Winter 2013 In Touch - Muscular Dystrophy Association of New ...
Winter 2013 In Touch - Muscular Dystrophy Association of New ...
Winter 2013 In Touch - Muscular Dystrophy Association of New ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
For people living with neuromuscular conditions<br />
Mō te hunga whai oranga i te mānuka-uaua<br />
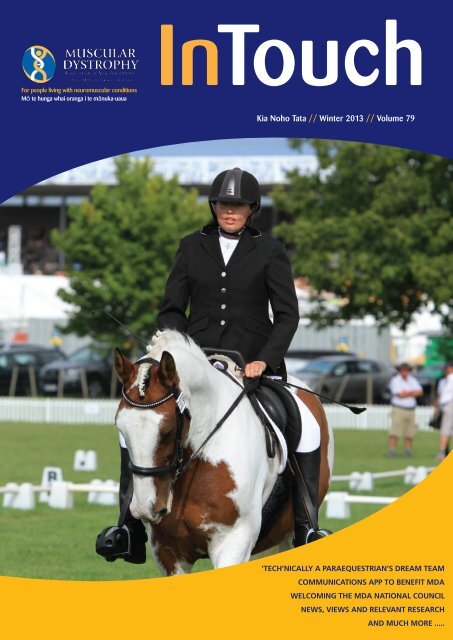
<strong>In</strong><strong>Touch</strong><br />
Kia Noho Tata // <strong>Winter</strong> <strong>2013</strong> // Volume 79<br />
‘Tech’nically a Paraequestrian’s dream team<br />
Communications App to benefit MDA<br />
Welcoming the MDA National Council<br />
<strong>New</strong>s, Views ANd Relevant REsearch<br />
IN <strong>Touch</strong> // <strong>Winter</strong> And <strong>2013</strong> Much // PAGE more 1 .....
<strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong> would like to thank the following sponsors and supporters<br />
Also thanks to the Rehabilitation Welfare Trust, CR Stead Trust, The Richdale Charitable Trust and the Douglas<br />
Charitable Trust for their continuing support.
<strong>In</strong><strong>Touch</strong><br />
Contents<br />
The Official Journal <strong>of</strong> <strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong> <strong>of</strong> NZ <strong>In</strong>c. // Kia Noho Tata // <strong>Winter</strong> <strong>2013</strong> // Volume 79<br />
PO Box 120663, Penrose,<br />
Auckland 1642, <strong>New</strong> Zealand.<br />
Freephone 0800 800 337<br />
NZ Phone: (09) 815 0247<br />
<strong>In</strong>ternational prefix (00649)<br />
Fax: (09) 815 7260<br />
Editor: Kimberley Cameron<br />
Email: kimberley@mda.org.nz<br />
Contributions:<br />
We welcome contributions, comments<br />
and letters to the editor. We thank all<br />
contributors to this edition.<br />
Deadline for next issue:<br />
Wednesday 31 July <strong>2013</strong><br />
Subscriptions: <strong>In</strong> <strong>Touch</strong> is available free to<br />
people with neuromuscular conditions,<br />
their families, health and education<br />
pr<strong>of</strong>essionals and other interested people.<br />
Advertising: <strong>In</strong> <strong>Touch</strong> welcomes<br />
advertisements concerning products<br />
and services <strong>of</strong> relevance to people with<br />
disabilities. For a rate card, please contact<br />
the editor.<br />
Printer: Converga<br />
Ph: 09 271 8420<br />
www.converga.co.nz<br />
The opinions and views expressed in this<br />
magazine are not necessarily those <strong>of</strong><br />
<strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong>.<br />
All material in this magazine is copyright.<br />
You must therefore contact the editor for<br />
permission before copying or reproducing<br />
any <strong>of</strong> it.<br />
Charities Commission Registration:<br />
CC31123<br />
ISSN 1179-2116<br />
Out and about<br />
07 Horse <strong>of</strong> the Year <strong>2013</strong> - done and dusted<br />
08 Making a difference through enabling communication<br />
09 Setting out on some Muscle Miles<br />
MDA news<br />
12 From the Chief Executive<br />
13 From the Chairperson<br />
14-17 <strong>2013</strong> MDA National Councillors in pr<strong>of</strong>ile<br />
18-19 Highlights from Bow Tie Week<br />
Your condition in review<br />
20-26 Mitochondrial myopathies in brief<br />
24-25 Living with mitochondrial myopathy<br />
- members share their own experiences<br />
Research and relevance<br />
28 Recent developments in treatment<br />
29 Behavioural management in neuromuscular conditions<br />
32 DMD clinical trials show promise<br />
<strong>In</strong> your words<br />
34 At ease - Ben Robertson<br />
35 Registry update - Miriam Rodrigues<br />
36 GenYine issue - Stacey Christie<br />
37 Legally mindful - Dr Huhana Hickey<br />
COVER IMAGE: Jodie Thorne with ‘Tech’ during their<br />
Horse <strong>of</strong> the Year winning ride.<br />
PHOTO CREDIT: R Moss <strong>of</strong> Nzequine<br />
The production <strong>of</strong> this<br />
magazine is generously<br />
supported by<br />
The Lion Foundation.
<strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong><br />
Our Mission<br />
To provide <strong>New</strong> Zealanders living with neuromuscular conditions personal support and<br />
information, and to advocate, influence and promote equality <strong>of</strong> opportunity.<br />
Our services include:<br />
•<br />
Membership <strong>of</strong> our branches and national organisation.<br />
• Specialised information about neuromuscular conditions.<br />
• <strong>In</strong>formation about disability equipment, resources<br />
and services.<br />
CHIEF EXECUTIVE<br />
Chris Higgins<br />
• <strong>In</strong> <strong>Touch</strong> magazine delivered to members four times a year.<br />
• <strong>In</strong>formative website and free 0800 phone number.<br />
• Workshops for people with neuromuscular conditions,<br />
their families, carers, medical pr<strong>of</strong>essionals and others.<br />
• Advocacy on behalf <strong>of</strong> members and their families.<br />
NATIONAL SERVICE<br />
LEADER<br />
Claudine Young<br />
ACCOUNTANT/<br />
BUSINESS MANAGER<br />
Tammy Miles<br />
• Opportunities to meet and network with other people<br />
and families affected by the same and other<br />
neuromuscular conditions.<br />
• Referrals to genetic services for genetic testing.<br />
• Support for research projects throughout <strong>New</strong> Zealand.<br />
MARKETING MANAGER<br />
Deborah Baker<br />
PROGRAMME SERVICE<br />
ADVISOR<br />
Miriam Rodrigues<br />
• Disability and medical support equipment on loan<br />
when available.<br />
• Public promotion and education about neuromuscular<br />
conditions and how they affect people’s lives.<br />
To view a list <strong>of</strong> neuromuscular conditions<br />
covered by MDA, go to page 38.<br />
Should you have a query regarding a condition<br />
not listed please contact Claudine on<br />
(09) 815 0247, 0800 800 337 or<br />
email Claudine@mda.org.nz<br />
MEMBERSHIP AND<br />
MARKETING ASSISTANT<br />
Kerry Hills<br />
ACCOUNTS<br />
ASSISTANT<br />
Olisia Sparey<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 4<br />
VOLUNTEER<br />
Kate Longmuir
from the editor<br />
I would like to begin this note by thanking all <strong>of</strong> those who have<br />
contributed to this edition and continue to engage with and enjoy<br />
this publication. It is really a pleasure to communicate with so many<br />
<strong>of</strong> you and try to bring you ideas, news and views that are <strong>of</strong> interest<br />
and personal stories that are in many cases inspirational. Secondly,<br />
however, I must apologise to those <strong>of</strong> you who suggested topics for<br />
stories or sent in content that does not appear in the following pages.<br />
Unfortunately, short <strong>of</strong> significantly increasing the size <strong>of</strong> this already<br />
lengthy publication, not all <strong>of</strong> your contributions could be fitted nor<br />
potential suggestions followed - but we’ll do our best to include them<br />
in editions later in the year. Thank you so much for your efforts.<br />
Following the MDA AGM in Christchurch in April and the election<br />
<strong>of</strong> new and re-election <strong>of</strong> incumbent members <strong>of</strong> the <strong>Association</strong>’s<br />
National Council, we include in this edition brief introductions to<br />
these elected members <strong>of</strong> the MDAs governing body. Also included<br />
are pr<strong>of</strong>iles <strong>of</strong> our Young (Rangatahi) Representative and our<br />
regional Branch Representatives. Each <strong>of</strong> these individuals are highly<br />
committed to the MDA’s development and success and would also<br />
welcome contact from our members about what can be done to<br />
assist you in your areas.<br />
Excitingly in this edition we also announce the intentions <strong>of</strong>, MDA<br />
Patron and dedicated supporter, Dame Susan Devoy to re-walk the<br />
length <strong>of</strong> <strong>New</strong> Zealand for the MDA (page 9) - watch this space<br />
for more details later in the year - and outline some information,<br />
relevant research and personal stories <strong>of</strong> our members who live<br />
with mitochondrial myopathies (pages 20-26). Also included is a<br />
summary <strong>of</strong>, neurological and neuromuscular disorder expert,<br />
Lawrence Stern’s presentation at the MDA AGM in Christchurch<br />
recently (page 28). His presentation detailed exciting new<br />
developments in the treatment <strong>of</strong> neuromuscular conditions and<br />
may be <strong>of</strong> particular interest to many <strong>of</strong> our readers.<br />
Kimberley Cameron<br />
kimberley@mda.org.nz<br />
<strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong> would also like to acknowledge its formal partners:
“<br />
Take time to discover the <strong>In</strong>vacare ®<br />
Storm ® 4 X-plore“<br />
Simply the best fit - for all terrains!<br />
With the new <strong>In</strong>vacare Storm4 X-plore power wheelchair, the demanding user<br />
can enjoy all the benefits <strong>of</strong> Storm4, combined with a four-wheel-suspension for<br />
enhanced outdoor performance, increased shock absorption / comfort and better<br />
traction on uneven ground. The G-Trac option is also available for the ulimate<br />
driving performance. The new Storm4 X-plore <strong>of</strong>fers the same advantages as the<br />
Storm4 in terms <strong>of</strong> configurability, adaptability and functionality. The stylish look <strong>of</strong><br />
Storm4 has been conserved, with its modularity, flexible seat concept and the troublefree<br />
servicing.<br />
To book a trial or to find out more call our<br />
Customer Care Team on 0800 468 222.<br />
0800 INVACARE | www.invacare.co.nz
Horse <strong>of</strong> the Year <strong>2013</strong><br />
- done and dusted!<br />
Jodie Thorne and, her horse, Tech have<br />
developed a special bond.<br />
Para-equestrian hopeful, Jodie Thorne, has once again outdone “We rode a 65% test which I was pleased with. Tech felt more<br />
herself with her competing this year so far, winning the trust<br />
active and responsive than the day before so I was pleased our score<br />
and commitment <strong>of</strong> her spirited horse, Tech, and the Grade One reflected that.”<br />
Para-Equestrian Dressage Championship at the Horse <strong>of</strong> the Year<br />
“While it was me and Tech in the arena during competitions, our<br />
competition in March.<br />
win was a credit to the fantastic team that supports us. This is truly a<br />
Horse <strong>of</strong> the Year is Jodie’s favourite show. She says she was team sport and Tech and I couldn’t do what we do without them.”<br />
nervous and sore on arrival at the show grounds – having driven for During Sunday’s musical freestyle test, Jodie says her team came<br />
five hours to the event - but she felt excited about competing with into their own as things did not begin all that well. They went on to<br />
some <strong>of</strong> <strong>New</strong> Zealand’s top riders.<br />
ride a good musical freestyle test but, Jodie says, she could not have<br />
“Tech and I had been working really hard and I wanted to end our done so without the trust <strong>of</strong> her great boy, Tech, and the commitment<br />
season with a bang.”<br />
and care <strong>of</strong> her support crew.<br />
She was happy about how her horse settled into the grounds – he’d “Just as I was finishing my warm-up ready to start my test, a<br />
only had the shavings down in his pen for 20 minutes and he was helicopter appeared from nowhere and was hovering right above our<br />
led down snoozing and, over the next few days, despite a couple <strong>of</strong> heads taking photos. It felt like they could reach out and touch my<br />
settling in issues, he really proved his mettle.<br />
head they were so low!“<br />
“We competed at the polo grounds this year which was a first<br />
She says poor Tech had no idea what was going on and she could<br />
for us. Unfortunately the route to the polo grounds went right past feel him shaking.<br />
one <strong>of</strong> the show jumping arenas, which Tech thought was incredibly “He was genuinely scared (and I was rather worried too if I’m<br />
exciting! He gave Becky a nice little sideways trot past the arenas and honest!). At the same time, the carriage drivers started warming up<br />
was a bit worked up when she arrived at the para-equestrian warm nearby which added lots <strong>of</strong> scary sights and sounds to the mix, which<br />
up area. Needless to say she had to give him a good warm in to settle Tech found overwhelming. He started jig-jogging and flung his head<br />
him down enough for me which resulted in him not being as active as up in the air, which threw me forward, onto his neck. Poor Becky<br />
Chris Mitchell and, his wife, Susan (also a runner) rest outside their camper ahead <strong>of</strong> beginning on Chris’ mammoth challenge to run the<br />
I would have liked in our test. It’s a really fine line between having him (Tech’s trainer) was trying to hold onto a dancing Tech with one hand,<br />
length <strong>of</strong> <strong>New</strong> Zealand to raise money and awareness for the <strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong>. INSET: On a training run.<br />
calm enough for me to ride, yet active enough for us to get the good while stopping me from sliding <strong>of</strong>f with the other while Sarita, Lucy<br />
walk marks and we’re still fine-tuning that side <strong>of</strong> our system!” and Chontelle ran in to catch me. It was really bad timing, as I was<br />
The next day was Saturday and the pair rode their Championship just about to leave the warm up area to go around the arena to start<br />
test. Jodie says for this ride Tech had a lot more fuel in his tank, which my test. Thankfully the judges made the call it wasn’t safe for us to<br />
was great. She says it helped that he wasn’t as excited as the previous start our test at that point, so we rode half an hour later. I was so<br />
day because they gained access to the polo grounds via a different relieved! There was no way I would have been able to ride safely under<br />
gate, which didn’t involve passing the jumping arenas!<br />
those conditions.” They went on to ride a 66% test which, combined<br />
with their other scores, won them the Grade 1<br />
Championship.<br />
One <strong>of</strong> the highlights for Jodie was the prize<br />
giving in the main dressage oval, where the paraequestrian<br />
champions and reserve champions went<br />
on parade, Jodie says.<br />
“The atmosphere in there was amazing. It was<br />
such an honour to be riding in the ho<strong>of</strong>-prints <strong>of</strong><br />
the top dressage riders in the country. We rode<br />
around the oval twice, with crowds around the<br />
outside cheering us on. It was just such a fantastic<br />
feeling - I had the biggest smile on my face the<br />
entire time we were in there!”<br />
To keep up with Jodie’s news and follow her<br />
on her quest to make the Paralympic team for Rio<br />
2016, visit www.jodiethorne.co.nz.<br />
Jodie Thorne and, her horse, Tech show their form in the ring on show day. PHOTO CREDIT: R Moss <strong>of</strong> Nzequine<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 7
Making a difference through<br />
enabling communication<br />
As a university academic, business-person, mother <strong>of</strong> a 26 year<br />
old son with muscular dystrophy and now an MDA National Council<br />
member, Sophie Tauwehe Tamati is committed to making a difference<br />
to the lives <strong>of</strong> others. Her company’s launch in 2012 <strong>of</strong> an iphone<br />
or android mobile application (App) which won a cash prize in an<br />
international award provided Sophie with an opportunity to help even<br />
more by choosing MDA as the recipient charity <strong>of</strong> the prize money.<br />
The Hika LITE App was developed as a 21st Century languagelearning<br />
tool for those wanting to learn te reo and won the ‘Diversity’<br />
Award at the Australia-<strong>New</strong> Zealand <strong>In</strong>ternet Awards (ANZIAs)<br />
following its launch in 2012. Sophie, who is a Co-founder/Director <strong>of</strong><br />
Hika Group Ltd, and whose idea it was to develop the Hika LITE App,<br />
was thrilled at the application’s success at the ANZIA’s and equally<br />
thrilled to be able to donate the cash prize to the <strong>New</strong> Zealand MDA.<br />
The ANZIA judges agreed that the Hika Group translationcommunication<br />
products have potential to migrate to other languages<br />
and are significant for their global use and appeal. The technology that<br />
the Hika LITE application is built on means that it can be used all over<br />
the world, Sophie says. There is large scope and interest in the Hika<br />
technology internationally and she sees this as just the beginning <strong>of</strong> its<br />
potential use.<br />
“Coming out <strong>of</strong> a recession, we need to be able to communicate<br />
for humanitarian and economic reasons and the fact that this app<br />
could facilitate better communication also in developing countries,<br />
among other regions, is exciting.”<br />
About the Hika LITE application, Sophie says she feels blessed that<br />
she had come up with the idea some time ago and that Hika Group<br />
Ltd has been able to turn it into something tangible that would help<br />
others to learn te reo Māori and other languages. Another aspect <strong>of</strong><br />
this application’s development that was especially rewarding to Sophie<br />
was that it brought together both her English and Māori heritage<br />
“There are many <strong>New</strong> Zealanders who want to learn te reo Māori<br />
but find getting access to the language is a huge barrier so we created<br />
Chris Higgins with Sophie Tauwehe Tamati, during her visit to the MDA<br />
National Office when she came to discuss her family and business<br />
intentions to contribute to the MDA.<br />
Hika LITE to remove that barrier.”<br />
She is also interested in seeing what opportunities there might be<br />
for Hika Group and the MDA to work together in the future. Sophie’s<br />
son, Richard, lives with muscular dystrophy having been diagnosed<br />
when he was 20.<br />
“We have incredible respect and admiration for other families that<br />
have to cope with MD. This is the beginning for us to continue our<br />
support here and internationally for those with MD.”<br />
Further information about Hika LITE can be found at<br />
http://hikagroup.com/<br />
Use the following link to view Hika LITE and other winners <strong>of</strong> the<br />
Australia/<strong>New</strong> Zealand <strong>In</strong>ternet Awards:<br />
http://www.internetawards.org.au/index.php/winners<br />
We have room to spare and are looking for a<br />
like-minded organisation to share our space.<br />
FOR LEASE: a separate designated open-plan <strong>of</strong>fice, that can comfortably fit three<br />
workstations and a meeting table, in our recently fitted out fully accessible premises.<br />
The shared facilities also include two accessible toilets, a boardroom, a meeting room and an<br />
open plan lunchroom and kitchen which can double as a training/function room.<br />
BUILDING LOCATION: Penrose, Auckland - with good motorway access and close to public<br />
transport.<br />
For a viewing, please contact Tammy Miles, MDA’s Business Manager, at tammy@mda.org.nz<br />
or phone 09 973 2665.
