Is treating Blood pressure alone enough to protect your
Is treating Blood pressure alone enough to protect your
Is treating Blood pressure alone enough to protect your

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
The challenge of <strong>protect</strong>ion in<br />
hypertensive patients<br />
Magdy Rashwan, MD<br />
Professor of cardiology<br />
University of Alexandria<br />
Egypt
<strong>Is</strong> <strong>treating</strong> <strong>Blood</strong> <strong>pressure</strong> <strong>alone</strong> <strong>enough</strong> <strong>to</strong> <strong>protect</strong> <strong>your</strong><br />
hypertensive patient?<br />
Does the elevation of blood <strong>pressure</strong> increase the atherogenecity<br />
of cholesterol-rich lipoproteins ?<br />
Want <strong>to</strong> go beyond blood <strong>pressure</strong> in patients with hypertension?<br />
EBM.<br />
<strong>Is</strong> it just an antihypertensive treatment + statin?<br />
Who are those hypertensive patients at high CVD risk?<br />
Conclusion.<br />
<strong>Is</strong> <strong>treating</strong> <strong>Blood</strong> <strong>pressure</strong> <strong>alone</strong> <strong>enough</strong> <strong>to</strong> <strong>protect</strong> <strong>your</strong><br />
hypertensive patient?<br />
Does the elevation of blood <strong>pressure</strong> increase the atherogenecity<br />
of cholesterol-rich lipoproteins ?<br />
Want <strong>to</strong> go beyond blood <strong>pressure</strong> in patients with hypertension?<br />
EBM.<br />
<strong>Is</strong> it just an antihypertensive treatment + statin?<br />
Who are those hypertensive patients at high CVD risk?<br />
Conclusion.
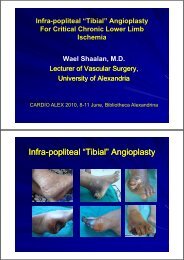
Treating a Single Risk Fac<strong>to</strong>r is Not Enough:<br />
Event (%)<br />
f Primary E<br />
Risk of<br />
100<br />
90<br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
Risk reduction (%) Events not avoided (%)<br />
CV Risk 64<br />
Remains Even After<br />
75<br />
72<br />
86<br />
Antihypertensive Therapy in<br />
Placebo-Controlled 36<br />
Studies<br />
SHEP (chlorthalidone<br />
+/- atenolol)<br />
25<br />
MRC-O (HCTZ +<br />
atenolol)<br />
14<br />
Syst-Eur (nitrendipine,<br />
enalapril, HCTZ)<br />
28<br />
PROGRESS<br />
(perindopril +/-<br />
diuretic)<br />
SHEP Cooperative Research Group. JAMA. 1991;265:3255-3264. MRC Working Party. BMJ. 1992;304:405-412.<br />
Staessen JA et al, for the Syst-Eur Trial Investiga<strong>to</strong>rs. Lancet. 1997;350<br />
350:757-764. PROGRESS Collaborative Group.<br />
Lancet. 2001;358:1033-1041.
Treating single risk fac<strong>to</strong>r is not <strong>enough</strong><br />
CV risk remains even after statin therapy<br />
CV Risk Remains Even After<br />
Antidyslipidemic Therapy in<br />
Placebo-Controlled Studies<br />
Adapted from reference 1<br />
Landmark studies in patients with varying degrees of<br />
CV risk show that statins reduce CV events by 9 -<br />
1. Kastelein 37% JJP. 1 Eur Heart J 2005; 7:F27-F33.<br />
Risk Fac<strong>to</strong>rs Are Part of the Same<br />
Atherosclerotic ti Disease Process<br />
CV Risk<br />
Atherosclerosis<br />
Dyslipidaemia<br />
Remodeling<br />
Hypertension<br />
Hypoxia/<br />
<strong>Is</strong>chemia<br />
Diabetes<br />
Smoking<br />
Obesity<br />
Promotion<br />
Inflammation<br />
Vasoconstriction<br />
Plaque<br />
Rupture<br />
CV Events<br />
Stroke<br />
MI<br />
Heart Failure<br />
Angina<br />
Thrombosis<br />
Adapted from Schiffrin EL et al. Am J Hypertens. 2002;15:115s-122s.
