

January/February - West Virginia State Medical Association
January/February - West Virginia State Medical Association
January/February - West Virginia State Medical Association

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Scientific Article |<br />
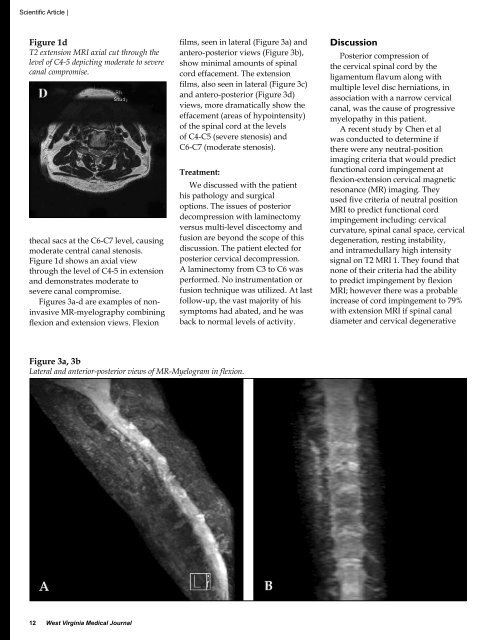
Figure 1d<br />
T2 extension MRI axial cut through the<br />
level of C4-5 depicting moderate to severe<br />
canal compromise.<br />
thecal sacs at the C6-C7 level, causing<br />
moderate central canal stenosis.<br />
Figure 1d shows an axial view<br />
through the level of C4-5 in extension<br />
and demonstrates moderate to<br />
severe canal compromise.<br />
Figures 3a-d are examples of noninvasive<br />
MR-myelography combining<br />
flexion and extension views. Flexion<br />
films, seen in lateral (Figure 3a) and<br />
antero-posterior views (Figure 3b),<br />
show minimal amounts of spinal<br />
cord effacement. The extension<br />
films, also seen in lateral (Figure 3c)<br />
and antero-posterior (Figure 3d)<br />
views, more dramatically show the<br />
effacement (areas of hypointensity)<br />
of the spinal cord at the levels<br />
of C4-C5 (severe stenosis) and<br />
C6-C7 (moderate stenosis).<br />
Treatment:<br />
We discussed with the patient<br />
his pathology and surgical<br />
options. The issues of posterior<br />
decompression with laminectomy<br />
versus multi-level discectomy and<br />
fusion are beyond the scope of this<br />
discussion. The patient elected for<br />
posterior cervical decompression.<br />
A laminectomy from C3 to C6 was<br />
performed. No instrumentation or<br />
fusion technique was utilized. At last<br />
follow-up, the vast majority of his<br />
symptoms had abated, and he was<br />
back to normal levels of activity.<br />
Discussion<br />
Posterior compression of<br />
the cervical spinal cord by the<br />
ligamentum flavum along with<br />
multiple level disc herniations, in<br />
association with a narrow cervical<br />
canal, was the cause of progressive<br />
myelopathy in this patient.<br />
A recent study by Chen et al<br />
was conducted to determine if<br />
there were any neutral-position<br />
imaging criteria that would predict<br />
functional cord impingement at<br />
flexion-extension cervical magnetic<br />
resonance (MR) imaging. They<br />
used five criteria of neutral position<br />
MRI to predict functional cord<br />
impingement including: cervical<br />
curvature, spinal canal space, cervical<br />
degeneration, resting instability,<br />
and intramedullary high intensity<br />
signal on T2 MRI 1. They found that<br />
none of their criteria had the ability<br />
to predict impingement by flexion<br />
MRI; however there was a probable<br />
increase of cord impingement to 79%<br />
with extension MRI if spinal canal<br />
diameter and cervical degenerative<br />
Figure 3a, 3b<br />
Lateral and anterior-posterior views of MR-Myelogram in flexion.<br />
12 <strong>West</strong> <strong>Virginia</strong> <strong>Medical</strong> Journal