Dame Susan to set out on some<br />
Muscle Miles<br />
<strong>In</strong> 1988 MDA Patron and one <strong>of</strong> its most willing supporters Dame<br />
Susan Devoy walked the length <strong>of</strong> <strong>New</strong> Zealand for the <strong>Association</strong><br />
and, in doing so, raised $500,000 for those living with neuromuscular<br />
conditions. True to form Dame Susan has pledged to repeat this<br />
endeavour this year, setting her fundraising target far higher this time<br />
– she plans once again to walk from Cape Reinga to Bluff but aims to<br />
raise for the MDA this time an amazing total <strong>of</strong> $1 million.<br />
Dame Susan will begin her fund and awareness raising walk on<br />
27 October <strong>2013</strong> in Auckland and will cover full marathon distances<br />
each day, winding through both urban and rural <strong>New</strong> Zealand.<br />
Each day Susan will be joined by a number <strong>of</strong> local celebrities and<br />
members <strong>of</strong> the public all supporting Susan on her quest to raise<br />
funds for and the pr<strong>of</strong>ile <strong>of</strong> the <strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong>.<br />
As the walk passes through each centre, events that would<br />
welcome MDA member involvement and that will be focused around<br />
engaging the local communities will be hosted. Over the coming few<br />
months the Muscle Miles team will be looking to firm up plans for<br />
each <strong>of</strong> these events and would love to hear from all those with ideas<br />
or who are interested in being involved.<br />
The Team<br />
We have a great team <strong>of</strong> passionate individuals that are helping<br />
put together this ambitious project. If you would like to be involved in<br />
Muscle Miles <strong>2013</strong> please get in touch with one <strong>of</strong> the team.<br />
Event Manager<br />
Hi everyone,<br />
My name is Hamish and I will be managing the Muscle Miles<br />
walk alongside Kelly and Stacey for <strong>2013</strong>. We have had a very busy<br />
few months with preparation for the event, which is to take place at<br />
the end <strong>of</strong> the year. We are very excited to hear from the members,<br />
branches and all those who wish to be involved and look forward to<br />
making it a memorable event on the MDA’s calender.<br />
By way <strong>of</strong> background, I spent several years running an event<br />
management company. During this time we produced, organised and<br />
ran a variety <strong>of</strong> events including: outdoor music festivals, business<br />
conferences, music video releases and contracting with various other<br />
festivals. Currently I am Managing Director for a digital agency that<br />
specialise in social media management/marketing and web/app<br />
development. I hope to use the skills I have acquired alongside our<br />
great team to create a series <strong>of</strong> exciting, unique events which can raise<br />
both awareness and funds for the <strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong>.<br />
We will be launching the website shortly, which will allow access<br />
to up to date information on how the event is looking and how you<br />
can get involved.<br />
Regards, Hamish<br />
hamish@musclemiles.org.nz<br />
TOP: During her historical walk, Dame Susan certainly carried more than<br />
her own weight. ABOVE: Presenting the cheque to the MDA in 1988.<br />
Events Facilitator<br />
Hi Guys,<br />
I come from a background that extends from recently running<br />
two successful businesses simultaneously, to event management and<br />
hospitality. My strengths lie in my communication and organisational<br />
skills and at the end <strong>of</strong> this project my aim would be to leave a<br />
portfolio <strong>of</strong> events that can be continued on an annual basis by the<br />
<strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong>, the branches and their members.<br />
I remember the original walk that Dame Susan Devoy completed<br />
25 years ago and feel very privileged to have the opportunity to be<br />
part <strong>of</strong> this wonderful fundraiser in <strong>2013</strong>.<br />
I am very excited to be working with and for the branches here<br />
in the North Island and getting to know the members, their stories<br />
and how together we can all make this 25th Anniversary and Muscle<br />
Miles a huge success.<br />
I look forward to meeting you soon! Stacey<br />
Stacey@musclemiles.org.nz<br />
Events Facilitator<br />
Hi my name is Kelly Barry.<br />
Last year I embarked on a new journey that has led me to<br />
working with the MDA today. I ran a concert in Christchurch to raise<br />
awareness around the issue <strong>of</strong> fracking. That concert made me realise<br />
a few things about myself; I have an ability to juggle many different<br />
things at once and I’m addicted to organising. I am at my best when<br />
I am giving to others and helping serve humanity. I also believe in the<br />
goodness <strong>of</strong> people and the difference we can make collectively.<br />
Even after years <strong>of</strong> organising numerous events while working full<br />
time as a business administrator, the one thing that changed for me<br />
after this event was that I knew I would not be in my current job for<br />
much longer; my heart was definitely somewhere else and so began<br />
my new journey in events. When I saw that the MDA was looking for<br />
a South Island Event facilitator I knew it was the role for me. I see this<br />
event as a wonderful opportunity to raise awareness in <strong>New</strong> Zealand<br />
about muscular dystrophy.<br />
It will be an absolute pleasure for me to be involved in this project<br />
and I feel very excited about the upcoming months. <strong>In</strong> time I hope<br />
to meet with and get to know MDA members as we work towards<br />
creating a great event.<br />
Thanks, Kelly<br />
kelly@musclemiles.org.nz
MUSCULAR DYSTROPHY ASSOCIATION<br />
OF NEW ZEALAND INC.<br />
Contact details for the <strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong>’s branches<br />
NORTHERN BRANCH<br />
Fieldworkers: Kristine <strong>New</strong>some and Darian Smith<br />
Office Manager: Denise Ganley<br />
Physical Address:<br />
Postal Address:<br />
Lion Foundation House PO Box 300429<br />
3 William Laurie Place Albany<br />
Albany North Shore City 7052<br />
North Shore City<br />
Phone: 09 415 5682 or 0800 636 787<br />
Email: support@mdn.org.nz<br />
SOUTHERN BRANCH<br />
Mary Burn<br />
Raewyn Hodgson<br />
Postal Address: Postal Address:<br />
151 Stobo Street 7 Lynas Street<br />
Grasmere Outram 9019<br />
<strong>In</strong>vercargill 9810 Phone: 03 486 2066<br />
Phone: 03 215 7781 Email: raewyn.hodgson@xtra.<br />
or 03 218 3975 co.nz<br />
WELLINGTON BRANCH<br />
Fieldworker: Dympna Mulroy<br />
Office Manager: Margaret Stoddart<br />
Physical Address:<br />
Postal Address:<br />
49 Fitzherbert Street PO Box 33037<br />
Petone<br />
Petone<br />
Lower Hutt 5012 Lower Hutt 5012<br />
Phone: 04 5896626 or 0800 886626<br />
Email: <strong>of</strong>fice.mdawgtn@xtra.co.nz<br />
CANTERBURY BRANCH<br />
Fieldworkers: Paul Graham and Donna Mason<br />
Office Manager: Eris Le Compte<br />
Physical Address:<br />
Postal Address:<br />
314 Worcester Street, PO Box 80025<br />
Linwood,<br />
Riccarton<br />
Christchurch 8247 Christchurch 8440<br />
Phone: 03 377 8010 or 0800 463 222<br />
Email: mdacanty@xtra.co.nz<br />
If you want issues brought to National Council<br />
meetings, talk to your branch representative. They have the<br />
responsibility to raise your issues at National Council meetings<br />
and to make sure you are heard. Your branch representatives<br />
and their contact details are as follows:<br />
Northern branch<br />
Trevor Jenkin<br />
Ph 021 267 4380<br />
Email Trevor.jenkin@gmail.com<br />
Wellington branch<br />
Liz Mills<br />
Ph 04 566 9557<br />
Email stuartcmills@xtra.co.nz<br />
Southern branch<br />
Raewyn Hodgson<br />
Ph 03 486 2066<br />
Email raewyn.hodgson@xtra.co.nz<br />
Canterbury branch<br />
Vivienne Palmer<br />
Ph 021 571 258<br />
Email: vivienne.palmer@clear.net.nz<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 10
LEVO OF SWITZERLAND - C3<br />
The NEW C3 combines world renowned standing functions with a unique auto<br />
adjustable traction power base.<br />
Characteristics <strong>of</strong> the Sitting and Standing unit:<br />
• Optimal biomechanics in all sitting and standing positions<br />
• Quickly and easily adaptable to any individual body size<br />
• Enables mounting for individual back and seat systems<br />
• Minimal seat height for easy transfer and table or desk accessibility<br />
• Sitting and Standing unit with a new ‘Low Shearing System’.<br />
Characteristics <strong>of</strong> the power base :<br />
• 4WD – Compact, agile, easy to operate and extremely efficient drive system<br />
• Small dimensions for use in narrow spaces<br />
• Compact design for easy transport<br />
• Reliably manages curbs, ramps and rough ground<br />
• Center wheel drive in seated position means a smaller turn radius<br />
• Front wheel drive in standing position, safer to maneuver<br />
• Turns in sitting and in standing position around the users center <strong>of</strong> gravity<br />
• Easy to service, superior accessibility, constant support.<br />
VENDLET OF DENMARK - PATIENT TURNER<br />
The founder Christian Buus, had a disabled daughter who was cared for at<br />
home. As the daughter grew older, his wife could no longer endure the physical<br />
strain <strong>of</strong> turning her daughter in bed, thus, he invented the first VENDLET<br />
almost 30 years ago.<br />
The latest model is the Vendlet V5, which provides full electric operation.<br />
Other benefits include :<br />
• Prevention <strong>of</strong> caregiver injuries<br />
• Ease <strong>of</strong> daily care routines<br />
• <strong>In</strong>creased patient comfort<br />
• Positive contact between the caregiver and patient<br />
• Improved caregiver productivity<br />
• Easy attachment to most healthcare and hospital beds<br />
AEROLET OF HOLLAND - TOILET LIFT<br />
The AEROLET Toiletlift, is suitable for those with weight bearing difficulty and is ideal for users<br />
who have Multiple Sclerosis, Motor Neurone disease, <strong>Muscular</strong> <strong>Dystrophy</strong>, strokes and other<br />
disabling conditions.<br />
With easy to use electronic controls, it gently raises and lowers, while the user remains fully seated,<br />
supported, and in control at all times ensuring safe, comfortable personal hygiene management.<br />
Ergonomically designed and <strong>of</strong>fering independence, privacy and dignity for the mobility impaired,<br />
The Toiletlift comes with arm supports, which move with the user giving constant support when<br />
sitting down and standing. It is adjustable for the height and weight <strong>of</strong> the disabled user, without<br />
any inconvenience to other toilet users.<br />
FOR MORE INFORMATION OR TO ARRANGE A TRIAL CALL US FREE ON 0800 338 877<br />
WWW.EUROMEDICAL.CO.NZ I INFO@EUROMEDICAL.CO.NZ<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 11
From the Chief Executive<br />
MDA news<br />
Greetings and kia ora koutou<br />
MDA Chief Executive,<br />
Chris Higgins<br />
The Annual General Meeting (AGM) <strong>of</strong> an incorporated society deserves to<br />
be regarded as a significant event. Typically in <strong>New</strong> Zealand incorporated<br />
societies are run throughout the year by governing boards or executive<br />
committees on behalf <strong>of</strong> and as elected by the societies’ members. The AGM<br />
provides an annual opportunity for Societies’ members themselves to directly<br />
influence policy and decision making. It is also an opportunity for them to<br />
hold their governing boards and executive committees, together with their<br />
executive staff, accountable for their stewardship <strong>of</strong> resources, past actions<br />
and future intentions.<br />
The <strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong> (MDA)’s<br />
AGM on 19th April was therefore an important<br />
event. It was an opportunity for me as Chief<br />
Executive and Helen Melrose as National<br />
Council Chairperson to be accountable to the<br />
MDA’s members through the presentation <strong>of</strong><br />
our reports, and for the National Council to<br />
demonstrate its stewardship <strong>of</strong> the <strong>Association</strong>’s<br />
resources through the presentation <strong>of</strong><br />
its audited annual accounts. These three<br />
documents collectively comprise the MDA’s<br />
2012 Annual Report which is available as a hard<br />
copy on request or through the MDA’s website.<br />
A big thank you therefore to all members who<br />
came along to the AGM, read and listened to<br />
the reports and asked questions.<br />
The AGM also confirmed those elected<br />
to serve as <strong>of</strong>fice holders and I wish to<br />
congratulate Lindsay McGregor, Heather<br />
Browning, Sophie Tamati, Gill Goodwin and<br />
Derek Woodward on their appointments<br />
and reappointments. Congratulations also to<br />
Raewyn Hodgson, Vivienne Palmer, Liz Mills<br />
and Trevor Jenkin who have been appointed by<br />
their Branch executive committees as National<br />
Council Branch representatives. I look forward<br />
to working with you all, together with other<br />
members Stacey Christie, Roger Loveless and<br />
Andrea McMillan.<br />
<strong>In</strong> his first <strong>In</strong> <strong>Touch</strong> column as Chairperson<br />
Lindsay has commented on the importance <strong>of</strong><br />
the MDA’s fieldworker service and that it should<br />
be funded by government as a core service,<br />
rather than by the MDA. The MDA’s equivalent<br />
UK organisation, the <strong>Muscular</strong> <strong>Dystrophy</strong><br />
Campaign (MDC), has been successful in having<br />
its MDC funded fieldwork service funded by the<br />
UK health service, and we hope to emulate this<br />
here in <strong>New</strong> Zealand.<br />
However it is likely to be very challenging<br />
in the current fiscally tight environment where<br />
the government is reluctant to spend money<br />
on new initiatives, and where any discretionary<br />
funds tagged for disability support services are<br />
being allocated to the Ministry <strong>of</strong> Health’s new<br />
model for supporting people with disabilities.<br />
This notably includes the development <strong>of</strong><br />
“local area coordination” (LAC) services<br />
which are being piloted in the Bay <strong>of</strong> Plenty.<br />
Furthermore, the government funding that we<br />
currently receive to support the provision <strong>of</strong><br />
information services appears to be regarded as<br />
“discretionary” and is therefore at risk.<br />
The proposed LAC service bears a<br />
resemblance to the MDA’s fieldworker services<br />
in that it is intended to:<br />
• promote positive values towards, and<br />
expectations <strong>of</strong>, disabled people, and focus on<br />
the question “what’s a good life for you?”;<br />
• help disabled people and their<br />
families and whānau to explore how to live a<br />
good life through <strong>of</strong>fering general information<br />
and someone to talk to about living with a<br />
disability;<br />
• provide access to tailored information<br />
and may facilitate access to small amounts <strong>of</strong><br />
funding to address immediate issues;<br />
• help disabled people to build a<br />
community <strong>of</strong> support through, for example,<br />
making connections with natural supports and<br />
the local community; and<br />
• support communities to be inclusive<br />
and help people to access government services<br />
(including specialised disability supports)<br />
However, what the LAC service will not be<br />
able to do is provide specialist knowledge <strong>of</strong><br />
neuromuscular conditions either to people living<br />
with these conditions or their health and other<br />
support pr<strong>of</strong>essionals. We believe that this is<br />
crucial to ensuring that MDA members and<br />
others with a condition can “live a good life” and<br />
that its absence from the LAC model means that<br />
it is fundamentally flawed. We further believe<br />
that funds allocated to support LAC would be<br />
used much more effectively if they were instead<br />
allocated to the MDA’s (and other disability<br />
support organisations’) fieldwork services, which<br />
already have a proven track record in providing<br />
LAC type services. <strong>In</strong> other words why reinvent<br />
the wheel?<br />
Our challenge is to convince the health<br />
bosses and policy makers, together with<br />
those evaluating the Bay <strong>of</strong> Plenty pilot, <strong>of</strong> the<br />
merits <strong>of</strong> our case. We intend to make this a<br />
priority over the next few months. Any MDA<br />
members or readers who have comments as<br />
to how we might get maximum traction with<br />
this important issue are welcome to contact<br />
me. A more detailed paper on this issue was<br />
considered by the National Council at its<br />
February <strong>2013</strong> meeting and is available to MDA<br />
members on request or by visiting the members<br />
only section <strong>of</strong> the MDA website.<br />
E noho ra<br />
Chris Higgins<br />
Chief Executive<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 12
From the Chairperson<br />
MDA news<br />
Hi Everyone.<br />
At the recent Annual General Meeting in Christchurch I took over as<br />
Chairperson from Helen Melrose.<br />
I have been on the National Council for around fifteen years initially as<br />
Treasurer and more recently as Vice-Chairperson. I am really looking<br />
forward to taking on this new challenge and I trust that I can help to<br />
continue to develop our organisation.<br />
MDA Chairperson,<br />
Lindsay McGregor<br />
I would firstly like to sincerely thank Helen<br />
for her four years as Chairperson. Helen took<br />
on the role just as we were coming through<br />
a very difficult time and she has worked very<br />
hard to re-build MDA into what is now a very<br />
stable organisation providing many services to<br />
our members.<br />
At the AGM we welcomed two new people<br />
who are joining the National Council, Gill<br />
Goodwin and Sophie Tamati. It’s great to have<br />
new people and I know both Gill and Sophie<br />
will bring plenty <strong>of</strong> enthusiasm and skills to<br />
their roles.<br />
The existing National Council members<br />
who are continuing are Heather Browning<br />
(Vice-Chairperson), Roger Loveless, Derek<br />
Woodward, Andrea McMillan and Stacey<br />
Christie (Young (Rangatahi) Representative).<br />
We also have our Branch Representatives,<br />
Raewyn Hodgson (Southern Regions),<br />
Vivienne Palmer (Canterbury), Liz Mills<br />
(Wellington) and Trevor Jenkin (Northern).<br />
Branch Representatives are appointed by their<br />
respective Branches and will be confirmed<br />
following their Annual General Meeting’s.<br />
Following the AGM we enjoyed<br />
presentations from three guest speakers, Dr.<br />
Larry Stern (Pr<strong>of</strong>essor <strong>of</strong> Neurology, University<br />
<strong>of</strong> Arizona), Hannah Kirsten (PhD student<br />
and recipient <strong>of</strong> the inaugural Neuromuscular<br />
Research Foundation Trust scholarship)<br />
and Bridget Williams (Canterbury Student<br />
Volunteer Army).<br />
Larry’s presentation highlighted the very<br />
exciting advances in treatments for some<br />
conditions. (More details can be found in the<br />
Research and Relevance section <strong>of</strong> this edition).<br />
Hannah gave us some details <strong>of</strong> her work<br />
into myotonic dystrophy which reinforced<br />
the benefits <strong>of</strong> being able to provide funding<br />
through our Research Trust.<br />
