Diseases of the salivary glands
Diseases of the salivary glands
Diseases of the salivary glands

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Diseases</strong> <strong>of</strong> <strong>the</strong> <strong>salivary</strong> <strong>glands</strong><br />
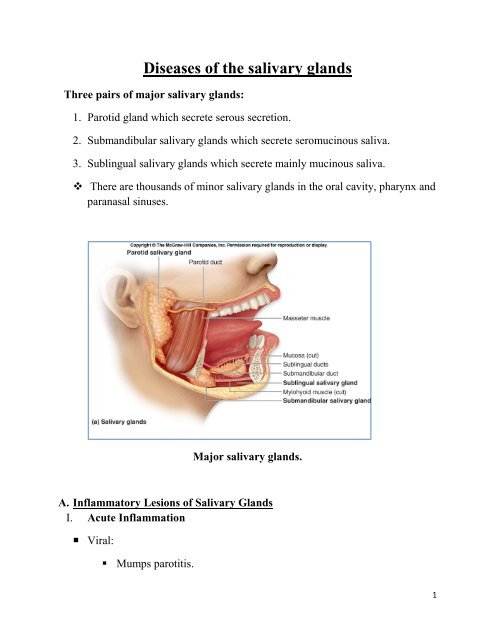
Three pairs <strong>of</strong> major <strong>salivary</strong> <strong>glands</strong>:<br />
1. Parotid gland which secrete serous secretion.<br />
2. Submandibular <strong>salivary</strong> <strong>glands</strong> which secrete seromucinous saliva.<br />
3. Sublingual <strong>salivary</strong> <strong>glands</strong> which secrete mainly mucinous saliva.<br />
There are thousands <strong>of</strong> minor <strong>salivary</strong> <strong>glands</strong> in <strong>the</strong> oral cavity, pharynx and<br />
paranasal sinuses.<br />
Major <strong>salivary</strong> <strong>glands</strong>.<br />
A. Inflammatory Lesions <strong>of</strong> Salivary Glands<br />
I. Acute Inflammation<br />
• Viral:<br />
• Mumps parotitis.<br />
1
• Bacterial<br />
• Acute suppurative parotitis<br />
Parotid abscess.<br />
Mumps.<br />
II.<br />
Chronic inflammation:<br />
• Chronic parotitis (Sialectasis): dilation <strong>of</strong> ductules <strong>of</strong> <strong>the</strong> parotid due to<br />
fibrosis <strong>of</strong> its proximal parts due to intercurrent inflammation (or stones).<br />
The gland is enlarged, s<strong>of</strong>t tender, usually bilaterally with attacks <strong>of</strong> acute<br />
exacerpations with high fever and pain.<br />
• Mikulicz’ syndrome: Enlargement <strong>of</strong> all <strong>the</strong> <strong>salivary</strong> <strong>glands</strong> (parotid,<br />
submandibular and sublinguals in addition to lachrymal gland. It is an<br />
autoimmune disease.<br />
• Sjögren’s syndrome: is similar to Mikilicz plus dryness <strong>of</strong> mouth and eye –<br />
xerostomia and xerophthalmia.<br />
B. Cysts <strong>of</strong> <strong>the</strong> <strong>salivary</strong> <strong>glands</strong><br />
Mucocele: It is a retention cyst which affect ei<strong>the</strong>r minor <strong>salivary</strong> <strong>glands</strong> (in <strong>the</strong><br />
oral cavity especially in <strong>the</strong> buccal mucosa) or in <strong>the</strong> major <strong>salivary</strong> <strong>glands</strong>.<br />
2
Rannula: A mucocele <strong>of</strong> <strong>the</strong> sublingual <strong>salivary</strong> gland, it presents as large tense<br />
bluish swelling in <strong>the</strong> floor <strong>of</strong> mouth which displaces <strong>the</strong> tongue.<br />
Mucocele<br />
Ranula<br />
C. Stones <strong>of</strong> <strong>the</strong> <strong>salivary</strong> <strong>glands</strong><br />
They are 30 times more common in submandibular <strong>glands</strong> than in parotids. Why?<br />
• Secretion <strong>of</strong> submandibular gland is more viscid.<br />
• The drainage is less dependent.<br />
• The opening <strong>of</strong> <strong>the</strong> submandibular duct is in <strong>the</strong> floor <strong>of</strong> <strong>the</strong> mouth, so food<br />
debris can precipitate in it.<br />
Clinical picture<br />
• The obstruction caused by <strong>the</strong> stone toge<strong>the</strong>r with <strong>the</strong> superadded infection<br />
leads to acute (or chronic) submandibular calculous sialadenitis.<br />
• This condition is manifested by pain and swelling <strong>of</strong> <strong>the</strong> gland on eating,<br />
swelling or seeing food. It may be associated with fever.<br />
• Clinically, <strong>the</strong> gland is felt bidigitally, <strong>the</strong> stone can be felt as well in <strong>the</strong><br />
floor <strong>of</strong> mouth.<br />
3
The submandibular stone lies in one <strong>of</strong> four positions;<br />
(1) meatal, (2) intraductal,(3) juxtaglandular, and (4) intraglandular.<br />