Current Guidelines Recognize the Relationship<br />
Among Risk Fac<strong>to</strong>rs<br />
All patients should be classified<br />
not only in relation <strong>to</strong> the grades<br />
of hypertension but also in<br />
terms of the <strong>to</strong>tal cardiovascular<br />
risk resulting from the<br />
coexistence of different risk<br />
fac<strong>to</strong>rs, organ damage and<br />
disease.<br />
Decisions on treatment<br />
strategies (initiation of drug<br />
treatment, BP threshold and<br />
target t for treatment, t t use of<br />
combination treatment, need of<br />
a statin and other nonantihypertensive<br />
drugs) all<br />
importantly depend on the initial<br />
level of risk.<br />
ABCs of multiple risk fac<strong>to</strong>r management<br />
A<br />
treatment.<br />
<strong>Blood</strong><br />
BC Cholesterol<br />
D<br />
Diabetes<br />
is<br />
E Eye<br />
F<br />
Feet<br />
G<br />
‘‘Guardian’’<br />
Advice—Education, self<br />
management, concordance with<br />
t t t Special focus on smoking<br />
cessation, diet, physical activity, and<br />
weight reduction<br />
<strong>Blood</strong> <strong>pressure</strong> targets — <strong>Blood</strong><br />
<strong>pressure</strong> , 130/80 mm Hg, which may<br />
require combinations of a diuretic,<br />
ACE inhibi<strong>to</strong>r/ARB, and a CCB<br />
and LDL cholesterol<br />
targets<br />
control —A normal HbA1c%<br />
ideal but the practical target is<br />
6.5%.<br />
care<br />
care<br />
Hypertension<br />
Dyslipidemia<br />
Hyperglycemia/<br />
Insulin resistance<br />
Platelet activation<br />
and aggregation<br />
Adapted from JBS 2: Joint British Societies’ guidelines on prevention<br />
drugs for cardiovascular<br />
of cardiovascular disease in clinical practice Heart 2005;91;1-52<br />
prevention—Aspirin75 mg daily
<strong>Is</strong> <strong>treating</strong> <strong>Blood</strong> <strong>pressure</strong> <strong>alone</strong> <strong>enough</strong> <strong>to</strong> <strong>protect</strong> <strong>your</strong><br />
hypertensive patient?<br />
Does the elevation of blood <strong>pressure</strong> increase the atherogenecity<br />
of cholesterol-rich lipoproteins ?<br />
Want <strong>to</strong> go beyond blood <strong>pressure</strong> in patients with hypertension?<br />
EBM.<br />
<strong>Is</strong> it just an antihypertensive treatment + statin?<br />
Who are those hypertensive patients at high CVD risk?<br />
Conclusion.<br />
Hypertension and Dyslipidemia<br />
• Mechanism:<br />
1. Increase Shear force on Endothelium.<br />
2. Decreased NO Availability<br />
3. Increased Oxidized LDL-Cholesterol
Circulating oxidized LDL and<br />
Hypertension<br />
80<br />
70 Hypertensive<br />
60<br />
men had 62%<br />
50<br />
higher mean<br />
40<br />
Ox LDL levels<br />
30<br />
compared with<br />
20 normotensive<br />
controls<br />
10<br />
0<br />
Normotensive<br />
Subjects<br />
Borderline Hypertensive<br />
Subjects<br />
Toikka JO. Hypertension 2000; 36: 929-33<br />
<strong>Is</strong> <strong>treating</strong> <strong>Blood</strong> <strong>pressure</strong> <strong>alone</strong> <strong>enough</strong> <strong>to</strong> <strong>protect</strong> <strong>your</strong><br />
hypertensive patient?<br />
Does the elevation of blood <strong>pressure</strong> increase the atherogenecity<br />
of cholesterol-rich lipoproteins ?<br />
Want <strong>to</strong> go beyond blood <strong>pressure</strong> in patients with hypertension?<br />
EBM.<br />
<strong>Is</strong> it just an antihypertensive treatment + statin?<br />
Who are those hypertensive patients at high CVD risk?<br />
Conclusion.