Lastly Bridget gave a very enthusiastic<br />
presentation <strong>of</strong> the work <strong>of</strong> the Student<br />
Army in Christchurch formed following the<br />
earthquake. They are keen to assist us and<br />
I am sure the Canterbury Branch will take<br />
advantage <strong>of</strong> this.<br />
At the Council meeting the following day,<br />
I asked everyone to introduce themselves and<br />
to tell us some personal background including<br />
life and work experience, what motivates<br />
them to give up their valuable personal time<br />
to serve on the National Council, and what<br />
skills and attributes they can <strong>of</strong>fer to our<br />
functioning and effectiveness.<br />
Everyone was very open about themselves<br />
and members can be confident that the new<br />
National Council is a group <strong>of</strong> very dedicated<br />
and passionate people who have a wide range<br />
<strong>of</strong> skills and experiences to continue to develop<br />
the MDA.<br />
Last year the 2020 Vision Strategic Plan<br />
was developed after receiving extensive<br />
feedback from members. The key priorities for<br />
the next three years are <strong>In</strong>come generation,<br />
campaigning, empowerment, reach and<br />
business excellence.<br />
The Annual Operating Plan for this year<br />
includes work in each <strong>of</strong> these areas but a key<br />
focus is continuing to develop our income base.<br />
It is clear that our current methods <strong>of</strong> funding<br />
are under pressure, particularly telemarketing<br />
and grants. Last year we generated similar<br />
income to the previous year from telemarketing<br />
but at a higher cost.<br />
We have now implemented closer liaison<br />
with our telemarketing provider and it is<br />
pleasing to see that for the first quarter <strong>of</strong> this<br />
year we are “back on track.”<br />
We have also appointed a new Grants<br />
Coordinator to replace the organisation we<br />
used last year in order to provide a better<br />
management <strong>of</strong> this important function.<br />
However, the Council are keen to move<br />
away from our reliance on telemarketing<br />
income. We believe that it is unreasonable<br />
for us to provide our own funding for the<br />
fieldworker service which we know is very<br />
important to members. <strong>In</strong> a fully inclusive<br />
society everyone is entitled to appropriate<br />
access to health services and this should<br />
be core government policy. So we will<br />
put considerable effort into lobbying for<br />
government funding for the fieldworker service<br />
to ensure our members needs are met and free<br />
up our own funding for other services.<br />
As I said earlier, I am excited (but with some<br />
trepidation) to take on the role <strong>of</strong> Chairperson<br />
and will do my best to ensure we have a strong<br />
and valuable organisation for our members.<br />
Best wishes<br />
Lindsay McGregor<br />
Chairperson<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 13
MDA Chairperson<br />
Lindsay McGregor<br />
I live in Howick, Auckland, with my wife Sheryl, and I have two<br />
adult children; Sarah who lives in Melbourne with her husband and a<br />
10 month old boy, Marlon; and Cameron who currently lives with us<br />
with his partner – they are both heading <strong>of</strong>f for an extended OE in a<br />
couple <strong>of</strong> months.<br />
I have Becker’s muscular dystrophy which was diagnosed when<br />
I was 18. I was walking until four years ago and am using a manual<br />
chair but am transitioning to a powerchair.<br />
I trained as a Chartered Accountant and have worked for a variety<br />
<strong>of</strong> accounting and commercial businesses since leaving school in<br />
1971. I currently work for Weston Milling (one <strong>of</strong> two large flour<br />
manufacturers in <strong>New</strong> Zealand) where I was Financial Controller for<br />
10 years before being appointed CEO in 2008.<br />
I have recently semi-retired, but am still with Weston Milling doing<br />
financial and systems project work mainly for our Australian business.<br />
I love travelling having done my OE in the late 70’s – six months<br />
in a Combi van in Europe, followed by a year working in London<br />
and then travel through Scandinavia and Eastern Europe including<br />
in Russia, before returning home through Asia. I have also been<br />
fortunate to have travelled extensively for business, mainly Australia<br />
but also the USA, and Asia.<br />
My interest in sailing has led to competing at regattas in <strong>New</strong><br />
Zealand and also Adelaide, Nova Scotia (Canada) and last year in<br />
the Access Class World Champs in Sydney. A member <strong>of</strong> Sailability<br />
Auckland for eight years – we aim to get on the water every week<br />
right through the year.<br />
I also enjoy gliding; the Auckland Gliding Club have recently set-up<br />
a glider with hand-controls and have a people hoist. I have had one<br />
flight and will be doing more.<br />
I have been on the MDA National Council since 1997. I was<br />
Treasurer for 10 years and then Vice-Chairperson before taking over<br />
as Chairperson at our AGM in April.<br />
I believe that all disabled people should have the same access to<br />
education, health-care, work and social opportunites as non-disabled<br />
people and not be marginalised as <strong>of</strong>ten happens.<br />
It is and should continue to be a significant focus <strong>of</strong> MDA to<br />
lobby government and other agencies to continue to improve our<br />
opportunities.<br />
A key focus <strong>of</strong> MDA through each branch is providing the fieldworker<br />
service. This is very expensive and relies mainly on charitable<br />
grants which each Branch works hard to continue to obtain. I believe<br />
this service should be provided by DHB’s and the MDA will continue<br />
to push for this.<br />
MDA Vice Chairperson<br />
Heather Browning<br />
I am the General Manager <strong>of</strong> Enable <strong>New</strong> Zealand, one <strong>of</strong> the<br />
largest disability support providers in <strong>New</strong> Zealand. I have a wide<br />
understanding <strong>of</strong> the disability sector and a long association with<br />
disability support services, both as a funder and provider, through<br />
which I have developed a depth and breadth <strong>of</strong> knowledge, insight<br />
and experience. I originally trained as a physiotherapist, and over<br />
the past 20 years in <strong>New</strong> Zealand I have worked with the <strong>Muscular</strong><br />
<strong>Dystrophy</strong> <strong>Association</strong> - as a physiotherapist, then as the Director and<br />
then in policy and contracting settings with both the former Health<br />
Funding Authority and the Ministry <strong>of</strong> Health and now with Enable<br />
<strong>New</strong> Zealand. My background gives me a sound understanding <strong>of</strong><br />
the drivers for the disability sector and the need to deliver quality and<br />
accessible services to disabled people.<br />
I have been a National Council member for four years and have<br />
a strong commitment to ensuring the MDA can move forward and<br />
continue to diversify. We have the opportunity to grow and develop<br />
as we respond to members needs for support in the ever changing<br />
environment <strong>of</strong> the disability sector.<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 14
Gill Goodwin<br />
I am excited by the opportunity to serve on the National Council<br />
<strong>of</strong> the MDA. I am currently a partner in the law firm <strong>of</strong> Burke<br />
Melrose, which specialises in elder law. I have advised boards <strong>of</strong><br />
directors on governance, directors’ duties and compliance issues<br />
(including in connection with privacy<br />
and discrimination issues). I am also on<br />
the panel <strong>of</strong> the Human Rights Review<br />
Tribunal.<br />
Gill Goodwin<br />
Roger Loveless<br />
Since my election to Council in 2008, the MDA has identified<br />
that some 4000 people in <strong>New</strong> Zealand suffer from a neuromuscular<br />
condition, yet our membership only touches about 25% <strong>of</strong> these<br />
people. I see providing the best possible support to all <strong>of</strong> these<br />
people as the <strong>Association</strong>’s core mission. The present government<br />
pr<strong>of</strong>esses to support all people with disabilities both effectively<br />
and efficiently so that sufferers are both valued in society and can<br />
achieve their full potential. The challenge for the <strong>Association</strong> is to<br />
build partnerships with government and other health service nongovernment<br />
organisations to make this happen. <br />
I joined the <strong>Association</strong> shortly after being diagnosed with<br />
Becker MD in 1990. This will be my sixth year on Council. While<br />
2009 marked the end <strong>of</strong> my career as a pr<strong>of</strong>essional electric<br />
power engineer, the last 12 years as managing director <strong>of</strong> a small<br />
engineering consultancy I founded, I still remain active in the<br />
community as an Access Coordinator for CCS Disability Action<br />
Waikato, placing the needs to remove barriers to full participation<br />
Sophie Tauwehe Tamati<br />
I am the inventor <strong>of</strong> the Hika Rapid Language Learning System<br />
and Co-founder/Director <strong>of</strong> Hika Group Ltd.<br />
With tribal affiliations that include Waikato, Ngāti Maniapoto,<br />
Ngāi Tuhoe and Ngāti Tuwharetoa, I also acknowledge my English,<br />
Irish and French settler ancestry.<br />
As a Senior Lecturer at The University <strong>of</strong> Auckland, Faculty <strong>of</strong><br />
Education in the School <strong>of</strong> Te Puna Wānanga, I have lectured in the<br />
Māori medium pathway since 1998 and held a range <strong>of</strong> positions<br />
<strong>of</strong> responsibility in the Education Sector including that <strong>of</strong> Primary<br />
School Principal and Ministry <strong>of</strong> Education Consultant delivering<br />
Māori language pr<strong>of</strong>essional development programmes to Māori<br />
medium teachers.<br />
Among my qualifications, I hold a Bachelor <strong>of</strong> Education,<br />
Postgraduate Diploma in <strong>In</strong>terpreting and Translating Māori and<br />
a Master <strong>of</strong> Education degree from The University <strong>of</strong> Auckland. I<br />
am presently completing my PhD at The University <strong>of</strong> Auckland in<br />
by the disabled community in front<br />
<strong>of</strong> society and more specifically local,<br />
regional and national government. <strong>In</strong><br />
this role we recently won some funding<br />
from the Ministry <strong>of</strong> Social Development<br />
Making a Difference fund to develop<br />
a recognised and statistically robust<br />
methodology to measure the numbers<br />
Roger Loveless<br />
<strong>of</strong> disabled people in the community,<br />
which can be compared with expected<br />
numbers to determine levels <strong>of</strong> exclusion. Hamilton also has an<br />
advisory group known as the Council <strong>of</strong> Elders comprising those over<br />
60, <strong>of</strong> which I was elected vice chairman in December 2012.<br />
I am married to Mary, have two grown up, and happily married<br />
sons, two grandchildren in the UK, and two in Rotorua. I really<br />
appreciate the support <strong>of</strong> the MDA, and would encourage all people<br />
with a neuromuscular condition to play an active, if not physical, role<br />
in society within, and occasionally outside, their comfort zone!<br />
Education and Applied Linguistics with<br />
my research strengths including Māori<br />
Medium Education; Applied Linguistics;<br />
Second Language Acquisition and<br />
Bilingual Education.<br />
As a wife, mother and grandmother,<br />
I have focused my efforts on ensuring<br />
that te reo Māori is passed on as a Sophie Tauwehe Tamati<br />
linguistic legacy to my children and<br />
mokopuna (grandchildren). As an inventor and Māori entrepreneur<br />
in the technology ecosystem, I have been influential in creating<br />
a technology that other indigenous peoples can use to save their<br />
languages. As a pr<strong>of</strong>essional, I am well educated and articulate in<br />
both Māori and English. And finally as a Māori woman, I hope that<br />
my story will inspire other Māori women to be role models, leaders<br />
and visionaries for the next generations.<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 15
Andrea McMillian<br />
I grew up near Greymouth on the West Coast, and have lived in<br />
Gore for the past 20 years. I have worked as a Practice Nurse for 21<br />
years and have three children, Ben (14), Olivia (13) and Zac (11). My<br />
eldest was diagnosed with Friedreich ataxia when he was age 11.<br />
My interests and goals are ensuring that people with health<br />
challenges are put in touch with the services required to help/<br />
support their condition, ie removing and/or addressing the barriers<br />
at grass roots level.<br />
Having a child with a disability and also working in the health<br />
sector gives you a view on both sides<br />
<strong>of</strong> the fence. I have experienced the<br />
frustration <strong>of</strong> how simple things can<br />
be made harder, unnecessarily.<br />
I think it’s important for health<br />
providers to be aware <strong>of</strong> what the<br />
barriers are, as <strong>of</strong>ten they don’t.<br />
The above challenges are highlighted<br />
more so in rural areas.<br />
Andrea McMillan<br />
Derek Woodward<br />
I am 66 yrs old and am married to Claire for 45yrs this October.<br />
I have two sons, both living in Brisbane. Craig (39) is a geologist<br />
who is doing research in the field <strong>of</strong> limno paleology, he also<br />
enjoys his lecturing, and Mark (41) who is an assistant manager in<br />
a large electronics store. He is also a computer whiz and regularly<br />
saves me or my computer from a meltdown whilst he is sitting in<br />
his study in Brisbane.<br />
I, like all <strong>of</strong> my siblings, have PROMM, which is a form <strong>of</strong> myotonic<br />
muscular dystrophy<br />
My work history has largely involved sales in the photographic<br />
industry. I have been a part owner <strong>of</strong> three photographic shops in<br />
Dunedin and a bookshop, Postshop and Lotto shop in Christchurch.<br />
I also spent 25 Years as a volunteer ambulance <strong>of</strong>ficer and head <strong>of</strong><br />
the Mosgiel division <strong>of</strong> St John, until my disability brought that to an<br />
end.<br />
I have, all <strong>of</strong> my life had a desire to help others in the community,<br />
as in my ambulance service. I also spent five years training those who<br />
had not achieved well in schools, or those who had lost their job, with<br />
Trevor Jenkin<br />
Northern Branch representative<br />
My name is Trevor Jenkin, I am the father <strong>of</strong> a 14 year old boy with<br />
Duchenne muscular dystrophy, I am married to Joy and we own our<br />
own successful business.<br />
We as a family have been associated with the <strong>Muscular</strong> <strong>Dystrophy</strong><br />
<strong>Association</strong> for the past 12 years and with <strong>Muscular</strong> <strong>Dystrophy</strong><br />
Northern since its formation.<br />
I was elected to the position <strong>of</strong> Vice Chairperson <strong>of</strong> MDN in 2011<br />
and again in 2012, and at the recent MDN AGM on the 28th April<br />
<strong>2013</strong> was elected Chairperson and Northern Branch rep on the<br />
National Coucil. I am also the President <strong>of</strong> the Auckland Powerchair<br />
Football Club which promotes and runs powerchair football games<br />
in the Auckland area. I have been very active within MDN helping<br />
organise and attending family camps, Christmas parties and many<br />
other events, as well as the normal committee stuff. This gives me the<br />
opportunity to get out there and meet other members, talk to them<br />
and understand their views and expectations <strong>of</strong> MDN. I also like to be<br />
actively involved in supporting MDN’s many sponsors and funders in<br />
their events to show we as a membership do appreciate all they do for<br />
the necessary skill to succeed in a sales<br />
career. I also taught older school children<br />
who had some learning difficulties<br />
I am motivated to serve on the<br />
National Council, and on my area<br />
committee to put something back<br />
into the organisation that has not only<br />
assisted me, but many others in the Derek Woodward<br />
community. I have served on the National Council now for just over<br />
a year.<br />
I feel that the skills that were derived from many years <strong>of</strong> owning<br />
and operating several Businesses, also translate to making me an<br />
excellent Council member. I am a good people person and I feel I am a<br />
creative thinker and a good family man with a lively sense <strong>of</strong> humour.<br />
I have actively contributed to the team <strong>of</strong> people that comprises<br />
the National Council and I will continue to do so, to ensure MDA<br />
is financially strong, and continues to grow, so it is still able to<br />
<strong>of</strong>fer support to as many in the community as possible that have a<br />
neuromuscular condition.<br />
us. I also get around to as many expos<br />
and other disability sector events as I can<br />
to show a presence as I think awareness<br />
is another important part.<br />
I wish to continue to do all <strong>of</strong><br />
the above now as Chairperson and<br />
encourage any members to contact me<br />
if they want to get a message to the<br />
Trevor Jenkin<br />
committee or even to our National Council. I am only too happy<br />
to help and please if there is something we are not doing right tell<br />
me, I need to know so we can at least try and put it right. <strong>In</strong> saying<br />
that I also like to hear things we are doing or have done right from<br />
our members.<br />
Within the next year I will be trying to get around and meet as<br />
many members as possible so if you know <strong>of</strong> an event that a few<br />
members will be at please let me know or let our Office Manager<br />
Denise Ganley know so I can attempt to be there.<br />
All the very best to you all lets make <strong>2013</strong>/14 a great year for MDN.<br />
Below are my contacts, please use them.<br />
Trevor.jenkin@gmail.com<br />
PH/TEXT: 021 267 4380<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 16
Stacey Christie<br />
As you probably know by now, my name is Stacey Christie and<br />
I am your Young (Rangatahi) Representative. It is such an honour<br />
to be able to represent the younger members <strong>of</strong> the <strong>Muscular</strong><br />
<strong>Dystrophy</strong> <strong>Association</strong>.<br />
It is my hope to connect with MDA’s youth and engage them with<br />
the <strong>Association</strong> and with each other. I am living in Wellington while I<br />
attend university, studying fashion design. Myself and another young<br />
MDA member are currently organising a youth meet up for members<br />
under 30 in Wellington, so we can connect with each other. So get in<br />
Raewyn Hodgson<br />
Southern Regions Branch representative<br />
I am the mother <strong>of</strong> two adult children, a daughter, Lisa, and a<br />
son, Rhys. Rhys is now aged twenty nine and has Duchenne muscular<br />
dystrophy. My husband and I are his main caregivers.<br />
I have been a registered nurse for thirty five years and currently<br />
work part-time in the cardiology department at Dunedin Hospital.<br />
I have been involved with the <strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong> for<br />
