

PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
to charge $17,000? How do I, as a practitioner<br />
and as a leader, signal to the marketplace<br />
– my patients, my team – that we’re<br />
worth it?” Because the difference between<br />
the $10,000 and the $17,000 reconstruction,<br />
when it’s done well, is huge. You can’t be<br />
doing reconstructions half-assed, because it<br />
will come back to haunt you. So the higher-fee<br />
cases are more difficult to sell. Case<br />
acceptance for the high-fee case is something<br />
that I have focused on for the last 20<br />
years of my life.<br />
MD: Now, in those 20 years that you’ve been<br />
focusing on high-fee case acceptance, is there<br />
a huge difference between case acceptance for<br />
a $10,000 case and a $17,000 case? Don’t they<br />
both sound relatively expensive to the patient?<br />
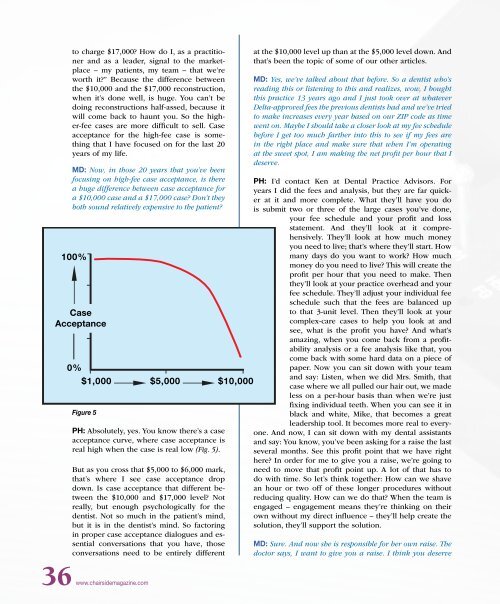
100%<br />
Case<br />
Acceptance<br />
0%<br />
$1,000 $5,000 $10,000<br />
Figure 5<br />
PH: Absolutely, yes. You know there’s a case<br />
acceptance curve, where case acceptance is<br />
real high when the case is real low (Fig. 5).<br />
But as you cross that $5,000 to $6,000 mark,<br />
that’s where I see case acceptance drop<br />
down. Is case acceptance that different between<br />
the $10,000 and $17,000 level? Not<br />
really, but enough psychologically for the<br />
dentist. Not so much in the patient’s mind,<br />
but it is in the dentist’s mind. So factoring<br />
in proper case acceptance dialogues and essential<br />
conversations that you have, those<br />
conversations need to be entirely different<br />
at the $10,000 level up than at the $5,000 level down. And<br />
that’s been the topic of some of our other articles.<br />
MD: Yes, we’ve talked about that before. So a dentist who’s<br />
reading this or listening to this and realizes, wow, I bought<br />
this practice 13 years ago and I just took over at whatever<br />
Delta-approved fees the previous dentists had and we’ve tried<br />
to make increases every year based on our ZIP code as time<br />
went on. Maybe I should take a closer look at my fee schedule<br />
before I get too much farther into this to see if my fees are<br />
in the right place and make sure that when I’m operating<br />
at the sweet spot, I am making the net profit per hour that I<br />
deserve.<br />
PH: I’d contact Ken at <strong>Dental</strong> Practice Advisors. For<br />
years I did the fees and analysis, but they are far quicker<br />
at it and more complete. What they’ll have you do<br />
is submit two or three of the large cases you’ve done,<br />
your fee schedule and your profit and loss<br />
statement. And they’ll look at it comprehensively.<br />
They’ll look at how much money<br />
you need to live; that’s where they’ll start. How<br />
many days do you want to work? How much<br />
money do you need to live? This will create the<br />
profit per hour that you need to make. Then<br />
they’ll look at your practice overhead and your<br />
fee schedule. They’ll adjust your individual fee<br />
schedule such that the fees are balanced up<br />
to that 3-unit level. Then they’ll look at your<br />
complex-care cases to help you look at and<br />
see, what is the profit you have? And what’s<br />
amazing, when you come back from a profitability<br />
analysis or a fee analysis like that, you<br />
come back with some hard data on a piece of<br />
paper. Now you can sit down with your team<br />
and say: Listen, when we did Mrs. Smith, that<br />
case where we all pulled our hair out, we made<br />
less on a per-hour basis than when we’re just<br />
fixing individual teeth. When you can see it in<br />
black and white, Mike, that becomes a great<br />
leadership tool. It becomes more real to everyone.<br />
And now, I can sit down with my dental assistants<br />
and say: You know, you’ve been asking for a raise the last<br />
several months. See this profit point that we have right<br />
here? In order for me to give you a raise, we’re going to<br />
need to move that profit point up. A lot of that has to<br />
do with time. So let’s think together: How can we shave<br />
an hour or two off of these longer procedures without<br />
reducing quality. How can we do that? When the team is<br />
engaged – engagement means they’re thinking on their<br />
own without my direct influence – they’ll help create the<br />
solution, they’ll support the solution.<br />
MD: Sure. And now she is responsible for her own raise. The<br />
doctor says, I want to give you a raise. I think you deserve<br />
36 www.chairsidemagazine.com