Treatment<br />
Anatomy <strong>of</strong> <strong>the</strong> submandibular gland.<br />
• meatal stone: only meatotomy and extraction.<br />
• intraductal stone: open <strong>the</strong> duct in <strong>the</strong> floor <strong>of</strong> mouth under local (nerve<br />
block) or general anaes<strong>the</strong>sia, extract <strong>the</strong> stone and do not close <strong>the</strong> incision.<br />
• juxtaglandular stone: do not try to extract <strong>the</strong> stone intra-orally to avoid<br />
injury to lingual nerve which hooks on <strong>the</strong> duct at this point, so excision <strong>of</strong><br />
<strong>the</strong> gland is mandatory.<br />
• intraglandular stone: The treatment is submandibular sialadenectomy.<br />
D. Tumours <strong>of</strong> <strong>salivary</strong> <strong>glands</strong><br />
The larger <strong>the</strong> gland, <strong>the</strong> more benign is <strong>the</strong> higher incidence<br />
Parotid <strong>glands</strong> 80% benign,<br />
Submandibular 60% benign,<br />
4
Minor <strong>salivary</strong> <strong>glands</strong> 50% malignant.<br />
Parotid is gland <strong>of</strong> tumor while submandibular is a gland <strong>of</strong> stones.<br />
Criteria <strong>of</strong> parotid gland swelling.<br />
• Elevation <strong>of</strong> ear lobule<br />
• Obliteration <strong>of</strong> furrow between <strong>the</strong> mandible and mastoid process.<br />
• Get prominent on clenching <strong>of</strong> teeth.<br />
• Less prominent on opening <strong>of</strong> <strong>the</strong> mouth.<br />
Benign tumors<br />
1. Pleomorphic adenoma<br />
Rule <strong>of</strong> 80%<br />
• 80% <strong>of</strong> tumors <strong>of</strong> <strong>salivary</strong> occurs in parotid<br />
• 80% <strong>of</strong> <strong>the</strong>m are benign<br />
• 80% <strong>of</strong> <strong>the</strong>m are pleomorphic adenoma<br />
Treatment:<br />
Superficial parotidectomy. If <strong>the</strong> tumour is in <strong>the</strong> deep lobe, we do total<br />
conservative parotidectomy.<br />
2. Warthin’s tumour. ( Adenolymphoma or Papillary cystadenoma<br />
lymphomatosum).<br />
• It occurs after 60 years <strong>of</strong> age, male to female = 4:1.<br />
• Only occurs in <strong>the</strong> parotid gland (15% <strong>of</strong> all parotid tumours).<br />
• Mostly in <strong>the</strong> tail <strong>of</strong> <strong>the</strong> parotid.<br />
• It is s<strong>of</strong>t or cystic.<br />
• It has high incidence <strong>of</strong> bilaterality and multiplicity.<br />
5
• Treatment: Superficial parotidectomy.<br />
Malignant <strong>salivary</strong> gland tumors.<br />
1. Acinic cell carcinoma<br />
It is a low grade tumour with very late lymph node and distant metastasis.<br />
Prognosis is good in comparison to o<strong>the</strong>r types.<br />
2. Mucoepidermoid carcinoma (2 types)<br />
Low grade malignancy type.<br />
High grade variant: with lymph nodes.<br />
3. Adenoid cystic carcinoma (cylinderoma)<br />
It is aggressive and has tendency to perineural spread even intracranially.<br />
4. Carcinoma ex pleomorphic adenoma (rare).<br />
Clinical picture <strong>of</strong> a malignant <strong>salivary</strong> tumors:<br />
• Pain.<br />
• Rapid rate <strong>of</strong> growth.<br />
• Consistency is mainly hard.<br />
• Facial nerve dysfunction or even paralysis.<br />
• Fixity to skin → Ulceration.<br />
• Fixity to deeper structures: muscles, bone.<br />
• Cervical lymph node metastasis.<br />
• Bone and lung metastasis.<br />
Investigations <strong>of</strong> a <strong>salivary</strong> gland mass<br />
• X-ray: Oblique view and intra-oral film for submandibular stone.<br />
6
• Ultrasonography.<br />
• CT.<br />
• MRI.<br />
• PET.<br />
• FNAC.<br />
• Sialography: Dye study is beneficial in diagnosing sialectasis.<br />
7