twenty years and am a life member <strong>of</strong> the Southern Region Branch. I<br />
was a branch representative for a number <strong>of</strong> years during the 1990s.<br />
contact with me if you’d like to be a<br />
part <strong>of</strong> it!<br />
Over the last few years I have<br />
really enjoyed talking to members<br />
and meeting up with many <strong>of</strong> you,<br />
so continue to introduce yourselves.<br />
I write an article in each issue <strong>of</strong> <strong>In</strong><br />
<strong>Touch</strong>, so you can keep up to date<br />
Stacey Christie<br />
with what’s going on with me and find my contact details in there.<br />
Again, thank you for this opportunity to represent you, and feel<br />
free to email me at shchristie@live.com or add me on Facebook.<br />
I have been the Branch Representative<br />
for the National Council, for the<br />
Southern Region Branch since June<br />
2009. I look forward to the challenge<br />
<strong>of</strong> representing the Southern Region<br />
Branch at the National Council meetings.<br />
I believe I have the skills and broad<br />
knowledge base and experience to<br />
Raewyn Hodgson<br />
provide effective communication/consultation and liaison between<br />
the Southern Region Branch members, the National Council, other<br />
branches and the national <strong>of</strong>fice.<br />
Liz Mills<br />
Wellington Branch representative<br />
Since November 2008 I have been the Chairperson and Branch<br />
Rep <strong>of</strong> MDAW. I have been married to Stu for 23 years and we have<br />
two daughters – Hannah (21) and Georgia. (18). We live in Lower<br />
Hutt. I was diagnosed in 1982 with Friedreichs Ataxia and am now<br />
fully wheelchair dependent. I am fortunate to have always been<br />
surrounded by family and friends who have always given me lots <strong>of</strong><br />
support and encouragement and have<br />
got me through the last 31 years. I am<br />
actively involved at branch level and<br />
on the National Council because I am<br />
passionate about the great things MDA<br />
are doing for its members and want to<br />
play a role to see this continue.<br />
Liz Mills<br />
Vivienne Palmer<br />
Canterbury Branch representative<br />
I am the branch representative for MDA Canterbury and have<br />
been on the MDA Canterbury committee for 12 years. <strong>In</strong> my earlier<br />
years I married a farmer with whom I have four children - two boys<br />
and two girls.<br />
The three youngest were having physical difficulties, as<br />
compared to their peers at school, and all three were subsequently<br />
diagnosed with limb girdle muscular dystrophy (LGMD).<br />
I attended the Christchurch Polytechnic <strong>In</strong>stitute <strong>of</strong> Technology<br />
and achieved a Bachelor <strong>of</strong> Nursing Degree in 1997 and have<br />
practiced full time nursing since. I feel that this has further enabled<br />
me to support and advocate for my family.<br />
As a family we have always tried to live as normal a life as<br />
possible but, were always very pleased to receive help and resources<br />
from the MDA and community health<br />
pr<strong>of</strong>essionals. We feel very privileged<br />
to have been part <strong>of</strong> the MDA<br />
community and a supportive health<br />
system.<br />
My busy working and family<br />
life caused me to delay elected<br />
commitment until the recent<br />
Vivienne Palmer<br />
opportunity <strong>of</strong> being a Branch<br />
Representative which is now fulfilling<br />
my aspiration to give back to the<br />
MDA and MDA Canterbury. I am enjoying the contact with the<br />
<strong>Association</strong> and working with dedicated and fabulous people. The<br />
opportunity is also further enhancing my life experience.<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 17
MDA news<br />
Community Forums<br />
PHARMAC is seeking feedback on the<br />
criteria it uses to make decisions about which<br />
pharmaceuticals to make available.<br />
On the pharmac website http://www.<br />
pharmac.health.nz you can find out about<br />
how you can have your say on the decision<br />
criteria consultation, and be part <strong>of</strong> the<br />
Community Forums during June and July<br />
<strong>2013</strong>.<br />
MDA is keen to see Pharmac extend its<br />
decision criteria to include pharmaceuticals<br />
for rare disorders, like neuromuscular<br />
conditions, given that people with a rare<br />
disorder have <strong>of</strong>ten experienced long<br />
term disability and disadvantage prior to<br />
treatment.<br />
Please contact the MDA or visit the<br />
MDA website if you would like to take a<br />
copy <strong>of</strong> the 1 page summary <strong>of</strong> MDA’s view<br />
<strong>of</strong> what Pharmac’s decision criteria should<br />
look like so that people with neuromuscular<br />
conditions get a fairer go.<br />
Community consultation dates:<br />
Whangarei - Toll Stadium,<br />
13th August 10-12.30pm<br />
Auckland Central - Mt Albert War Memorial<br />
Hall, 25th June 10.45-1pm<br />
Auckland South - Wiri Community Hall,<br />
25th June 2.15-4.30pm<br />
Hamilton - Chartwell Cooperating Church<br />
Hall, 28th June 1-3.30pm<br />
Tauranga - Greerton Community Hall,<br />
9th August 1.30-4pm<br />
<strong>New</strong> Plymouth - Citizens Advice Bureau,<br />
1st July 1.30-4pm<br />
Wellington - Pataka Art + Museum Porirua,<br />
3rd July 1-3.30pm<br />
Hokitika - All Saints Church Hall,<br />
12th July 1-3.30pm<br />
Christchurch - Canterbury Horticultural<br />
Society, 9th July 10-12.30pm<br />
Dunedin - Otago Museum,<br />
31st July 1-3.30pm<br />
Bow tie week <strong>2013</strong><br />
The MDA was proud to once again be supported by<br />
Judy Bailey for our annual awareness campaign, bow<br />
tie week (16-24 March). Judy appeared alongside<br />
MDA member, nine year old Nicholas Brockelbank,<br />
who has Duchenne muscular dystrophy. Judy was<br />
also the voice <strong>of</strong> the national radio and appeared on the print campaign<br />
which brought greater awareness to neuromuscular conditions.<br />
The MDA uses the image <strong>of</strong> a bow tie to demonstrate the difficulties<br />
our members can face doing many everyday tasks. The exclusively<br />
designed bow tie pins were available in WORLD stores, and ASB<br />
branches nationwide for a gold coin donation.<br />
A special thank you to all the amazing members and supporters<br />
nationwide that collected for the branches and made the <strong>2013</strong><br />
campaign happen.<br />
Wellington Branch organises Bow Tie Design Competition<br />
The year 8 students from Samuel<br />
Marsden Collegiate School in Karori,<br />
Wellington held a Design a Bow Tie<br />
competition during Bow Tie Week <strong>2013</strong><br />
which raised $50.70 for the MDA.<br />
Dympna Mulroy, the Wellington<br />
Branch fieldworker, was invited to judge<br />
the designs.<br />
“A lot <strong>of</strong> skill and effort went into<br />
making each <strong>of</strong> the bow ties with some<br />
very inventive and creative ideas. The<br />
standard was high and it was difficult to<br />
choose winners.”<br />
The Warehouse Petone very<br />
generously sponsored the first prize<br />
with a $25 gift voucher; “Picture This”,<br />
Petone provided second prize with a<br />
voucher to have a bow tie framed, Village<br />
Beads Petone sponsored third prize with<br />
a $10 gift voucher and fourth prize was<br />
an attractive hard covered notebook.<br />
All participating students received a<br />
small bag <strong>of</strong> MDA jelly beans.<br />
Dympna gave a presentation to the 50<br />
students in attendance about muscular<br />
dystrophy and how it manifests in our<br />
members. The students had studied<br />
David Hill’s book See Ya Simon which is<br />
MDA Wellington fieldworker, Dympna<br />
Mulroy, with students from Collegiate<br />
School in Karori, Wellington<br />
about a boy with muscular dystrophy.<br />
By using weights and other practical<br />
activities the girls were able to experience<br />
some <strong>of</strong> the difficulties members<br />
experience in their day to day lives.<br />
The students and their teacher, Sarah<br />
Harvey, provided feedback saying that<br />
the practical sessions and discussions<br />
about muscular dystrophy helped them<br />
to appreciate some <strong>of</strong> the challenges our<br />
members face within everyday tasks that<br />
they <strong>of</strong>ten take for granted.<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 18
MDA news<br />
Waiuku Volunteer Brigade make good on deal<br />
LEFT: Waiuku Volunteer Brigade Chief<br />
Fire Officer, Colin Riddle presents a<br />
$4000 donation for the MDA to MDA<br />
member and Waiuku identity Kevin<br />
Laing following the Waiuku Volunteer<br />
Fire Brigade Poker Run during Bow Tie<br />
Week.<br />
ABOVE INSET: Some <strong>of</strong> the hotrods<br />
and classic cars that entrants drove in<br />
the Poker Run.<br />
A significant contributor to the MDA’s<br />
Bow Tie Week appeal this year was the<br />
Waiuku Volunteer Fire Brigade, which<br />
donated a cheque for $4000 following a<br />
Poker Run they hosted in Franklin.<br />
The run started with a briefing at the<br />
fire station, where all entrants were given<br />
their first playing card, making their way<br />
first to Waiau Pa Fire Station then on to the<br />
Clevedon Hotel, the Ramarama Country <strong>In</strong>n,<br />
Tuakau Fire Station and Otaua. Participants<br />
picked up a card at each stop, at the end<br />
holding a hand <strong>of</strong> six cards. On the return<br />
to Waiuku Fire Station entrants were able to<br />
open their cards (they remained sealed until<br />
the return trip) and could throw away their<br />
worst card. Whoever had the best “Poker<br />
Hand” back at the station won.<br />
Firefighter Mark McDonagh says the<br />
event was a huge success.<br />
“As you can imagine it is a big<br />
undertaking and it took input from all<br />
26 members <strong>of</strong> the Brigade to put it<br />
together, as well as the awesome support<br />
the businesses <strong>of</strong> Waiuku always show us.”<br />
“The run was open for anyone to<br />
enter, they didn’t need to have a hot rod<br />
or motorbike. There were quite a few families<br />
that came along, although it was awesome<br />
to see how many classic cars and bikes came<br />
out for the day.” <br />
Mark says immense thanks are due to<br />
the major sponsors that contributed to<br />
the day - DW Homes (the naming rights<br />
sponsor), Carters, Gary Pyes 100%, Mitre10<br />
Waiuku, Power and Performance and Vanilla<br />
Homewares. <br />
The event was followed by a prize giving,<br />
dinner (a sheep on spit) and a live band,<br />
which played into the night. <br />
It was the second time the Waiuku<br />
Brigade has run the event and due to the<br />
success <strong>of</strong> both times, and the ability for<br />
the funds raised to go to other communitybased<br />
organisations, Mark says, the Brigade<br />
hopes to be able to continue the event on an<br />
annual basis.<br />
As part <strong>of</strong> <strong>Muscular</strong> <strong>Dystrophy</strong> Northern’s Bow Tie Week fundraising activities volunteers and members, including MDA Chief Executive<br />
Chris Higgins ( CENTRE ABOVE) also attended and collected at the HOG National Rally in Ellerslie and hosted a stand at Westfield Albany<br />
(PICTURED RIGHT ABOVE).<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 19
Your condition in review<br />
Mitochondrial myopathies<br />
A large group <strong>of</strong> conditions affecting more than one type <strong>of</strong> cell, tissue or organ commonly damaging nerve<br />
cells in the brain and muscles.<br />
What are mitochondrial<br />
myopathies?<br />
Mitochondrial diseases are a large<br />
group <strong>of</strong> diseases caused by damage to the<br />
mitochondria, the small, energy-producing<br />
structures that serve as the cells’ “power<br />
plants”. The more energy an organ needs the<br />
more mitochondria the cells will have.<br />
Nearly all our cells rely on mitochondria<br />
for a steady energy supply, so a mitochondrial<br />
disease can be a multisystem disorder<br />
affecting more than one type <strong>of</strong> cell, tissue<br />
or organ. Nerve cells in the brain and muscles<br />
both have a high number <strong>of</strong> mitochondria<br />
and thus appear to particularly damage when<br />
mitochondrial dysfunction occurs. The exact<br />
symptoms aren’t the same for everyone,<br />
because a person with mitochondrial<br />
disease can have a unique mixture <strong>of</strong><br />
healthy and defective mitochondria, with a<br />
unique distribution in the body. Also, some<br />
symptoms <strong>of</strong> mitochondrial disease (such as<br />
diabetes or heart arrhythmia) are common<br />
in the general population, or common<br />
to other neuromuscular diseases (such as<br />
muscle weakness). Usually, a person with<br />
a mitochondrial disease has two or more<br />
<strong>of</strong> these conditions, some <strong>of</strong> which occur<br />
together so regularly that they’re grouped<br />
into syndromes.<br />
A mitochondrial disease that causes<br />
prominent muscular problems is called<br />
a mitochondrial myopathy (myo means<br />
muscle, and pathos means disease); while<br />
a mitochondrial disease that causes both<br />
prominent neurological problems is called a<br />
mitochondrial encephalomyopathy (encephalo<br />
refers to the brain).<br />
What are the features <strong>of</strong><br />
mitochondrial myopathies?<br />
There are ten well-defined syndromes<br />
classified as mitochondrial myopathies<br />
(see details on page 26.) The symptoms<br />
can include muscle weakness or exercise<br />
intolerance, heart failure or rhythm<br />
disturbances, dementia, movement<br />
disorders, stroke-like episodes, deafness,<br />
blindness, droopy eyelids, limited mobility<br />
<strong>of</strong> the eyes, vomiting and seizures. The<br />
group <strong>of</strong> symptoms will depend on the<br />
specific myopathy. The prognosis for these<br />
disorders ranges in severity from progressive<br />
weakness to death. Most mitochondrial<br />
myopathies occur before the age <strong>of</strong> 20, and<br />
<strong>of</strong>ten begin with exercise intolerance or<br />
muscle weakness. During physical activity,<br />
muscles may become easily fatigued or<br />
weak. Muscle cramping is rare, but may<br />
occur. Nausea, headache and breathlessness<br />
are also associated with these disorders.<br />
Muscle weakness and wasting, and<br />
exercise intolerance are common to most<br />
syndromes. However the severity <strong>of</strong> any<br />
<strong>of</strong> these symptoms varies greatly from one<br />
person to the next, even in the same family. <strong>In</strong><br />
some individuals, weakness is most prominent<br />
in muscles that control movements <strong>of</strong> the<br />
eyes and eyelids. Two common consequences<br />
are the gradual paralysis <strong>of</strong> eye movements,<br />
called progressive external ophthalmoplegia<br />
(PEO), and drooping <strong>of</strong> the upper eyelids,<br />
called ptosis. Often, people automatically<br />
compensate for PEO by moving their heads<br />
to look in different directions, and might<br />
not even notice any visual problems. Ptosis<br />
is potentially more frustrating because it<br />
can impair vision and also cause a listless<br />
expression, but it can be corrected by surgery,<br />
or by using glasses that have a “ptosis crutch”<br />
to lift the upper eyelids. Mitochondrial<br />
myopathies also can cause weakness and<br />
wasting in other muscles <strong>of</strong> the face and<br />
neck, which can lead to slurred speech and<br />
difficulty with swallowing.<br />
Sometimes people with mitochondrial<br />
myopathies experience loss <strong>of</strong> muscle<br />
strength in the arms or legs, and might need<br />
braces or a wheelchair to get around. Exercise<br />
intolerance, also called exertional fatigue,<br />
refers to unusual feelings <strong>of</strong> exhaustion<br />
brought on by physical exertion. The degree<br />
<strong>of</strong> exercise intolerance varies greatly among<br />
individuals. Some people might only have<br />
trouble with athletic activities like jogging,<br />
while others might experience problems<br />
with everyday activities like walking to the<br />
mailbox or lifting a milk carton. Sometimes,<br />
exercise intolerance is associated with painful<br />
muscle cramps and/or injury induced pain.<br />
The cramps are actually sharp contractions<br />
that may seem to temporarily lock the<br />
muscles, while the injury-induced pain<br />
is caused by a process <strong>of</strong> acute muscle<br />
breakdown called rhabdomyolysis, leading<br />
to leakage <strong>of</strong> myoglobin from the muscles<br />
into the urine (myoglobinuria). Cramps or<br />
myoglobinuria usually occur when someone<br />
with exercise intolerance “overdoes it,” and<br />
can happen during the overexertion or several<br />
hours afterward.<br />
What causes mitochondrial<br />
myopathies?<br />
Mitochondrial myopathies are caused<br />
by mutations, or changes, in genes — the<br />
cells’ blueprint for making proteins. Genes<br />
are responsible for building our bodies, and<br />
are passed from parents to children, along<br />
with any mutations or defects they have.<br />
That means that mitochondrial diseases<br />
are inheritable, although they <strong>of</strong>ten affect<br />
members <strong>of</strong> the same family in different ways.<br />
Mutations in either nuclear DNA (nDNA)<br />
or mitochondrial DNA (mtDNA) can cause<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 20
Mitochondrial myopathies<br />
mitochondrial disease.<br />
Most nDNA (along with any mutations<br />
it has) is inherited in a Mendelian pattern,<br />
loosely meaning that one copy <strong>of</strong> each<br />
gene comes from each parent. Also, most<br />
mitochondrial diseases caused by nDNA<br />
mutations (including Leigh syndrome, MNGIE<br />
and even MDS) are autosomal recessive,<br />
meaning that it takes mutations in both<br />
copies <strong>of</strong> a gene to cause disease.<br />
Unlike nDNA, mtDNA passes only from<br />
mother to child. Thus, mitochondrial diseases<br />
caused by mtDNA mutations are unique<br />
because they’re inherited in a maternal<br />
pattern. A single cell can contain both mutant<br />
mitochondria and normal mitochondria, and<br />
the balance between the two will determine<br />
the cell’s health Also, when a mutation<br />
occurs in the mtDNA, only some <strong>of</strong> the<br />
many copies <strong>of</strong> mtDNA distributed within<br />
the mitochondria <strong>of</strong> each cell will carry the<br />
mutation - a situation known as heteroplasmy<br />
(see illustration opposite). The ratio <strong>of</strong> mutant<br />
to normal mtDNA in each tissue, along with<br />
other factors, may determine the severity <strong>of</strong><br />
the disease in an individual<br />
Diagnosis <strong>of</strong> mitochondrial<br />
myopathies<br />
None <strong>of</strong> the hallmark symptoms <strong>of</strong><br />
mitochondrial myopathies— muscle<br />
weakness, exercise intolerance, hearing<br />
impairment, ataxia, seizures, learning<br />
disabilities, cataracts, heart defects,<br />
diabetes and stunted growth — are unique<br />
to mitochondrial disease. However, a<br />
combination <strong>of</strong> three or more <strong>of</strong> these<br />
symptoms in one person strongly points to<br />
mitochondrial disease, especially when the<br />
symptoms involve more than one organ<br />
system. To evaluate the extent <strong>of</strong> these<br />
symptoms, a physician usually begins by<br />
taking the individual’s personal medical<br />
history, and then proceeds with physical and<br />
neurological exams.<br />
Diagnostic tests<br />
Physical examination<br />
The physical exam typically includes<br />
