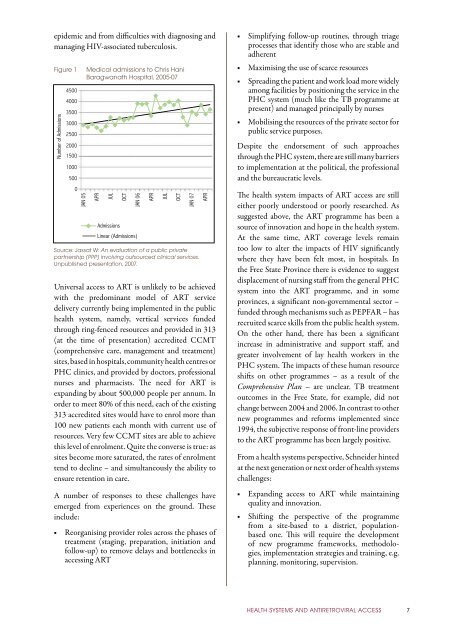
epidemic and from difficulties with diagnosing and<br />
managing HIV-associated tuberculosis.<br />
Figure 1<br />
Number <strong>of</strong> Admissions<br />
4500<br />
4000<br />
3500<br />
3000<br />
2500<br />
2000<br />
1500<br />
1000<br />
500<br />
0<br />
JAN 05<br />
Medical admissions to Chris Hani<br />
Baragwanath Hospital, 2005-07<br />
APR<br />
JUL<br />
Admissions<br />
OCT<br />
JAN 06<br />
Linear (Admissions)<br />
APR<br />
JUL<br />
OCT<br />
JAN 07<br />
Source: Jassat W: An evaluation <strong>of</strong> a public private<br />
partnership (PPP) involving outsourced clinical services.<br />
Unpublished presentation, 2007.<br />
APR<br />
Universal access to ART is unlikely to be achieved<br />
with the predominant model <strong>of</strong> ART service<br />
delivery currently being implemented in the public<br />
health system, namely, vertical services funded<br />
through ring-fenced resources and provided in 313<br />
(at the time <strong>of</strong> presentation) accredited CCMT<br />
(comprehensive care, management and treatment)<br />
sites, based in hospitals, community health centres or<br />
PHC clinics, and provided by doctors, pr<strong>of</strong>essional<br />
nurses and pharmacists. The need for ART is<br />
expanding by about 500,000 people per annum. In<br />
order to meet 80% <strong>of</strong> this need, each <strong>of</strong> the existing<br />
313 accredited sites would have to enrol more than<br />
100 new patients each month with current use <strong>of</strong><br />
resources. Very few CCMT sites are able to achieve<br />
this level <strong>of</strong> enrolment. Quite the converse is true: as<br />
sites become more saturated, the rates <strong>of</strong> enrolment<br />
tend to decline – and simultaneously the ability to<br />
ensure retention in care.<br />
A number <strong>of</strong> responses to these challenges have<br />
emerged from experiences on the ground. These<br />
include:<br />
■■ Reorganising provider roles across the phases <strong>of</strong><br />
treatment (staging, preparation, initiation and<br />
follow-up) to remove delays and bottlenecks in<br />
accessing ART<br />
■■ Simplifying follow-up routines, through triage<br />
processes that identify those who are stable and<br />
adherent<br />
■■ Maximising the use <strong>of</strong> scarce resources<br />
■■ Spreading the patient and work load more widely<br />
among facilities by positioning the service in the<br />
PHC system (much like the TB programme at<br />
present) and managed principally by nurses<br />
■■ Mobilising the resources <strong>of</strong> the private sector for<br />
public service purposes.<br />
Despite the endorsement <strong>of</strong> such approaches<br />
through the PHC system, there are still many barriers<br />
to implementation at the political, the pr<strong>of</strong>essional<br />
and the bureaucratic levels.<br />
The health system impacts <strong>of</strong> ART access are still<br />
either poorly understood or poorly researched. As<br />
suggested above, the ART programme has been a<br />
source <strong>of</strong> innovation and hope in the health system.<br />
At the same time, ART coverage levels remain<br />
too low to alter the impacts <strong>of</strong> HIV significantly<br />
where they have been felt most, in hospitals. In<br />
the Free State Province there is evidence to suggest<br />
displacement <strong>of</strong> nursing staff from the general PHC<br />
system into the ART programme, and in some<br />
provinces, a significant non-governmental sector –<br />
funded through mechanisms such as PEPFAR – has<br />
recruited scarce skills from the public health system.<br />
On the other hand, there has been a significant<br />
increase in administrative and support staff, and<br />
greater involvement <strong>of</strong> lay health workers in the<br />
PHC system. The impacts <strong>of</strong> these human resource<br />
shifts on other programmes – as a result <strong>of</strong> the<br />
Comprehensive Plan – are unclear. TB treatment<br />
outcomes in the Free State, for example, did not<br />
change between 2004 and 2006. In contrast to other<br />
new programmes and reforms implemented since<br />
1994, the subjective response <strong>of</strong> front-line providers<br />
to the ART programme has been largely positive.<br />
From a health systems perspective, Schneider hinted<br />
at the next generation or next order <strong>of</strong> health systems<br />
challenges:<br />
■■ Expanding access to ART while maintaining<br />
quality and innovation.<br />
■■ Shifting the perspective <strong>of</strong> the programme<br />
from a site-based to a district, populationbased<br />
one. This will require the development<br />
<strong>of</strong> new programme frameworks, method ologies,<br />
implementation strategies and training, e.g.<br />
planning, monitoring, supervision.<br />
Health systems and antiretroviral access 7