Adaptive Licensing: a useful approach for drug licensing in ... - TOPRA
Adaptive Licensing: a useful approach for drug licensing in ... - TOPRA
Adaptive Licensing: a useful approach for drug licensing in ... - TOPRA

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Adaptive</strong> <strong>Licens<strong>in</strong>g</strong>:<br />
a <strong>useful</strong> <strong>approach</strong> <strong>for</strong><br />
<strong>drug</strong> <strong>licens<strong>in</strong>g</strong> <strong>in</strong> the EU?<br />
London, <strong>TOPRA</strong>,<br />
November 2012<br />
Hans-Georg Eichler<br />
An agency of the European Union
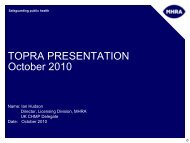
‘Eroom’s Law’: The number of<br />
new <strong>drug</strong>s approved by the FDA<br />
per billion dollars (<strong>in</strong>flationadjusted)<br />
spent on R&D has<br />
halved roughly every 9 years<br />
Scannell JW et al. Nature Rev Drug Disc, March 2012<br />
2
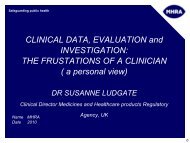
Trend <strong>in</strong> actual cl<strong>in</strong>ical development time <strong>for</strong> new development projects<br />
approved between 2000-2009<br />
Median<br />
12<br />
11<br />
10<br />
9<br />
8<br />
7<br />
6<br />
5<br />
4<br />
3<br />
2<br />
1<br />
n of <strong>in</strong>terventions/trial patient<br />
n of patients/trial<br />
n of trials/dossier<br />
0<br />
2000(15)<br />
2001(20)<br />
2002(17)<br />
2003(10)<br />
2004(8)<br />
2005(11)<br />
2006(12)<br />
2007(7)<br />
2008(11)<br />
2009(12)<br />
Year of approval<br />
Actual cl<strong>in</strong>ical development time is calculated <strong>for</strong> new development projects as the time between ‘First human dose’ (T-1-1) and ‘First approval’ (T-4-2). Data<br />
represent all new development projects that reached ‘First approval’ (T-4-2) between 2000-2009, where the start and end milestone dates <strong>for</strong> the <strong>in</strong>terval are<br />
available. (n) = number of projects analysed <strong>in</strong> each year. This analysis is based on data from a consistent cohort of 17 companies participat<strong>in</strong>g each year<br />
between 2001 and 2010.<br />
3<br />
© CMR International, a Thomson Reuters bus<strong>in</strong>ess
Evolution of life<br />
Mutation<br />
Selection<br />
Evolution of <strong>drug</strong> regulation<br />
Catastrophe<br />
Clamp Down<br />
4
Knowledge, <strong>in</strong>vestment<br />
The b<strong>in</strong>ary nature of<br />
<strong>drug</strong> regulation<br />
Current model of <strong>licens<strong>in</strong>g</strong><br />
“The Magic Moment”<br />
Evidence vs. access trade-off<br />
Time (years)<br />
5
The regulator’s dilemma<br />
“…it has been said that the FDA has<br />
just two speeds of [<strong>drug</strong>] approval –<br />
too fast and too slow.”<br />
Hamburg MA & Sharfste<strong>in</strong> JM. NEJM 360;24: 2493-5; 2009<br />
6
EMA Road map to 2015<br />
[…] a key issue <strong>for</strong> regulators will be whether a<br />
more ‘staggered‘ approval (or progressive<br />
<strong>licens<strong>in</strong>g</strong>) concept should be envisaged <strong>for</strong><br />
situations not covered by conditional<br />
market<strong>in</strong>g authorisations […]<br />
The Agency would like to launch a debate with<br />
all stakeholders on the appropriateness of<br />
<strong>in</strong>troduc<strong>in</strong>g such a concept, <strong>in</strong>clud<strong>in</strong>g a<br />
consideration of appropriate <strong>in</strong>centives to<br />
support new medic<strong>in</strong>es development.<br />
7
Different names, same ideas<br />
• EMA: staggered approval<br />
• FDA: progressive reduction of uncerta<strong>in</strong>ty<br />
• Health Canada: progressive authorization<br />
• HSA S<strong>in</strong>gapore: test bed <strong>for</strong> adaptive regulation<br />
• Payers (HTAi): managed entry<br />
• MIT/NEWDIGS: adaptive <strong>licens<strong>in</strong>g</strong> project<br />
8
NEWDIGS - Collaborators<br />
(NEW Drug Development ParaDIGmS)<br />
Pharma/Biotech Regulators Academia Payers<br />
AstraZeneca<br />
BMS<br />
GSK<br />
J&J<br />
Novartis<br />
Pfizer<br />
Qu<strong>in</strong>tiles<br />
Sanofi-aventis<br />
FDA<br />
EMA<br />
HSA (S<strong>in</strong>gapore)<br />
HealthCanada<br />
SwissMedic<br />
MIT<br />
Harvard<br />
Sloan –Ketter<strong>in</strong>g<br />
MGH/Partners<br />
Dana Farber<br />
Natl U of S<strong>in</strong>gapore<br />
Aetna<br />
Medco<br />
Wellpo<strong>in</strong>t<br />
NICE<br />
9
Cl<strong>in</strong>ical Pharmacology & Therapeutics (2012); 91 3, 426–437<br />
10
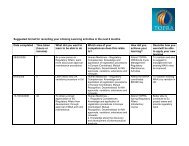
Millions<br />
Gilenya Case Study Results<br />
11<br />
• <strong>Adaptive</strong> <strong>approach</strong> <strong>in</strong>creases NPV<br />
NPV<br />
eNPV<br />
Real $ 1,440,469,095 $ 325,180,180<br />