tests <strong>of</strong> strength and endurance, such as an<br />
exercise test, which can involve activities like<br />
repeatedly making a fist, or climbing up and<br />
down a small flight <strong>of</strong> stairs. The neurological<br />
exam can include tests <strong>of</strong> reflexes, vision,<br />
speech and basic cognitive (thinking) skills.<br />
Depending on information found during the<br />
medical history and exams, the physician<br />
might proceed with more specialised tests<br />
that can detect abnormalities in muscles,<br />
brain and other organs.<br />
Muscle biopsy<br />
The most important <strong>of</strong> these tests is the<br />
muscle biopsy, which involves removing a<br />
small sample <strong>of</strong> muscle tissue to examine.<br />
When treated with a dye that stains<br />
mitochondria red, muscles affected by<br />
mitochondrial disease <strong>of</strong>ten show ragged<br />
red fibres —muscle cells (fibres) that have<br />
excessive mitochondria. Other stains can<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 21
Your condition in review<br />
detect the absence <strong>of</strong> essential mitochondrial<br />
enzymes in the muscle. It’s also possible<br />
to extract mitochondrial proteins from the<br />
muscle and measure their activity.<br />
Scans and electrophysiology testing<br />
<strong>In</strong> addition to the muscle biopsy, noninvasive<br />
techniques can be used to examine<br />
muscle without taking a tissue sample.<br />
For instance, a technique called muscle<br />
phosphorus magnetic resonance spectroscopy<br />
(MRS) can measure levels <strong>of</strong> phosphocreatine<br />
and ATP (which are <strong>of</strong>ten depleted in muscles<br />
affected by mitochondrial disease). CT scans<br />
and MRI scans can be used to visually inspect<br />
the brain for signs <strong>of</strong> damage, and surface<br />
electrodes placed on the scalp can be used to<br />
produce a record <strong>of</strong> the brain’s activity called<br />
an electroencephalogram (EEG).<br />
Similar techniques might be used to<br />
examine the functions <strong>of</strong> other organs<br />
and tissues in the body. For example, an<br />
electrocardiogram (EKG) can monitor the<br />
heart’s activity, and a blood test can detect<br />
signs <strong>of</strong> kidney malfunction.<br />
Genetic testing<br />
A genetic test can determine whether<br />
someone has a genetic mutation that causes<br />
mitochondrial disease. Ideally, the test is done<br />
using genetic material extracted from blood<br />
or from a muscle biopsy. It’s important to<br />
realise that, although a positive test result can<br />
confirm diagnosis, a negative test result isn’t<br />
necessarily meaningful.<br />
Special issues in mitochondrial<br />
myopathies<br />
While there is no cure for these<br />
mitochondrial myopathies there are many<br />
treatments that can help manage symptoms<br />
Ataxia and mobility issues<br />
Often, mitochondrial encephalomyopathy<br />
causes ataxia, or trouble with balance and<br />
coordination. People with ataxia are usually<br />
prone to falls. Sometimes, people with<br />
mitochondrial myopathies experience loss <strong>of</strong><br />
muscle strength in the arms or legs. These<br />
problems can be partially avoided through<br />
physical and occupational therapy, and the<br />
use <strong>of</strong> supportive aids such as railings, a<br />
walker, a cane, braces, or — in severe cases —<br />
a wheelchair.<br />
Respiratory care<br />
Sometimes, these diseases can cause<br />
significant weakness in the muscles that<br />
support breathing. A person with mild<br />
respiratory problems might require occasional<br />
respiratory support, such as pressurised air,<br />
while someone with more severe problems<br />
might require permanent support from<br />
a ventilator. Those with mitochondrial<br />
disorders should watch for signs <strong>of</strong> respiratory<br />
insufficiency (such as shortness <strong>of</strong> breath or<br />
morning headaches), and have their breathing<br />
checked regularly by a specialist.<br />
Speech and swallowing<br />
Muscle wasting in the neck region can<br />
lead to slurred speech and difficulty with<br />
swallowing. <strong>In</strong> these instances, speech<br />
therapy or changing the diet to easier-toswallow<br />
foods can be useful.<br />
Cardiac care<br />
Sometimes, mitochondrial diseases<br />
directly affect the heart. <strong>In</strong> these cases, the<br />
usual cause is an interruption in the rhythmic<br />
beating <strong>of</strong> the heart, called a conduction<br />
block. Though dangerous, this condition is<br />
treatable with a pacemaker, which stimulates<br />
normal beating <strong>of</strong> the heart. Cardiac<br />
muscle damage also may occur. People with<br />
mitochondrial disorders may need to have<br />
regular examinations by a cardiologist.<br />
Renal care<br />
Some people with mitochondrial disease<br />
experience serious kidney problems,<br />
gastrointestinal problems and/or diabetes.<br />
Some <strong>of</strong> these problems are direct effects <strong>of</strong><br />
mitochondrial defects in the kidneys, digestive<br />
system or pancreas (in diabetes), and others<br />
are indirect effects <strong>of</strong> mitochondrial defects in<br />
other tissues.<br />
Special issues in children<br />
Vision: Though PEO and ptosis typically<br />
cause only mild visual impairment in adults,<br />
they’re potentially more harmful in children<br />
with mitochondrial myopathies.<br />
Because the development <strong>of</strong> the brain<br />
is sensitive to childhood experiences, PEO<br />
or ptosis during childhood can sometimes<br />
cause permanent damage to the brain’s visual<br />
system. For this reason, it’s important for<br />
children with signs <strong>of</strong> PEO or ptosis to have<br />
their vision checked by a specialist.<br />
Developmental delays: Due to<br />
muscle weakness, brain abnormalities<br />
or a combination <strong>of</strong> both, children with<br />
mitochondrial diseases may have difficulty<br />
developing certain skills. For example, they<br />
might take an unusually long time to reach<br />
motor milestones such as sitting, crawling<br />
and walking. As they get older, they may<br />
be unable to get around as easily as other<br />
children their age, and may have speech<br />
problems and/or learning disabilities. Children<br />
who are severely affected by these problems<br />
may benefit from services. Occupational<br />
therapy is important for children with<br />
mitochondrial myopathies. Mitochondrial<br />
myopathy can lead to respiratory problems<br />
that require support from a ventilator.<br />
Research<br />
While there is no cure for these<br />
conditions scientists continue to make<br />
significant progress in their quest to fully<br />
understand mitochondrial diseases and<br />
identify the genetic mutations responsible<br />
for these conditions.<br />
Research into stem cells therapy for<br />
affected individuals to restore normal<br />
metabolic conditions and halt damage<br />
to the mitochondria is ongoing as is the<br />
use <strong>of</strong> dietary supplements. These dietary<br />
supplements based on three natural<br />
substances involved in ATP production in<br />
our cells. Although they don’t work for<br />
everyone, they do appear to help some<br />
people. One substance, creatine, normally<br />
acts as a reserve for ATP by forming a<br />
compound called creatine phosphate. When<br />
a cell’s demand for ATP exceeds the amount<br />
its mitochondria can produce, creatine can<br />
release phosphate (the “P” in ATP) to rapidly<br />
enhance the ATP supply. <strong>In</strong> fact, creatine<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 22
Mitochondrial myopathies<br />
phosphate (also called phosphocreatine)<br />
typically provides the initial burst <strong>of</strong> ATP<br />
required for strenuous muscle activity.<br />
Another substance, carnitine, generally<br />
improves the efficiency <strong>of</strong> ATP production<br />
by helping import certain fuel molecules<br />
into mitochondria, and cleaning up some<br />
<strong>of</strong> the toxic byproducts <strong>of</strong> ATP production.<br />
Carnitine is available as an over-the-counter<br />
supplement called L-carnitine.<br />
Finally, coenzyme Q10, or coQ10, is<br />
a component <strong>of</strong> the electron transport<br />
chain, which uses oxygen to manufacture<br />
ATP. Some mitochondrial diseases<br />
are caused by coQ10 deficiency, and<br />
there’s good evidence that coQ10<br />
supplementation is beneficial in these<br />
cases. Some doctors think that coQ10<br />
supplementation also might alleviate<br />
other mitochondrial diseases. When<br />
considering taking dietary supplements<br />
please consult your doctor first.<br />
Exercise<br />
While the benefits <strong>of</strong> endurance training<br />
have been demonstrated at a physiological<br />
and biochemical level in mouse models<br />
further studies are needed to evaluate the<br />
best physical exercise regime for people with<br />
mitochondrial myopathies. Strengthening<br />
muscles and improving oxygen intake is<br />
definitely beneficial but over excursion can<br />
have the opposite effect. Any new exercise<br />
regime should be designed in conjunction<br />
with a physiotherapist or pr<strong>of</strong>essional with<br />
an understanding <strong>of</strong> mitochondrial disease.<br />
<strong>In</strong>formation for these<br />
articles was primarily sourced<br />
from:<br />
www.mda.org/disease/<br />
mitochondrial-myopathies,<br />
www.mitoresearch.org/<br />
mitodiseases.html, www.<br />
mitoaction.org/medicalinformat<br />
What are<br />
mitochondria and<br />
what do they do?<br />
Mitochondria are tiny structures<br />
called organelles found in every<br />
cell in our body and are similar to<br />
bacteria in many ways. Scientists<br />
believe that millions <strong>of</strong> years<br />
ago early life forms containing<br />
eukaryotic cells developed a symbiotic<br />
relationship with bacteria. These eukaryotic<br />
cells had a nucleus so could divide and<br />
multiply but because they could not use<br />
oxygen to sustain themselves they died <strong>of</strong>f<br />
once they became too big. The bacteria<br />
with their own DNA could utilise oxygen.<br />
These bacteria eventually evolved into the<br />
mitochondria <strong>of</strong> human cells allowing for<br />
larger creatures<br />
Within these organelles carbohydrate,<br />
fat and protein is broken down in the<br />
presence <strong>of</strong> oxygen to create the energy<br />
you need to function, both physically and<br />
mentally. Some cell types like muscles,<br />
liver and brain cells require more energy<br />
so contain a higher percentage <strong>of</strong><br />
mitochondria. Hair follicles have a smaller<br />
amount <strong>of</strong> mitochondria.<br />
Mitochondria produce energy in the<br />
form <strong>of</strong> adenosine triphosphate (ATP),<br />
which is then transported to the cytoplasm<br />
<strong>of</strong> a cell for use in numerous cell functions<br />
The process <strong>of</strong> converting food and oxygen<br />
(fuel) into energy known as oxidative<br />
phosphorylation requires hundreds <strong>of</strong><br />
chemical reactions, and each chemical<br />
reaction must run almost perfectly in<br />
order to have a continuous supply <strong>of</strong><br />
energy. When one or more components<br />
<strong>of</strong> these chemical reactions does not run<br />
perfectly, there is an energy crisis, and<br />
the cells cannot function normally. As a<br />
result, the incompletely burned food might<br />
accumulate as poison inside the body.<br />
This poison can stop other chemical<br />
reactions that are important for the cells<br />
to survive, making the energy crisis even<br />
worse. <strong>In</strong> addition, these poisons can act<br />
as free radicals (reactive substances that<br />
readily form harmful compounds with<br />
other molecules) that can damage the<br />
mitochondria over time, causing damage<br />
that cannot be reversed.<br />
<strong>In</strong> addition to energy production,<br />
mitochondria play a role in several<br />
other cellular activities. For example,<br />
mitochondria help regulate the selfdestruction<br />
<strong>of</strong> cells (apoptosis). They<br />
are also necessary for the production <strong>of</strong><br />
substances such as cholesterol and heme (a<br />
component <strong>of</strong> hemoglobin, the molecule<br />
that carries oxygen in the blood).<br />
The central role <strong>of</strong> mitochondria in<br />
cellular function means that dysfunction <strong>of</strong><br />
mitochondria in any organ system can lead<br />
to widely varying clinical presentations.<br />
Primary mitochondrial diseases, which<br />
includes mitochondrial myopathies, are<br />
relatively common and affect up to 1 in<br />
5000 people. Mitochondrial dysfunction<br />
secondary to other diseases is even more<br />
common and plays a role in Alzheimer<br />
disease and Parkinsons disease and is<br />
also involved in the aging process. With<br />
this increasing understanding <strong>of</strong> the<br />
biochemistry <strong>of</strong> mitochondrial activity<br />
scientists are now researching a variety <strong>of</strong><br />
treatment strategies .<br />
Mitochondrial DNA (mDNA)<br />
Mitochondria like bacteria have their<br />
own set <strong>of</strong> DNA which is inherited from<br />
one’s mother, not father. This is because<br />
only the egg contains mitochondria,<br />
while sperm cells are mitochondria-free<br />
by the time it fuses with the egg. Thus,<br />
mitochondrial diseases caused by mtDNA<br />
mutations are unique because they’re<br />
inherited in a maternal pattern<br />
....... continued on the following page<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 23
Your condition in review<br />
What are mitochondria and what do they<br />
do?....... continued from the previous page.<br />
Looking for contact with others<br />
with mitochondrial myopathy/ IBM<br />
Another unique feature <strong>of</strong> mtDNA diseases<br />
arises from the fact that a typical human<br />
cell — including the egg cell — contains only<br />
one nucleus but hundreds <strong>of</strong> mitochondria.<br />
A single cell can contain both mutant<br />
mitochondria and normal mitochondria, and<br />
the balance between the two will determine<br />
the cell’s health. Also, when a mutation<br />
occurs in the mtDNA, only some <strong>of</strong> the<br />
many copies <strong>of</strong> mtDNA distributed within<br />
the mitochondria <strong>of</strong> each cell will carry the<br />
mutation -- a situation known as heteroplasmy<br />
(see illustration below). The ratio <strong>of</strong> mutant<br />
to normal mtDNA in each tissue, along with<br />
other factors, may determine the severity <strong>of</strong><br />
the disease in an individual.<br />
Maternal inheritance <strong>of</strong> mitochondrial DNA<br />
mutations.<br />
The DNA inside mitochondria is distinct<br />
from DNA inside the nucleus in its genetic<br />
code. Mitochondrial DNA contains 37<br />
genes, all <strong>of</strong> which are essential for normal<br />
mitochondrial function. Thirteen <strong>of</strong> these<br />
genes provide instructions for making<br />
enzymes involved in oxidative phosphorylation<br />
(producing energy ). The remaining genes<br />
provide instructions for making molecules<br />
called transfer RNAs (tRNAs) and ribosomal<br />
RNAs (rRNAs), which are chemical cousins<br />
<strong>of</strong> DNA. These types <strong>of</strong> RNA help assemble<br />
protein building blocks (amino acids) into<br />
functioning proteins.<br />
Refer graphic on page 24<br />
Toward the end <strong>of</strong> the 1990’s, I<br />
was having to travel from Masterton to<br />
Wellington each year to visit a neurologist<br />
at Wellington Hospital in the hope <strong>of</strong><br />
getting a diagnosis for the weakness that<br />
was becoming more noticeable in my left<br />
hand and arm.<br />
This had made my job as an ambulance<br />
<strong>of</strong>ficer rather precarious as I couldn’t lift or<br />
carry a stretcher as I was required to do.<br />
Finally, after the usual neurological tests<br />
and painful EMGs, it was decided I probably<br />
had IBM but a confirmation could only be<br />
achieved with a muscle biopsy. As this was<br />
not going to provide a cure for my problem,<br />
was probably going to hurt quite a bit and<br />
there was no compulsion to go ahead with<br />
it, I said I thought I would give it a miss<br />
thank you very much.<br />
While in hospital in mid - 2006, I was<br />
once again pressured to have the biopsy<br />
to which I relented and it was undertaken<br />
in November. Somewhere along the line,<br />
either the muscle specimen or the report<br />
got sent to the wrong hospital because<br />
it was several months later that we got<br />
the result back. This indicated that I had<br />
some “ragged red fibres” within the<br />
muscle sample which was indicative <strong>of</strong><br />
mitochondrial myopathy. That was all very<br />
well but what did all that mean and how<br />
was it going to affect me in the future? It<br />
was suggested that I should be given an<br />
electron microscope test to confirm the<br />
diagnosis but that has never happened.<br />
By checking the web for some detail,<br />
I have found that tiredness is a great<br />
indicator <strong>of</strong> the condition but as I have little<br />
to no ability to balance while standing, let<br />
alone walking, tiredness has been with me<br />
for some time. Recently, I have noticed a<br />
difference in my ability to sound certain<br />
words and my tongue has taken on a<br />
degree <strong>of</strong> numbness which makes eating<br />
MDA member and IBM support group<br />
convenor, Don Ross.<br />
just that much more difficult. I now wonder<br />
if the deafness in my left ear may have been<br />
more than just age related. I have pr<strong>of</strong>ound<br />
numbness in the calves <strong>of</strong> both legs but this<br />
what I expected to happen with my IBM.<br />
Just weeks ago, my wife Pat was going<br />
through all my old copies <strong>of</strong> <strong>In</strong> <strong>Touch</strong><br />
and she came across a story by Verina<br />
Kuriger (Autumn 2008) and found it most<br />
interesting in that the symptoms she talks<br />
about are what I am experiencing. Like her,<br />
I have been fortunate to have the attention<br />
<strong>of</strong> a very good O/T so I have all the aids I<br />
need to stay reasonably mobile in and out<br />
<strong>of</strong> the home.<br />
I would love to get in touch with anybody<br />
else who has been diagnosed with the<br />
condition. My email is teddy@wise.net.nz<br />
Supplied by Don Ross<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 24
Living with mitochondrial myopathy<br />
Setting an example for the young’uns.<br />
Nine years ago, when I was 64, I had never<br />
heard <strong>of</strong> MM. I’ve always been an incredibly<br />
busy, fit and active person, with a physically<br />
demanding job and a love <strong>of</strong> scuba-diving,<br />
sailing and water-skiing. The first sign that all<br />
was not right in my world was when I started<br />
to come home after a hard day’s work and<br />
would collapse in a heap with exhaustion<br />
for a couple <strong>of</strong> days. I ignored this, putting<br />
it down to just getting that little bit older.<br />
Then I developed droopy eye lids – as in I<br />
couldn’t open my eyes very much. A local<br />
surgeon thought the muscles above my<br />
eyes had detached from the eye lids and,<br />
with a short operation, he would reattach<br />
the muscles. However, when he undertook<br />
the surgery he couldn’t find the muscles at<br />
all, so suggested I contact a specialist who<br />
subsequently inserted ‘straps’ under the<br />
