CHOC Seizure Action Plan
CHOC Seizure Action Plan
CHOC Seizure Action Plan

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
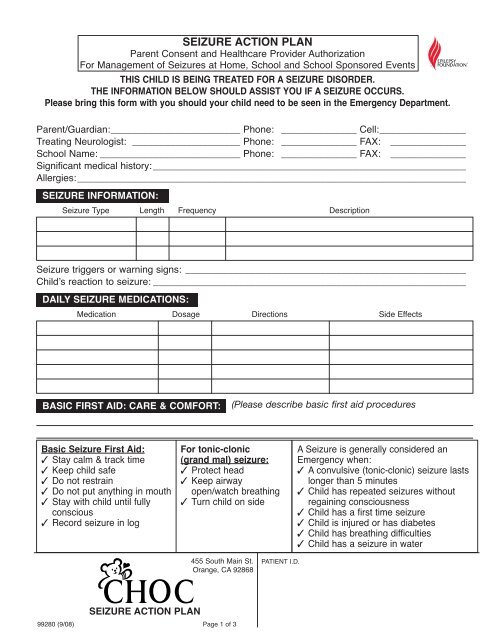
SEIZURE ACTION PLAN<br />
Parent Consent and Healthcare Provider Authorization<br />
For Management of <strong>Seizure</strong>s at Home, School and School Sponsored Events<br />
THIS CHILD IS BEING TREATED FOR A SEIZURE DISORDER.<br />
THE INFORMATION BELOW SHOULD ASSIST YOU IF A SEIZURE OCCURS.<br />
Please bring this form with you should your child need to be seen in the Emergency Department.<br />
Parent/Guardian:________________________ Phone: ______________ Cell:________________<br />
Treating Neurologist: ____________________ Phone: ______________ FAX: ______________<br />
School Name: __________________________ Phone: ______________ FAX: ______________<br />
Significant medical history:__________________________________________________________<br />
Allergies:________________________________________________________________________<br />
SEIZURE INFORMATION:<br />
<strong>Seizure</strong> Type Length Frequency Description<br />
<strong>Seizure</strong> triggers or warning signs: ____________________________________________________<br />
Childʼs reaction to seizure: __________________________________________________________<br />
DAILY SEIZURE MEDICATIONS:<br />
Medication Dosage Directions Side Effects<br />
BASIC FIRST AID: CARE & COMFORT:<br />
(Please describe basic first aid procedures<br />
Basic <strong>Seizure</strong> First Aid:<br />
✓ Stay calm & track time<br />
✓ Keep child safe<br />
✓ Do not restrain<br />
✓ Do not put anything in mouth<br />
✓ Stay with child until fully<br />
conscious<br />
✓ Record seizure in log<br />
For tonic-clonic<br />
(grand mal) seizure:<br />
✓ Protect head<br />
✓ Keep airway<br />
open/watch breathing<br />
✓ Turn child on side<br />
A <strong>Seizure</strong> is generally considered an<br />
Emergency when:<br />
✓ A convulsive (tonic-clonic) seizure lasts<br />
longer than 5 minutes<br />
✓ Child has repeated seizures without<br />
regaining consciousness<br />
✓ Child has a first time seizure<br />
✓ Child is injured or has diabetes<br />
✓ Child has breathing difficulties<br />
✓ Child has a seizure in water<br />
455 South Main St.<br />
Orange, CA 92868<br />
PATIENT I.D.<br />
SEIZURE ACTION PLAN<br />
99280 (9/08) Page 1 of 3
SEIZURE ACTION PLAN<br />
Parent Consent and Healthcare Provider Authorization<br />
For Management of <strong>Seizure</strong>s at Home, School and School Sponsored Events<br />
EMERGENCY RESPONSE:<br />
A “seizure emergency” for this child is defined as:________________________________________<br />
______________________________________________________________________________<br />
______________________________________________________________________________<br />
<strong>Seizure</strong> Emergency Protocol: (Check all that apply and clarify below)<br />
Contact school Nurse<br />
Call 911 for transport to __________________________________________________________<br />
Notify parent or emergency contact<br />
Parent to notify doctor<br />
(<strong>CHOC</strong> Neurology Clinic at 714-532-7601 (M-F 8-4:30) or 866-316-3347 (after hours)<br />
Administer emergency medications as indicated below<br />
Other ________________________________________________________________________<br />
“AS NEEDED” TREATMENT PROTOCOL:<br />
Emergency/Rescue Medication<br />
Diastat _________ mg Acudial:<br />