<strong>Adaptive</strong> $ 2,116,101,362 $ 378,517,356<br />
Gilenya NPVs by Scenario<br />
$2,000<br />
$1,800<br />
$1,600<br />
$1,400<br />
$1,200<br />
$1,000<br />
$800<br />
$600<br />
$400<br />
$200<br />
$-<br />
$1,440<br />
NPV<br />
$1,794<br />
$325<br />
eNPV<br />
$379<br />
Historic<br />
<strong>Adaptive</strong><br />
<strong>Adaptive</strong> <strong>Licens<strong>in</strong>g</strong> Economics<br />
December 2011
Knowledge, <strong>in</strong>vestment<br />
A better model <strong>for</strong> evolution?<br />
Current model of <strong>licens<strong>in</strong>g</strong><br />
“The Magic Moment”<br />
<strong>Adaptive</strong><br />
<strong>Licens<strong>in</strong>g</strong><br />
Time (years)<br />
12
<strong>Adaptive</strong> <strong>Licens<strong>in</strong>g</strong><br />
AL is a prospectively planned, adaptive <strong>approach</strong><br />
to regulation of <strong>drug</strong>s.<br />
Through iterative phases of evidence gather<strong>in</strong>g<br />
followed by regulatory evaluation and license<br />
adaptation,<br />
AL seeks to maximize the positive impact of new<br />
<strong>drug</strong>s on public health<br />
by balanc<strong>in</strong>g timely access <strong>for</strong> patients with the<br />
need to provide adequate evolv<strong>in</strong>g <strong>in</strong><strong>for</strong>mation<br />
on benefits and harms.<br />
13
<strong>Adaptive</strong> <strong>Licens<strong>in</strong>g</strong><br />
AL builds on exist<strong>in</strong>g regulatory processes,<br />
<strong>in</strong>clud<strong>in</strong>g Conditional Authorization and<br />
exist<strong>in</strong>g PhV tools.<br />
To achieve the full potential of AL, <strong>licens<strong>in</strong>g</strong><br />
decisions should ideally be aligned with<br />
coverage and prescribers’ decisions.<br />
14
“Precursors” to<br />
<strong>Adaptive</strong> <strong>Licens<strong>in</strong>g</strong><br />
• Conditional Market<strong>in</strong>g Authorization<br />
• New Pharmacovigilance legislation<br />
• Risk Management Plans<br />
• Periodic Safety Update Reports<br />
• Five-year renewal of market<strong>in</strong>g authorization<br />
• (Compassionate use programs)<br />
15
<strong>Adaptive</strong> <strong>Licens<strong>in</strong>g</strong><br />
AL builds on exist<strong>in</strong>g regulatory processes,<br />
<strong>in</strong>clud<strong>in</strong>g Conditional Authorization and<br />
exist<strong>in</strong>g PhV tools.<br />
To achieve the full potential of AL, <strong>licens<strong>in</strong>g</strong><br />
decisions should ideally be aligned with<br />
coverage and prescribers’ decisions.<br />
16
<strong>Adaptive</strong> <strong>Licens<strong>in</strong>g</strong> – a ‘systems <strong>approach</strong>’<br />
Regulatory<br />
Agency<br />
Payer / HTA<br />
body<br />
Prescriber<br />
Patient as<br />
payer<br />
Drug<br />
candidates<br />
Market and<br />
patient<br />
access<br />
Does the <strong>drug</strong><br />
do more good<br />
than harm <strong>in</strong> a<br />
def<strong>in</strong>ed group<br />
of patients?<br />
What are the<br />
health and cost<br />
consequences<br />
associated with<br />
this <strong>drug</strong><br />
relative to other<br />
<strong>in</strong>terventions?<br />
How does the<br />
<strong>drug</strong> per<strong>for</strong>m<br />
relative to other<br />
<strong>in</strong>terventions <strong>in</strong><br />
this patient?<br />
Am I will<strong>in</strong>g and<br />
able to pay <strong>for</strong><br />
this treatment<br />
out-of-pocket?<br />
Eichler et al, Nature Rev Drug Disc, 2010<br />
17
AL scenarios – “design factors”<br />
Incremental vs. trans<strong>for</strong>mative <strong>approach</strong>es<br />
• broaden treatment-eligible population<br />
• reduce uncerta<strong>in</strong>ty around endpo<strong>in</strong>t<br />
• reduce uncerta<strong>in</strong>ty around study design<br />
• reduce statistical uncerta<strong>in</strong>ty<br />
• enable new-new combo development<br />
• ensure effectiveness<br />
• address rare Adverse Events<br />
18
The O2 problem<br />
Obstacles and Opportunities<br />
• Not just focus on front end (<strong>in</strong>itial <strong>licens<strong>in</strong>g</strong>)<br />
• Make the ’systems <strong>approach</strong>’ work<br />
• Rapid learn<strong>in</strong>g systems<br />
• Cont<strong>in</strong>ual optimisation of <strong>drug</strong> use<br />
19
Conclusions?<br />
• Not a panacea, not necessarily a route <strong>for</strong> all<br />
<strong>drug</strong>s, one size doesn't fit all,<br />
• but might help regulators avoid the<br />
reputation trap (“too fast and too slow”),<br />
• if properly managed and communicated,<br />
might be the best (or only?) option to<br />
balance the access and evidence.<br />
20
Thank you!<br />
21