skin <strong>of</strong> my eyelids and connected them to<br />
my forehead. Now in order to open my eyes<br />
I have to raise my eyebrows. The specialist<br />
suggested I have a muscle biopsy to check if<br />
there was any underlying reason for having no<br />
eyelid muscles. After several visits to Auckland<br />
hospital and several biopsies later I was told I<br />
had MM and that it was reasonable advanced.<br />
MM is when the mitochondrial in your<br />
muscles start dying, and thus your muscles<br />
slowly waste away. It’s rare and few doctors<br />
have ever heard about the condition. Those<br />
that have any experience <strong>of</strong> it tell me the<br />
prognosis is different for everyone, and that<br />
my life expectancy would be about five years,<br />
with the last few years spent in a wheelchair<br />
and drinking food through a tube. Oh joy!<br />
After getting over the initial shock, my wife<br />
Sue and I starting making some plans – e.g.<br />
if I was in a wheelchair could my wife look<br />
after me or would I need to be in a home? My<br />
wife and I searched the internet to find out<br />
as much as possible about the disease – but<br />
there was little to find. The majority <strong>of</strong> my<br />
care has been by my GP – he’s been fantastic<br />
and better than any specialist. Between us we<br />
are probably <strong>New</strong> Zealand’s experts on MM!<br />
Over the last ten years there is still little<br />
new information about MM – I still have no<br />
idea what my prognosis is, but I am yet to be<br />
Peter ABOVE on a<br />
Coastguard flight and<br />
RIGHT with one <strong>of</strong> his<br />
much loved grandchildren.<br />
confined to a wheelchair. To<br />
eat requires many muscles,<br />
so you can imagine that as<br />
the mitochondria die, eating<br />
is becoming more and<br />
more difficult, and choking is a major risk. I<br />
regularly vomit up many perfectly lovely roast<br />
dinners - going out for dinner therefore can<br />
become a little embarrassing. Speaking also<br />
is difficult – especially when I’m tired. People<br />
just think I’m drunk! You have to laugh at the<br />
craziness <strong>of</strong> it all really.<br />
I wanted to keep working in order to<br />
kept my mind active and myself sane – and<br />
my wife was incredibly supportive <strong>of</strong> this<br />
(although we had lots <strong>of</strong> arguments initially<br />
about it). We spent many years planning how<br />
she would cope when I was gone. However,<br />
three years ago Sue died suddenly. That was<br />
never part <strong>of</strong> the plan – it never is –it was<br />
meant to be me first, not her. I’m not sure<br />
how I have coped since her death but I have.<br />
Stressful events tend to set <strong>of</strong>f a<br />
downward spiral <strong>of</strong> weight loss, until I plateau<br />
again for a while. I’ve lost muscle tone and<br />
strength and look like I’m anorexic – despite<br />
eating like a horse. With no body fat my body<br />
struggles to regulate my body temperature<br />
and I get the shivers. I am finding the simple<br />
act <strong>of</strong> getting up out <strong>of</strong> a chair and walking<br />
increasingly difficult, but I still run a plumbing<br />
and drainage business plus a marine electrical<br />
business. I’m also the training <strong>of</strong>ficer for<br />
the Northland Coastguard Air Patrol and<br />
spend most days driving myself between<br />
KeriKeri and Whangarei. Despite no previous<br />
experience, I’ve become an incredible cook<br />
(famous for my Xmas cake, Afghans and<br />
lemon meringue pie) and still do my own<br />
housework. I have two great sons, five<br />
grandchildren and the best network <strong>of</strong> friends<br />
you could ever ask for. Together with the<br />
<strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong>, they all keep<br />
a close eye on me. I also started ticking things<br />
<strong>of</strong>f my bucket list – I’ve done a month long<br />
cruise through the Mediterranean, a skydive<br />
for my 70th birthday, a zipline flying fox while<br />
hanging upside down through the trees in<br />
Canada, and have been front and centre to<br />
watch the start and finish <strong>of</strong> the Sydney to<br />
Hobart yacht race (because I couldn’t wangle<br />
a place on one <strong>of</strong> the boats). Whilst my quality<br />
<strong>of</strong> life has been dramatically affected, I’m still<br />
alive and active, and am reminded <strong>of</strong> this as I<br />
watch my aging friends pass away from more<br />
common conditions such as heart attacks<br />
and cancer. I’m doing OK for an old bugger.<br />
Life is what you make it after all. You can sit<br />
and wallow in self-pity or you can set a great<br />
example to your grandchildren and show<br />
them that despite your physical limitations<br />
a positive mental attitude and a good laugh<br />
makes all the difference to a good life.<br />
Supplied by Peter Greenaway<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 25
Your condition in review<br />
What are the different types <strong>of</strong> mitochondrial myopathy?<br />
Kearns-Sayre syndrome (KSS)<br />
Onset: Before age 20<br />
Symptoms: This disorder is defined by<br />
PEO and pigmentary retinopathy, a “saltand-pepper”<br />
pigmentation in the retina<br />
that can affect vision, but <strong>of</strong>ten leaves it<br />
intact. Other common symptoms include<br />
conduction block (in the heart) and ataxia.<br />
Less typical symptoms are mental retardation<br />
or deterioration, delayed sexual maturation<br />
and short stature.<br />
Leigh syndrome (subacute<br />
necrotising encephalomyopathy)<br />
and maternally inherited Leigh<br />
syndrome (MILS)<br />
Onset: <strong>In</strong>fancy<br />
Symptoms: Leigh syndrome causes brain<br />
abnormalities that can result in ataxia,<br />
seizures, impaired vision and hearing,<br />
developmental delays and altered control over<br />
breathing. It also causes muscle weakness,<br />
with prominent effects on swallowing, speech<br />
and eye movements.<br />
Mitochondrial DNA depletion<br />
syndrome (MDS)<br />
Onset: <strong>In</strong>fancy<br />
Symptoms: This disorder typically causes<br />
muscle weakness and/or liver failure,<br />
and more rarely, brain abnormalities.<br />
“Floppiness,” feeding difficulties and<br />
developmental delays are common<br />
symptoms; PEO and seizures are less<br />
common.<br />
symptoms include PEO, general muscle<br />
weakness, exercise intolerance, hearing loss,<br />
diabetes and short stature.<br />
Mitochondrial neurogastrointestinal<br />
encephalomyopathy (MNGIE)<br />
Onset: Usually before age 20<br />
Symptoms: This disorder causes PEO,<br />
ptosis (droopy eyelids), limb weakness and<br />
gastrointestinal (digestive) problems, including<br />
chronic diarrhoea and abdominal pain.<br />
Another common symptom is peripheral<br />
neuropathy (a malfunction <strong>of</strong> the nerves that<br />
can lead to sensory impairment and muscle<br />
weakness).<br />
Myoclonus epilepsy with ragged<br />
red fibres (MERRF)<br />
Onset: Late childhood to adolescence<br />
Symptoms: The most prominent symptoms<br />
are myoclonus (muscle jerks), seizures, ataxia<br />
and muscle weakness. The disease also can<br />
cause hearing impairment and short stature.<br />
Neuropathy, ataxia and retinitis<br />
pigmentosa (NARP)<br />
Onset: <strong>In</strong>fancy to adulthood<br />
GRAPHIC: The distinct nature <strong>of</strong> mitochondria with mutant DNA<br />
Symptoms: NARP causes neuropathy (a<br />
malfunction <strong>of</strong> the nerves that can lead to<br />
sensory impairment and muscle weakness),<br />
ataxia and retinitis pigmentosa (degeneration<br />
<strong>of</strong> the retina in the eye, with resulting loss <strong>of</strong><br />
vision). It also can cause developmental delay,<br />
seizures and dementia.<br />
Pearson syndrome<br />
Onset: <strong>In</strong>fancy<br />
Symptoms: This syndrome causes severe<br />
anaemia and malfunction <strong>of</strong> the pancreas.<br />
Children who survive the disease usually go<br />
on to develop Kearns-Sayre syndrome.<br />
Progressive external<br />
ophthalmoplegia (PEO)<br />
Onset: Usually in adolescence or early<br />
adulthood<br />
Symptoms: PEO — the gradual paralysis<br />
<strong>of</strong> eye movements — is <strong>of</strong>ten a symptom<br />
<strong>of</strong> mitochondrial disease, but sometimes<br />
it stands out as a distinct syndrome.<br />
It’s frequently associated with exercise<br />
intolerance.<br />
Mitochondrial<br />
encephalomyopathy, lactic<br />
acidosis and strokelike<br />
episodes (MELAS)<br />
Onset: Childhood to early adulthood<br />
Symptoms: MELAS causes recurrent<br />
stroke like episodes in the brain,<br />
migraine-type headaches, vomiting and<br />
seizures, and can lead to permanent<br />
brain damage. Other common
TA iQ the <strong>New</strong> Standard<br />
The new TA iQ MWD mid-wheel drive power chair is designed to improve your outdoor drive comfort and<br />
access, while providing you with superior functionality indoors.<br />
So why is the TA iQ unique?<br />
Outdoors: The suspension is very s<strong>of</strong>t, combined with pneumatic tyres, the TA iQ provides a smoother ride<br />
when travelling over bumps and kerbs. The unique suspension design allows the TA iQ to climb over larger<br />
obstacles.<br />
<strong>In</strong>doors: With a very small turning radius <strong>of</strong> only 45 cm, the TA iQ can spin easily in tight spaces. The TA iQ<br />
has the lowest floor to seat height <strong>of</strong> only 38 cm, lower than any other power chair, allowing you to easily sit at<br />
a desk or table, or even drive a vehicle. Every TA iQ has the standard specification lift/elevation function <strong>of</strong> 30<br />
cm (38-68 cm), allowing you to reach higher cupboards, benches, and basins.<br />
Performance: The TA iQ is the fastest with a top speed <strong>of</strong> 12.5km/h which it will reach in 3 seconds.<br />
Also with an optimum range <strong>of</strong> 40km you will travel further, faster.<br />
Designed and manufactured in Denmark with quality European motors, actuators and controllers. Safety tested<br />
in Germany. Also available in rear wheel drive and front wheel drive configuration.<br />
So if you are evaluating a new power chair you have to try the TA iQ for yourself. You can ask for a demo to<br />
purchase direct, or ask your therapist to arrange a MOH or ACC trial, then you decide.<br />
Experience for yourself.<br />
Seat height:<br />
Only 38cm<br />
Suspension:<br />
More comfortable<br />
Higher:<br />
30 cm elevation<br />
Faster:<br />
12.5 km/h<br />
Further:<br />
40km range<br />
0800 238 423 www.mortonperry.co.nz advice@mortonperry.co.nz
Research and relevance<br />
Recent developments in the treatment <strong>of</strong> neuromuscular disorders<br />
Lawrence Z. Stern, M.D. The University<br />
<strong>of</strong> Arizona Medical Center<br />
April 19, <strong>2013</strong><br />
The following are the key points <strong>of</strong><br />
Larry’s presentation at the mini conference in<br />
Christchurch following the MDA’s AGM in April.<br />
Much <strong>of</strong> the research in this area has<br />
focused on Duchenne muscular dystrophy,<br />
which is caused by a number <strong>of</strong> different<br />
genetic mutations in the dystrophin gene –<br />
meaning that one gene therapy approach<br />
is not going to be suitable for all boys with<br />
Duchenne. Research into Duchenne muscular<br />
dystrophy is likely to have positive knock-on<br />
effects for research into other neuromuscular<br />
conditions with the knowledge gained from<br />
research in this area benefitting those with<br />
other neuromuscular conditions.<br />
There are three antisense mediated<br />
exon skipping therapies currently in clinical<br />
trial phase. All <strong>of</strong> these therapies are being<br />
investigated to see whether they can turn<br />
a Duchenne-like presentation in a patient<br />
with Duchenne muscular dystrophy to a<br />
Becker muscular dystrophy-like presentation.<br />
Eteplirsen (Serepta) targets exon 51. Trials<br />
have shown that after one year <strong>of</strong> treatment,<br />
the 6-minute walking distance increased by<br />
21 metres. At 62 weeks <strong>of</strong> treatment, benefit<br />
was sustained and treated boys walked 62<br />
metres further than those receiving placebo.<br />
The other two therapies are Drisapersen<br />
(GlaxoSmithKline) and PRO044 (Prosensa), see<br />
the article on page 32 for more information.<br />
Ataluren (PTC Therapeutics) is another<br />
promising therapy for boys with nonsense<br />
mutations. After 48 weeks <strong>of</strong> treatment, boys<br />
walked 30 metres more in 6 minutes than<br />
those on placebo. Eteplirsen and Ataluren<br />
have now been submitted to the FDA for<br />
evaluation and approval.<br />
While the above therapies try to enhance<br />
the body’s ability to make dystrophin<br />
another approach is to increase the amount<br />
<strong>of</strong> utrophin, which may be able to act as<br />
a substitute for dystrophin. One drug in<br />
clinical trials, SMTC1100, has been shown to<br />
increase utrophin by 50% in DMD patient<br />
cell lines in the lab. <strong>In</strong>itial trials have shown<br />
it to be safe and well-tolerated in healthy<br />
volunteers. Clinical trials are beginning in<br />
DMD and BMD patients.<br />
Other conditions where therapies have<br />
shown promising results are myotonic<br />
dystrophy, spinal muscular atrophy (SMA) and<br />
Freidreichs ataxia.<br />
Myotonic dystrophy<br />
An antisense compound ASO44536<br />
(Gapmer) is thought to break up RNA/<br />
protein clumps in nuclei <strong>of</strong> cultured cells. The<br />
compound attracts enzymes which partially<br />
digest and then destroy abnormal RNA. <strong>In</strong> a<br />
myotonic dystrophy mouse model it reduced<br />
RNA clumping, reduced muscle shrinkage and<br />
eliminated myotonia. <strong>In</strong>terestingly the effects<br />
were long-lasting with the benefits lasting for<br />
one year after stopping treatment.<br />
Spinal muscular atrophy (SMA)<br />
<strong>In</strong> SMA the SMN1 gene is not functioning<br />
correctly. An antisense drug ISIS-SMNRx is<br />
designed to increase the amount <strong>of</strong> survival<br />
motor neuron<br />
(SMN) production<br />
by using the<br />
“backup” SMN2<br />
genes. This has<br />
Lawrence Z. Stern<br />
been shown to be<br />
safe and tolerated<br />
when injected into spinal fluid <strong>of</strong> 28 children<br />
with SMA with some improvement in motor<br />
function but more trials are needed to verify<br />
the benefits.<br />
Another experimental drug RG3039<br />
increased SMN protein in SMA cells. So far<br />
it has been shown to preserve mobility and<br />
increase lifespan in animal models <strong>of</strong> SMA.<br />
Freidreich ataxia<br />
A Phase I clinical trial <strong>of</strong> histone deacetylase<br />
inhibitor is underway in Italy.<br />
This is the first therapy specifically<br />
developed to treat the underlying cause <strong>of</strong> FA –<br />
the “turned <strong>of</strong>f” frataxin gene. It has shown to<br />
increase frataxin production in mouse models<br />
by turning the frataxin gene back on, allowing<br />
cells to read genetic instructions.<br />
Also presenting at the conference were,<br />
ophthalmology PhD student and, the first<br />
recipient <strong>of</strong> the MDA’s NRFT scholarship,<br />
Hannah Kersten and Bridget Williams<br />
from the Student Volunteer Army. Hannah<br />
presented her preliminary findings on the<br />
differences in the epiretinal membranes <strong>of</strong><br />
people with myotonic dystrophy while Bridget<br />
explained how her group are mobilising<br />
students to provide support to eathquake<br />
affected Canterbury residents.<br />
OPTIMISTIC focuses on myotonic<br />
dystrophy and involves an international<br />
multicentre intervention. The study, which<br />
was awarded €3million from the European<br />
Commission’s FP7 call in 2012, is coordinated<br />
by Baziel van Engelen from Radbound<br />
University Nijmegen Medical Centre in the<br />
Netherlands and includes seven collaborative<br />
partners from France, Germany, United<br />
Kingdom and the Netherlands.<br />
OPTIMISTIC will investigate the effect <strong>of</strong><br />
exercise training and cognitive behavioural<br />
therapy (CBT) on patients with myotonic<br />
dystrophy in order to find new and innovative<br />
ways to improve quality <strong>of</strong> life; in doing so<br />
protocols and guidelines will be developed<br />
specifically for this complex disease. Over 200<br />
patients will be involved in this project across<br />
Europe and recruitment is expected to start in<br />
2014. <strong>In</strong> addition OPTIMISTIC will utilise this<br />
opportunity to work towards standardising<br />
cardiac screening procedures and to carry out<br />
genetic analysis to better develop prognosis<br />
tools. Furthermore OPTIMISTIC aims to<br />
develop and validate clinically significant<br />
outcome measures that can be used in future<br />
clinical trials.<br />
The project will be closely linked to the<br />
TREAT-NMD Alliance and, as a member <strong>of</strong> the<br />
TREAT NMD Alliance, MDA NZ will keep <strong>New</strong><br />
Zealanders with myotonic dystrophy informed<br />
about the care guidelines and protocols that<br />
will result from this trial.<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 28
Research and relevance<br />
Behavioural management in<br />
neuromuscular conditions<br />
Research indicates that for many families the behavioural problems that can occur<br />
with a neuromuscular condition (NMC) are more stressful than the medical/<br />
physical aspects. Behaviour is a symptom and should be acknowledged and<br />
managed with appropriate support and treatment. Dr James Poysky, a clinical<br />
psychologist and paediatric neuropsychologist in neuromuscular conditions,<br />
presented at the Riding the Wave neuromuscular conference in 2012 about the<br />
different factors that can cause behaviour problems, pr<strong>of</strong>essional interventions<br />
available and strategies aimed at compliance and de-escalating conflict situations.<br />
MDA Wellington fieldworker, Dympna Mulroy attended the conference and the<br />
following is her summary <strong>of</strong> the information presented.<br />
What are behavioural problems?<br />
Behavioural problems may present as:<br />
• Moodiness, low mood, refusal to<br />
cooperate;<br />
• Bad temper, temper tantrums,<br />
screaming, swearing;<br />
• Frustration, throwing objects,<br />
hitting, biting;<br />
• Demanding behaviour, repeated<br />
requests.<br />
All <strong>of</strong> these behaviours in themselves are<br />
not unusual; it is only when they become<br />
more extreme and/or affect family life that<br />
they become problematic.<br />
Potential causes <strong>of</strong> behaviour<br />
problems<br />
There may be one or more reasons<br />
that trigger a change in behaviour.<br />
Various psychological, physical and social<br />
factors (such as deteriorating mobility and<br />
dependence on others) will impact on a<br />
persons’ life at different stages in their<br />
journey. This can lead to frustration and<br />
embarrassment, even among the youngest<br />
children and for some these emotions may<br />
be acted out through their behaviour.<br />
• Psychological<br />
Coping with a neuromuscular condition<br />
can cause various amounts <strong>of</strong> anxiety and<br />
stress. Future aspirations and goals may be<br />
unattainable and one’s sense <strong>of</strong> purpose<br />
may be altered. Most people learn to adjust<br />
and cope with having a neuromuscular<br />
condition but there will be times when they<br />
feel overwhelmed with emotional distress. As<br />
a condition progresses, children and young<br />
adults become more aware <strong>of</strong> their capabilities<br />