• Give ______mg per rectum for seizures > ____minutes; or in clusters > ____seizures in 1 hr<br />
• Call 911 if the seizures do not stop ______ minutes after you give the rescue medication or if<br />
child has problems breathing during or after the seizure.<br />
• Side Effects: drowsiness, sleepiness, fatigue, poor coordination, unsteadiness, behavior<br />
change<br />
Does child have a Vagus Nerve Stimulator (VNS)? YES NO<br />
If YES, Describe magnet use ________________________________________________________<br />
Parental Instructions for Routine Medication Dose Change<br />
Medication Dosage & Directions When to Give<br />
455 South Main St.<br />
Orange, CA 92868<br />
PATIENT I.D.<br />
SEIZURE ACTION PLAN<br />
99280 (9/08) Page 2 of 3
SEIZURE ACTION PLAN<br />
Parent Consent and Healthcare Provider Authorization<br />
For Management of <strong>Seizure</strong>s at Home, School and School Sponsored Events<br />
SPECIAL CONSIDERATIONS & SAFETY PRECAUTIONS:<br />
(re: school activities, sports, trips, etc.)<br />
None<br />
No contact sports<br />
No use of power tools/power equipment<br />
No swimming<br />
Other: ________________________________________________________________________<br />
Does child need to leave the classroom after a seizure? YES NO<br />
If YES, describe process for returning child to classroom __________________________________<br />
______________________________________________________________________________<br />
Authorized Health Care Provider Authorization for Management of <strong>Seizure</strong>s at School<br />
My signature below provides authorization for the above written order, including administration of<br />
Diastat. I understand that all procedures will be implemented in accordance with state laws and<br />
regulations. I understand that specialized physical health care services may be performed by<br />
unlicensed designated school personnel under the training and supervision provided by the school<br />
nurse. This authorization is for a maximum of one year. If changes are indicated, I will provide new<br />
written authorization (may be faxed).<br />
<strong>CHOC</strong> Neurology Department:<br />
Neurologist Signature __________________________ Date: __________Time: __________<br />
1120 West LaVeta Ave. #125, Orange, CA 92868 Phone # (714) 532-7601 Fax # (714) 532-7650<br />
Parent Consent for Management of <strong>Seizure</strong>s at School<br />
I (We), the parent/guardian of the above named student request that the following for Management of<br />
<strong>Seizure</strong>s in school be administered to our child in accordance with state laws and regulations.<br />
I will:<br />
1. Provide the necessary supplies and equipment, including 3 day emergency supply of<br />
medication<br />
2. Notify the school nurse if there is a change in the student health status or change of<br />
physician<br />
3. Notify the school nurse immediately and provide new consent for any changes in<br />
doctorʼs orders<br />
I authorize the school nurse to communicate with the Authorized Health Care Provider when<br />
necessary. I understand that I will be provided a copy of my childʼs completed Individual School<br />
Healthcare <strong>Plan</strong> (ISHP)<br />
Parent Signature: ____________________________________________ Date: ________________<br />
School Nurse Signature: ______________________________________ Date: ________________<br />
455 South Main St.<br />
Orange, CA 92868<br />
PATIENT I.D.<br />
SEIZURE ACTION PLAN<br />
99280 (9/08) Page 3 of 3