and limitations in comparison to their peers<br />
which can lead to adjustment problems<br />
especially as a person’s mobility deteriorates.<br />
Feelings <strong>of</strong> frustration, sadness, anger or<br />
anxiety can be experienced. These are normal<br />
reactions to a stressful situation and are<br />
more likely to be triggered during important<br />
developmental periods or times <strong>of</strong> change.<br />
• Psychosocial factors<br />
These include family stress or conflict;<br />
peer interactions and teacher/adult<br />
relationships.<br />
Parents want the best for their children<br />
and <strong>of</strong>ten have to juggle various roles and<br />
commitments to meet their child’s needs.<br />
At times individuals can feel overwhelmed<br />
dealing with these daily demands and<br />
stresses. <strong>In</strong> times <strong>of</strong> stress, managing a<br />
child’s behaviour can be more challenging<br />
if the parents/teachers/carers/whanau<br />
coping abilities and mental capacity are<br />
overwhelmed.<br />
Some teenagers have difficulty<br />
establishing their independence because<br />
they require more care and assistance from<br />
others such as parents. As muscle weakness<br />
progresses, they are at risk <strong>of</strong> becoming<br />
more isolated or socially withdrawn. Parents<br />
and teachers should look for signs <strong>of</strong> chronic<br />
sadness, depression or anxiety.<br />
While most individuals are not depressed<br />
or anxious, there is an increased chance when<br />
compared to peers. Depression is different<br />
from normal feelings <strong>of</strong> sadness, it is more<br />
pervasive, longer lasting (weeks to months<br />
instead <strong>of</strong> a day here or there) and powerful<br />
(interfering with daily activities, relationships<br />
and goals). Younger children are more likely<br />
to show symptoms <strong>of</strong> irritability, aggression,<br />
over-sensitivity or physical complaints, and<br />
do not always seem outwardly depressed.<br />
Most children have difficulty describing<br />
their emotions or identifying the cause <strong>of</strong><br />
their distress. Depression and anxiety can<br />
be very serious conditions and should be<br />
addressed with appropriate interventions and<br />
pr<strong>of</strong>essional support.<br />
• Medical factors<br />
Medical treatments, procedures and<br />
assessments will vary from person to person<br />
and can consume their normal routine. This<br />
may impact on their emotions, sense <strong>of</strong><br />
purpose and peer connections, and lead to<br />
disruptive behaviour.<br />
Fatigue is a major symptom in<br />
neuromuscular conditions. When a person<br />
is fatigued they find it difficult to reason,
problem solve, comprehend and behave<br />
appropriately which can be manifested in<br />
their behaviour.<br />
Some people with neuromuscular<br />
conditions take steroids or other medications<br />
to help manage their symptoms and some<br />
<strong>of</strong> these are known to cause behavioural<br />
problems. Prednisone is the steroid most<br />
widely used to treat Duchenne muscular<br />
dystrophy. It slows muscle loss and<br />
dramatically improves strength for most boys.<br />
On the other hand, it can cause irritability and<br />
some psychological side effects, which may<br />
affect a person’s behaviour and academic<br />
performance. Psychological side effects from<br />
steroids include difficulty concentrating,<br />
sleeping and controlling emotions. Some <strong>of</strong><br />
these problems may have existed before the<br />
child started taking medications but they<br />
were less severe and noticeable or considered<br />
to be a problem. It is advisable to speak to<br />
the child’s consultant/specialist if you think<br />
medications are having an adverse effect on a<br />
child’s behaviour and emotions.<br />
• Physical<br />
Behaviour can arise in response to a<br />
physical need such as pain and discomfort,<br />
fatigue or hunger.<br />
“Hangry” = Hungry + Angry<br />
It has been shown that when a person is<br />
hungry (even if they don’t feel it) they may<br />
become angry, irrational, mean/ aggressive<br />
and emotionally sensitive/labile. This is due<br />
to lowered blood glucose levels. A return to<br />
happy/normal mood can be seen once their<br />
blood sugar glucose level returns to normal.<br />
• Impact on brain functioning<br />
Some neuromuscular conditions such as<br />
Duchenne muscular dystrophy can lead to<br />
cognitive weakness and neurobehavioral<br />
disorders. While scientists are still<br />
investigating the exact role <strong>of</strong> dystrophin in<br />
the brain, not having dystrophin seems to<br />
cause an increased risk for specific cognitive<br />
weaknesses and learning difficulties. This<br />
does not mean that all boys with Duchenne<br />
will have deficits in these areas.<br />
Boys with problems in this area will have<br />
difficulty adapting to changes in expectations<br />
or requirements, or in transitioning from one<br />
activity to the next. They can get stuck on<br />
one idea, and have a hard time shifting their<br />
thinking away from it, even when others are<br />
getting annoyed or angry with them. They<br />
may appear stubborn or hard-headed, but it<br />
is important to keep in mind that this reflects<br />
a cognitive weakness rather than a character<br />
flaw. Problems with executive functioning<br />
commonly occur in the presence <strong>of</strong> ADHD<br />
and autism.<br />
• Other factors<br />
Young people regardless <strong>of</strong> whether<br />
they have a long term condition can have<br />
difficulty learning behavioural strategies and<br />
applying them to appropriate environments<br />
and situations.<br />
Remember they are a normal child who<br />
happens to have weak muscles!<br />
How to manage behaviour?<br />
There are a number <strong>of</strong> ways to deal with<br />
behaviour depending on the circumstances.<br />
1. General treatment<br />
recommendations - e.g. Seeking pr<strong>of</strong>essional<br />
assistance, support networks<br />
2. Behavioural management<br />
techniques to be utilised by the parent/<br />
teacher/whanau<br />
General treatment recommendations<br />
• There are a number <strong>of</strong> trained<br />
pr<strong>of</strong>essionals who are able to evaluate<br />
behaviour and provide necessary support:<br />
neuropsychological/psychological;<br />
developmental paediatrics; psychiatric;<br />
social worker. The interventions used are the<br />
same for someone without a neuromuscular<br />
condition; remember the mental health<br />
pr<strong>of</strong>essional doesn’t need to be an “expert”<br />
in these conditions.<br />
• Psychotherapy treatments include:<br />
Parental behavioural management training;<br />
individual therapy; group therapy; applied<br />
behavioural analysis.<br />
• Social interventions: Talking about<br />
the condition with the child, their peers,<br />
teachers etc. Developing their interests and<br />
supporting them to stay involved in groups<br />
and activities.<br />
• Promoting independence and selfadvocacy<br />
in the young person.<br />
• Family interventions: Counselling,<br />
building support networks, marital support,<br />
involvement in <strong>Muscular</strong> <strong>Dystrophy</strong><br />
<strong>Association</strong>, siblings support.<br />
• Psychiatric medication: for<br />
moderate to severe problems.<br />
Behavioural management techniques<br />
It is important to identify the reason or<br />
underlying cause that triggered the behaviour.<br />
Addressing the cause can <strong>of</strong>ten be the first<br />
step rather than targeting the behaviour.<br />
Part 1. Hangry = Hungry +Anger<br />
Don’t waste time trying to address<br />
behaviour until you get some calories into<br />
them first!<br />
More frequent (healthy) meals and snacks<br />
are advisable.<br />
Part 2. Models <strong>of</strong> behaviour<br />
The human brain is not fully developed<br />
until around 25 years <strong>of</strong> age. Part <strong>of</strong> growing<br />
up is to learn how to understand emotions<br />
and express them appropriately.<br />
• Traditional model <strong>of</strong> behaviour:<br />
Children engage in negative behaviour<br />
because they learn that they can get what<br />
they want if they act in a certain way.<br />
This behaviour is willful and intentional<br />
(manipulative!). Consistent discipline results<br />
in behaviour change.<br />
• Cognitive Deficit Model <strong>of</strong><br />
Behaviour:<br />
Children need to learn specific skills to<br />
manage and express their emotions and<br />
behaviours appropriately. These skills include:<br />
»» Cognitive flexibility;<br />
»» Frustration tolerance and delaying<br />
gratification;<br />
»» Problem solving;<br />
»» Anticipatory consequences;<br />
»» Expressing language;<br />
»» Social skills;<br />
»» <strong>In</strong>sight<br />
..... report continues on the facing page<br />
This report on Dr Poysky’s presentation will continue in the Spring <strong>2013</strong> edition<br />
<strong>of</strong> <strong>In</strong> <strong>Touch</strong> where information on ‘Where to start’ and some strategies on<br />
managing behaviour will be outlined.<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 30
Problems occur when demands <strong>of</strong> the<br />
situation exceed the child’s skills in these areas.<br />
The goal is not to punish the negative behaviours<br />
but to teach positive behaviours and the<br />
underlying skill.<br />
Deficits in cognitive skills can affect a person’s<br />
pattern <strong>of</strong> thinking, behaviour and response<br />
to certain situations. If a child has a weakness<br />
or developmental delay in their cognitive skills<br />
they may not pick up on parent threats and<br />
punishments leading to escalation. As a result<br />
they won’t learn from failure and may have<br />
difficulty making decisions not related to “right<br />
now”. Using punishment in these situations can<br />
escalate their behaviour and this pattern can lead to<br />
feelings <strong>of</strong> resentment for all involved.<br />
Rather than focus on the end result (behaviour)<br />
and forcing the child to obey it is better to recognise<br />
the underlying cause/weakness and help them to<br />
learn new skills. Focusing on the end result distracts<br />
from the main cause.<br />
Tapping into the underlying skills can help the<br />
child to readjust over time. It will not be instant and<br />
the model needs to be reinforced each time the child<br />
has learnt the necessary skill.<br />
The above images were sourced directly from Dr James Poysky’s conference<br />
presentation.<br />
Do you suffer from limited strength in your arms?<br />
Many have regained independence with a dynamic<br />
arm support system from Medifab.<br />
Elevation-assisted function allows far greater range <strong>of</strong> arm motion for<br />
increased functionality, independence, self-feeding and facial<br />
hygiene. Available for left or right arms and young children through<br />
to adults. Open up your life to higher achievement!<br />
Feed yourself again… <strong>In</strong>dependently<br />
Reduce fatigue and pain <strong>of</strong> the arm<br />
Strengthen your arm muscles<br />
Use a Keyboard to communicate again<br />
To view a video: scan the above QR code with your Smartphone<br />
and click ‘Media’ – or visit www.medifab.co.nz/multilink<br />
Contact the friendly team at Medifab today to chat about how your<br />
arm function can improve or arrange a FREE assessment trial.<br />
View this video online at: www.medifab.co.nz/multilink<br />
Call: 0800 543 343<br />
bruce@medifab.co.nz<br />
www.medifab.co.nz<br />
DO THINGS AGAIN<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 31<br />
you thought you never could…
Five years ago, effective treatment for<br />
DMD seemed an impossible dream, and few<br />
pharmaceutical companies were interested in<br />
investing in therapy for a fairly rare disease.<br />
However, this has all changed, as DMD is<br />
now seen as a model for the development<br />
<strong>of</strong> treatment on the basis <strong>of</strong> the specific<br />
mutation or mutations that are present in an<br />
individual (that is, personalised medicine), and<br />
advances in technology have made many <strong>of</strong><br />
the problems with therapeutic approaches<br />
more tractable. Many challenges remain,<br />
Research and relevance<br />
Clinical trials suggest great advances in future treatment<br />
<strong>of</strong> those with Duchenne muscular dystrophy<br />
however, not least for the development<br />
<strong>of</strong> reliable endpoints for clinical trials. The<br />
problem <strong>of</strong> delivery to all muscles <strong>of</strong> the body<br />
will also need to be resolved. However, there<br />
is little doubt that although a cure remains<br />
some way <strong>of</strong>f, treatments are currently<br />
entering trials that have the potential for<br />
providing a significant clinical impact on<br />
the quality <strong>of</strong> life <strong>of</strong> people with Duchenne<br />
muscular dysrtophy. <strong>In</strong> turn, these approaches<br />
are being applied to many other genetic<br />
disorders. The age <strong>of</strong> genomic medicine is<br />
moving forwards with rapid speed.<br />
Several promising genetic approaches,<br />
including viral delivery <strong>of</strong> the missing<br />
dystrophin gene, read-through <strong>of</strong> translation<br />
stop codons, exon skipping to restore the<br />
reading frame and increased expression <strong>of</strong> the<br />
compensatory utrophin gene are summarised<br />
in the below table, published in Nature<br />
Reviews Genetics June <strong>2013</strong> by Rebecca<br />
Fairclough, Matthew Wood and Kay Davies.<br />
The lessons learned from these approaches<br />
will be applicable to many other disorders.<br />
Drug name Description Company Delivery Route Results to date Current<br />
Stage<br />
Viral gene therapy<br />
Biostrophin<br />
rAAV2.5<br />
CMV minidystrophin<br />
(d3990)<br />
Termination codon read through<br />
Ataluren<br />
Nonsense<br />
suppression<br />
Exon skipping<br />
Eteplirsen (AVI<br />
4568)<br />
GSK2402968<br />
(PRO051);<br />
Drisapersen<br />
PRO044<br />
PMO<br />
morpholino<br />
targeting exon<br />
51<br />
2′OMePS<br />
AON targeting<br />
exon 51<br />
2′OMePS<br />
AON targeting<br />
exon 44<br />
Asklepios<br />
Biopharmaceutical<br />
<strong>In</strong>tramuscular<br />
injection<br />
(biceps)<br />
Failed to establish<br />
long-term<br />
dystrophin<br />
expression;<br />
immune response<br />
against transgene<br />
in 4 out <strong>of</strong> 6<br />
patients<br />
PTC Therapeutics Oral Slowed loss <strong>of</strong><br />
walking ability<br />
in patients with<br />
DMD or BMD (n =<br />
174) at the lower<br />
<strong>of</strong> two doses<br />
tested<br />
Sarepta<br />
Therapeutics<br />
Prosensa-<br />
GlaxoSmithKline<br />
Prosensa<br />
<strong>In</strong>travenous<br />
injection<br />
Subcutaneous<br />
injection<br />
Subcutaneous<br />
or intraveneous<br />
injection<br />
Well-tolerated<br />
and restored<br />
dystrophin<br />
expression in<br />
7 out <strong>of</strong> 19<br />
patients in a<br />
dose-dependent<br />
manner (
TA <strong>In</strong>door independence indoors like never before<br />
A powerchair with standard hilow function. Reach higher in the kitchen while sitting very low under a table or<br />
desk. The TA <strong>In</strong>door has a small base, only 56cm wide, 69.5cm long. This ensures narrow doorways and turning<br />
in bathrooms is easier. No need to worry about costly modifications to doorways, walls, and living spaces.<br />
See our website for videos and brochures: www.mortonperry.co.nz/TA-<strong>In</strong>door-Powerchair.html<br />
Sit, Stand & Transfer more safely with TA<br />
Trusted and proven over the last 10 years in <strong>New</strong> Zealand for their function, durability, and reliability. Vertical<br />
lift for safer and easier self or assisted transfers.<br />
Toilet Lifter<br />
Robust, stainless steel.<br />
Easy to clean.<br />
Shower and Toilet Lifter<br />
Waterpro<strong>of</strong>.<br />
Portable on wheels.<br />
Living and Office Chair<br />
Hilow with 360˚ swivel<br />
and brake<br />
Ask your therapist to specify TA. Available for Ministry <strong>of</strong> Health funded trials.<br />
0800 238 423 www.mortonperry.co.nz advice@mortonperry.co.nz
At ease<br />
Ben Robertson shares his views on<br />
life, opportunity and finding peace<br />
I wrote recently about Oscar Pistorius – the<br />
South African Olympian who broke all sorts <strong>of</strong><br />
barriers by competing at the London Olympics<br />
despite his disability. I thought this man was great, a role model for<br />
us all. Well it may not be that cut and dried because, shortly after the<br />
Olympics, he was back in the headlines, not for something incredible<br />
or inspiring but because he has been charged with the murder <strong>of</strong> his<br />
girlfriend.<br />
The case is set to be heard in June <strong>of</strong> this year but Pistorius <strong>of</strong>fers<br />
no defence for the shooting. He has admitted that he shot four times<br />
at someone, connecting three times and fatally wounding them. He<br />
claims that he thought that the person inside the bathroom was an<br />
intruder and only later found out that it was actually his girlfriend.<br />
Public opinion <strong>of</strong> Pistorius, which has been created by the media, is<br />
good but some believe him to be a loose cannon. It is claimed that he<br />
always carried a gun on him, applied to have more than the four-gun<br />
legal limit and is quick to anger.<br />
Jeopardising the good publicity he brought<br />
to disabled people Pistorius may well have<br />
reinforced a negative stereotype <strong>of</strong> disabled<br />
people – that <strong>of</strong> the disabled person as one that is inherently evil.<br />
Often disability is used to connote this in movies, a limp, a hook<br />
for a hand, a patch over the eye or a hunchback are some common<br />
examples but more examples <strong>of</strong> this stereotype are not hard to find. <strong>In</strong><br />
movies like Forest Gump this stereotype is used to create an ‘othering’<br />
effect. The disabled community have perhaps been beginning to<br />
redress the effects <strong>of</strong> this stereotype but Pistorius’ efforts have done<br />
us a huge disservice.<br />
Perhaps he will be acquitted in June. He has been competing at<br />
track meets all over the world because he has been deemed to be a<br />
non-flight risk; I don’t know why, if I was guilty I would sure want to<br />
flee – disability or not. Maybe this indicates that he is not guilty. Either<br />
way Pistorius’ girlfriend <strong>of</strong> three months, promising model and law<br />
graduate, Reeva Steenkamp lies dead. I guess we will never truly know<br />
if this was Pistorius’ intention or not.<br />
THREE REASONS WHY YOU WILL LOVE VILLAGE LIFE<br />
location<br />
LOCATION ONE<br />
Russley Village in Christchurch<br />
Gracious botanic splendour in the Garden City.<br />
The individual design and facilities continuing<br />
the spirit and hospitality <strong>of</strong> Christchurch’s old<br />
Russley Hotel never fail to impress visitors.<br />
Another icon in the making.<br />
location<br />
location<br />
UNDER CONSTRUCTION<br />
avoid this kind oF pressure ulcer<br />
russleyvillage.co.nz<br />
LOCATION TWO<br />
Pacific Coast Village in Papamoa<br />
Finally you can experience the Gold Coast lifestyle<br />
without leaving home. Year-round resort living<br />
across from a beautiful white sand beach. Stroll<br />
the boardwalk in the morning, go bowling in the<br />
afternoon, and finish with a barbecue at your<br />
beautifully designed Summerhouse.<br />
pacificcoastvillage.co.nz<br />
LOCATION THREE<br />
Ranfurly Village in Auckland<br />
Over 100 years <strong>of</strong> heritage combined with<br />
brand new facilities makes this central Auckland<br />
location unbeatable. Physio and OT are<br />
already on site, an aged care facility is under<br />
construction, and apartments are available at<br />
pre-construction prices now.<br />
ranfurlyvillage.co.nz<br />
<strong>In</strong>dividually crafted to recognize the characteristics <strong>of</strong> each location, Retirement<br />
Assets Villages <strong>of</strong>fer a truly unique retirement lifestyle. Our residents enjoy a<br />
level <strong>of</strong> elegance matched only by the security, care and respect they deserve.<br />
And as a company we’re proud to extend that care further, by supporting the<br />
<strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong> <strong>of</strong> NZ. 0800 22 44 88
NZ NMD Registry update<br />
The NZ NMD Registry is the only one <strong>of</strong> its kind in <strong>New</strong> Zealand<br />
and its model is unlike any other in the world which does make it<br />
difficult for us to compare just how well we are doing. However, at a<br />
recent meeting in Australia, Hugh Dawkins from the Western Australia<br />
Department <strong>of</strong> Health Office for Population Health and Genomics<br />
provided an update on the Australia and NZ Duchenne muscular<br />
dystrophy registries. He outlined the formation <strong>of</strong> the Australian DMD<br />
registry and then the subsequent involvement <strong>of</strong> NZ’s MDA and the<br />
formation <strong>of</strong> the Rare Disease Registries programme.<br />
Current registrations show that some states in Australia are<br />
experiencing difficulties in getting their patients enrolled and most<br />
cited a lack <strong>of</strong> human resource as the reason for this.<br />
Overall, 67% have genetic data, 60% have complete clinical<br />
data, 9% have partial clinical data and 31% contain no clinical data,<br />
however <strong>of</strong> the NZ enrolments 75% have genetic data and 93% have<br />
complete clinical data.<br />
<strong>New</strong> Zealand is currently the only jurisdiction to have registrations<br />
in the SMA database, also housed with the Office for Population<br />
Health and Genomics, totalling 21. As you can see we are measuring<br />
up quite well against the Australian states!<br />
Of course the NZ NMD Registry is about more than Duchenne<br />
muscular dystrophy and spinal muscular atrophy. We have over<br />
360 participants enrolled with the registry with a broad range <strong>of</strong><br />
neuromuscular disorders including inherited neuropathies such as<br />
Charcot-Marie-Tooth disease, muscular dystrophies, spinal muscular<br />
atrophies, inflammatory myopathies, inherited ataxias, myasthenic<br />
syndromes and others. There is strength in<br />
numbers so if you are interested in enrolling<br />
with the NZ NMD Registry then talk to your<br />
MDA fieldworker or email registry@mda.<br />
org.nz.<br />
NZNMD Registry Curator,<br />
Miriam Rodrigues<br />
complex seating solutions<br />
For those individuals with limited movement there is an increased<br />
risk <strong>of</strong> developing an unconventional body shape and therefore<br />
if assistance can be provided to manage posture through a multipositional<br />
seating system then the risk can be significantly reduced.<br />
Duo MAJoR<br />
The Duo’s purpose is to provide the ultimate in<br />
positioning and postural management for those<br />
who are unable to maintain their body posture and<br />
require extra support.<br />
The Duo range provides flexible adjustment and Duo M<strong>In</strong>I<br />
positioning opportunities with the choice <strong>of</strong> either<br />
manual gas action or electrically powered tilt-in-space and leg-rest elevation<br />
or indeed the option <strong>of</strong> Regulated Motion where the tilt-in-space movement<br />
continually changes.<br />
Furthermore the Duo range now has the option <strong>of</strong> different pressure relieving seat modules depending on<br />
individual user’s pressure management requirements. From the highly advanced <strong>In</strong>telli-Gel seat module for<br />
those at very high risk <strong>of</strong> developing pressure problems through to the Transflo Gel cushion and Reflexion<br />
foam seat modules for those at medium to high risk. <strong>In</strong>deed the flexibility <strong>of</strong> the Duo range as with the<br />
majority <strong>of</strong> the specialist seating portfolio enables users to either integrate their own pressure relieving seat<br />
cushion into the seat module <strong>of</strong> the chair or apply a flat seat board upon which it can be effectively used.<br />
Chair adjustments include:<br />
l Tilt-in-space and leg-rest<br />
elevation<br />
l Seat height adjustment<br />
l Back angle recline<br />
l Back height adjustment<br />
l Variable seat length and<br />
width<br />
l Adjustable arm height<br />
l Headrest angle<br />
adjustment<br />
l Removable arms for side<br />
transfer<br />
l Height adjustable,<br />
integrated flip-up<br />
footboard<br />
Accessories: Lateral<br />
supports, leg-laterals,<br />
pommel, leg-rest bracket<br />
to achieve a 25% negative<br />
angle, flat seat board, pelvic<br />
positioners, lap belt, tray.<br />
Funding may be available or the chair can be purchased direct<br />
Phone 0800-330 331 or email don@wsmedical.co.nz<br />
Website www.wsmedical.co.nz
GenY ine issue<br />
As promised with this article, I have included a photograph<br />
<strong>of</strong> my family’s adventure to Rabbit Island with Mum’s new<br />
beach wheelchair. It was such fun, everybody needs one!<br />
Since then, I have returned to Wellington and am now in<br />
my third year <strong>of</strong> university. <strong>In</strong> fact, my first semester is over at<br />
the end <strong>of</strong> this month, and I’ve got some big news. I have to<br />
wait for my visa to be confirmed, but it seems that I will be<br />
moving abroad for my second semester. I have been accepted<br />
into my university’s exchange programme with California<br />
State University!<br />
I’ve been to California before, with Koru Care, however<br />
actually moving there, knowing nobody at all, seems exciting,<br />
daunting and completely crazy all at the same time.<br />
One thing that makes it rather scary is the fact that I have<br />
a disability and a wheelchair. Of course, the two go hand in<br />
hand, but I’m a little worried about them separately.<br />
My condition means that I have trouble with stairs and<br />
walking long distances, but I’m not too concerned about<br />
it because the States has a law requiring all buildings to<br />
have disabled access. Honestly, I’m more worried about<br />
my wheelchair. Of all the things to worry about most, the<br />
wheelchair seems silly. After all, it is the thing that gives me so<br />
much freedom and in many ways takes away my disability. But<br />
I think that that’s the reason why I am so concerned about it.<br />
If it gets a flat tire or breaks or gets stolen, it’s going<br />
to be so much more difficult to resolve on the other<br />
side <strong>of</strong> the world. I can’t simply call my local wheelchair<br />
repair guy (yes, I do have one). I guess I never really<br />
considered how much I truly relied on my wheelchair. Even<br />
though I don’t use it inside buildings, outdoors it functions<br />
as my legs. So the thought <strong>of</strong> losing my ‘legs’ in America,<br />
although it sounds comical, is actually pretty scary.<br />
With that slightly worried note, I must say that I do have<br />
great faith in the goodness <strong>of</strong> people, so any concerns I have<br />
are diminished when I remember that. If something drastic<br />
does happen, I’m sure somebody will help me out.<br />
When I’m in the ‘land <strong>of</strong> opportunity’ I definitely plan on<br />
visiting the MDA over there, to gain some new ideas for the<br />
youth here.<br />
Currently myself and another youth member are organising<br />
a Wellington meet up for younger members aged between<br />
15-30 to be held soon. So if you’d like to be a part <strong>of</strong> that, to<br />
meet up with us and MDA youths for a casual dinner, do get<br />
in contact. We’d love to have as many people as we can come<br />
along. If you’re interested, contact me at shchristie@live.com<br />
or add me on Facebook http://www.facebook.com/stacey.<br />
christie.16<br />
Stacey Christie,<br />
MDA Young (Rangatahi) Representative<br />
Stacey’s parents, Delwyn and Donald Christie, try out the<br />
new beach wheelchair at Rabbit Island this past summer.<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 36
Legally mindful<br />
Dr Huhana Hickey is an education and law reform<br />
solicitor with recent experience at Auckland Disability<br />
Law (ADL), a community law centre service that aims to meet the unmet legal needs<br />
<strong>of</strong> Aucklanders with disabilities.<br />
Huhana has direct experience in issues relating to disability. She was the sole<br />
solicitor with ADL until February this year when she took on a new part-time role in<br />
education and law reform to try and concentrate on the legal issues rather than the<br />
case law for Aucklanders with disabilities.<br />
Article 13 - Access to justice<br />
I am sure we all believe we have access to justice? Well, some more than others; the good<br />
news is the UN Convention on the Rights <strong>of</strong> Persons with Disabilities outlines how we can get<br />
access to justice. The article states:<br />
1. Parties shall ensure effective access to justice for persons with<br />
disabilities on an equal basis with others, including through the<br />
provision <strong>of</strong> procedural and age-appropriate accommodations, in<br />
order to facilitate their effective role as direct and indirect participants,<br />
including as witnesses, in all legal proceedings, including at<br />
investigative and other preliminary stages.<br />
2. <strong>In</strong> order to help to ensure effective access to justice for persons<br />
with disabilities, States Parties shall promote appropriate training for<br />
those working in the field <strong>of</strong> administration <strong>of</strong> justice, including police<br />
and prison staff.<br />
Article number 1 simply means you have the right to access justice<br />
the same as everyone else and in a way that you can understand.<br />
If you are learning disabled, the courts have to accommodate your<br />
need so you can understand the process whether you are a witness,<br />
or another member <strong>of</strong> the legal issue. This means you cannot be<br />
discriminated against because you have a disability and therefore<br />
if you have a legal issue you are entitled to have all the legal help<br />
and support you need. This includes the police, lawyers, judges and<br />
everyone who you are involved with when addressing any legal issues.<br />
Article number 2 is where the Government will promote training<br />
for the lawyers, judges, the police and anyone else involved in legal<br />
work, even prison staff. This is possibly easier said than done as until<br />
the Government promotes training at the undergraduate level <strong>of</strong><br />
lawyers, judges, the police and prison staff then the training they get<br />
will only have a limited impact.<br />
What can we do about this? Now you know you have rights, you<br />
can say you are entitled and fight for those rights. For instance if<br />
you are a victim <strong>of</strong> a crime and insist on having justice served, then<br />
if you can’t argue your case verbally you can then insist upon using a<br />
computer or an interpreter for your voice so you can see justice served.<br />
The justice system cannot deny you that right. If you have a family<br />
member who is learning disabled and unable to speak their complaint,<br />
then you can fight for their right to have their case taken up by the<br />
police etc.<br />
We have rights and no one can remove those rights from us. I insist<br />
you use your rights for any injustice you experience. If you need help<br />
and support for your case, then go to your local community law centre<br />
who will assist you or if you are based in Auckland you can go to see<br />
Auckland Disability Law at info@adl.org.nz or phone 2575140 and ask<br />
if you can speak to a lawyer. Remember you do have rights.<br />
Next time we will be looking at Article 14 – Liberty and security<br />
<strong>of</strong> person. Until then be well and know your rights are there through<br />
the UN Convention on the Rights <strong>of</strong> Persons with Disabilities and our<br />
domestic law.<br />
Dr Huhana Hickey<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 37
CONDITIONS COVERED BY MDA<br />
MUSCULAR DYSTROPHIES:<br />
• Duchenne <strong>Muscular</strong><br />
<strong>Dystrophy</strong><br />
• Becker <strong>Muscular</strong> <strong>Dystrophy</strong><br />
• Manifesting carrier <strong>of</strong><br />
<strong>Muscular</strong> <strong>Dystrophy</strong><br />
• Emery-Dreifuss <strong>Muscular</strong><br />
<strong>Dystrophy</strong><br />
• Limb-Girdle <strong>Muscular</strong><br />
<strong>Dystrophy</strong><br />
• Facioscapulohumeral<br />
<strong>Muscular</strong> <strong>Dystrophy</strong><br />
• Myotonic <strong>Dystrophy</strong><br />
• Oculopharyngeal <strong>Muscular</strong><br />
<strong>Dystrophy</strong><br />
• Distal <strong>Muscular</strong> <strong>Dystrophy</strong><br />
• Congenital <strong>Muscular</strong><br />
Dystrophies and Congenital<br />
Myopathies<br />
METABOLIC DISEASES OF MUSCLE<br />
- all types including:<br />
• Phosphorylase Deficiency<br />
(also known as McArdle’s<br />
Disease)<br />
• Acid Maltase Deficiency<br />
(also known as Pompe’s<br />
Disease)<br />
• Phosph<strong>of</strong>ructokinase<br />
Deficiency (also known as<br />
Tarui’s Disease)<br />
• Debrancher Enzyme<br />
Deficiency (also known as<br />
Cori’s or Forbes’ Disease)<br />
• Mitochondrial Myopathy<br />
(including MELAS, MERRF,<br />
NARP and MIDD)<br />
DISEASES OF THE MOTOR<br />
NEURONS:<br />
• Spinal <strong>Muscular</strong> Atrophy -<br />
all types including Type<br />
1 <strong>In</strong>fantile Progressive<br />
Spinal <strong>Muscular</strong> Atrophy<br />
(also known as Werdnig<br />
H<strong>of</strong>fman Disease)<br />
• Type 2 <strong>In</strong>termediate Spinal<br />
<strong>Muscular</strong> Atrophy<br />
• Type 3 Juvenile Spinal<br />
<strong>Muscular</strong> Atrophy<br />
(Kugelberg Welander<br />
Disease)<br />
• Type 4 Adult Spinal<br />
<strong>Muscular</strong> Atrophy<br />
• Spinal Bulbar <strong>Muscular</strong><br />
Atrophy (Kennedy’s Disease<br />
and X-Linked SBMA)<br />
DISEASES OF PERIPHERAL NERVE:<br />
• Charcot-Marie-Tooth<br />
Disease (CMT) (Hereditary<br />
Motor and Sensory<br />
Neuropathy) - all types<br />
• Dejerine-Sottas Disease<br />
(CMT Type 3)<br />
• Hereditary Sensory<br />
Neuropathy<br />
INFLAMMATORY MYOPATHIES:<br />
• Dermatomyositis<br />
• Polymyositis<br />
• <strong>In</strong>clusion Body Myositis<br />
Should you have a query<br />
regarding a condition<br />
not listed please contact<br />
Claudine on (09) 815 0247,<br />
0800 800 337 or email<br />
Claudine@mda.org.nz<br />
DISEASES OF THE<br />
NEUROMUSCULAR<br />
JUNCTION:<br />
• Myasthenia Gravis<br />
• Lambert-Eaton Syndrome<br />
• Congenital Myasthenic<br />
Syndrome<br />
MYOPATHIES - all types:<br />
• Myotonia Congenita (Two<br />
forms: Thomsen’s and<br />
Becker’s Disease)<br />
• Paramyotonia Congenita<br />
• Central Core Disease<br />
• Nemaline Myopathy<br />
• Myotubular Myopathy<br />
• <strong>In</strong>clusion Body Myopathy<br />
• Periodic Paralysis<br />
• ` Andersen-Tawil Syndrome<br />
• Hyperthyroid Myopathy<br />
• Hypothyroid Myopathy<br />
INHERITED ATAXIAS<br />
• Friedreich Ataxia (FA)<br />
• Spinocerebellar Ataxia<br />
(SCA)<br />
HEREDITARY SPASTIC<br />
PARAPLEGIAS - all types - (HSP)<br />
(also called Familial Spastic<br />
Paraparesis)<br />
LEUCODYSTROPHIES - all types<br />
PHAKOMATOSES<br />
(conditions affecting the brain and<br />
the skin)<br />
• Neur<strong>of</strong>ibromatosis<br />
Types 1<br />
in touch // <strong>Winter</strong> <strong>2013</strong> // PAGE 38
YES, I would like to help.<br />
Please accept my donation.<br />
Please charge my credit card:<br />
Visa Mastercard Other<br />
Credit Card No:<br />
Name on Credit Card ....................................................................................................................<br />
Expiry Date:<br />
Signature...............................................................................<br />
Or enclosed is my cheque<br />
Your name ................................................................. Mailing address ...........................................................<br />
.........................................................................................................................................................................................<br />
The privacy act 1993 requires us to advise you that your private details are held in our records for our purposes only, but should you wish us not to do<br />
so at any time you may advise us <strong>of</strong> this.<br />
Or to make an online donation go to www.mda.org.nz<br />
Return to: <strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong> NZ <strong>In</strong>c.<br />
PO Box 120663, Penrose, Auckland 1642, <strong>New</strong> Zealand.<br />
Others ways to donate:<br />
- You can call 0900 426 98 to make an automatic $15 donation via your phonebill<br />
- Donate an amount <strong>of</strong> your choice securely online at www.mda.org.nz<br />
You can also donate via Payroll Giving<br />
Payroll giving is a really easy way to make regular donations to the MDA while also helping you to reduce your<br />
PAYE tax. For example a donation <strong>of</strong> $20 earns $6.66 in tax credits that is taken <strong>of</strong>f your PAYE, so MDA receives<br />
$20 and you keep $6.66. All you need to give your employer is our name, the amount you wish to donate and<br />
our bank account number. For more information contact us.<br />
To make a bequest to the MDA<br />
You may be thinking <strong>of</strong> making a will and may wish to include the MDA as a beneficiary. If so we suggest the<br />
following as an option for inclusion in your will:<br />
“I give and bequest to: <strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong> <strong>of</strong> NZ <strong>In</strong>c. …………% <strong>of</strong> my estate, or the sum <strong>of</strong><br />
$......... for the general purposes <strong>of</strong> the <strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong>, I declare that the receipt <strong>of</strong> an <strong>of</strong>ficer <strong>of</strong><br />
<strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong> shall be a full and sufficient discharge <strong>of</strong> my trustee”.<br />
THANK YOU FOR YOUR SUPPORT<br />
Charities Commission Registration CC31123<br />
IN <strong>Touch</strong> // <strong>Winter</strong> <strong>2013</strong> // PAGE 39
It might be you .....<br />
or a family member, a neighbour or a friend.<br />
It could be a wee baby, or a retiree, and could happen at any<br />
stage in life.<br />
Muscle weakness and wasting conditions can strike anyone <strong>of</strong><br />
any age, <strong>of</strong> any ethnicity.<br />
These disabling conditions are called neuromuscular conditions<br />
with most but not all being genetic in origin.<br />
<strong>Muscular</strong> <strong>Dystrophy</strong> <strong>Association</strong> Patron,<br />
Judy Bailey.<br />
We provide services to people with<br />
neuromuscular conditions - services that help<br />
them lead full lives<br />
You can help by<br />
• Telling family members affected by a<br />
neuromuscular condition about us<br />
• Supporting our fundraising efforts<br />
PO Box 120663, Penrose, 1642, Auckland Ph 09 815 0247 / 0800 800 337 www.mda.org.nz