Treatment of Associated Risk Fac<strong>to</strong>rs<br />
• Statins: small doses of statins e.g. a<strong>to</strong>rvastatin 10<br />
mg are added <strong>to</strong> antihypertensive therapy in<br />
patients with borderline elevation of LDL-C (> 130<br />
mg/dl) and multiple RFs.<br />
M h M Ib hi t l E ti G id li P ti f<br />
Mohsen. M.Ibrahim et al. Egyptian Guidelines: Prevention of<br />
Atherosclerotic CV Disease (Executive Summary):2006; 1-34
Treatment of Associated Risk Fac<strong>to</strong>rs<br />
Journal of Hypertension 2007, Vol 25 No 6
Cardiovascular risk fac<strong>to</strong>rs for consideration of statin<br />
therapy in non-dyslipidemic id i patients t with<br />
hypertension*<br />
• Male sex<br />
• Smoking<br />
• Left ventricular hypertrophy<br />
• Total cholesterol <strong>to</strong> HDL ratio > 6<br />
Risk Fac<strong>to</strong>rs<br />
• Age 55 years or older<br />
• Family his<strong>to</strong>ry of premature CVD<br />
• Other ECG abnormalities<br />
• Microalbuminuria or proteinuria<br />
If hypertensive patients have 3 or more of these RFs,<br />
statins should be considered.<br />
In addition, patients should be treated according <strong>to</strong><br />
the most recent Canadian Lipid Recommendations<br />
2008 Canadian Hypertension Education Program Recommendations<br />
Heart 2005;91(Suppl V):v1–v52. doi: 10.1136/hrt.2005.079988
Want <strong>to</strong> go beyond blood <strong>pressure</strong> in<br />
patients with hypertension?<br />
•Add a Statin !<br />
–Further reduction in CHD by >30%<br />
–Further reduction in stroke by 25%<br />
Irrespective of Baseline Cholesterol Values<br />
<strong>Is</strong> <strong>treating</strong> <strong>Blood</strong> <strong>pressure</strong> <strong>alone</strong> <strong>enough</strong> <strong>to</strong> <strong>protect</strong> <strong>your</strong><br />
hypertensive patient?<br />
Does the elevation of blood <strong>pressure</strong> increase the atherogenecity<br />
of cholesterol-rich lipoproteins ?<br />
Want <strong>to</strong> go beyond blood <strong>pressure</strong> in patients with hypertension?<br />
EBM.<br />
<strong>Is</strong> it just an antihypertensive treatment + statin?<br />
Who are those hypertensive patients at high CVD risk?<br />
Conclusion.
ASCOT: Integration of antihypertensive regimens with<br />
statin ( CADUET)<br />
Primary endpoint: Nonfatal MI and fatal CHD<br />
P=0.001<br />
Significant effects<br />
evident within the<br />
first 3 months of<br />
treatment (p=0.02)<br />
A previously<br />
unseen 53%<br />
reduction<br />
in CV events in just<br />
3.3 years<br />
Courtesy of Appel G, 2006.<br />
Adapted from Dahlöf B et al. www.ascotstudy.org.<br />
The Collaborative A<strong>to</strong>rvastatin Diabetes<br />
Study y( (CARDS) 1 :<br />
Can a<strong>to</strong>rvastatin <strong>protect</strong> patients at increased CV risk?<br />
Cumulative hazard of primary endpoint 1<br />
CARDS: Multicentre, randomised study in<br />
Type II diabetes patients without<br />
dyslipidaemia or documented his<strong>to</strong>ry of<br />
CVD, given a<strong>to</strong>rvastatin 10mg/day<br />
(n=1428) or placebo (n=1,410). Primary<br />
endpoint was time <strong>to</strong> first occurrence of<br />
acute CHD events, coronary<br />
revascularisation or stroke. The trial was<br />
s<strong>to</strong>pped 2 years earlier than planned<br />
because the pre-specified early s<strong>to</strong>pping<br />
rule for efficacy had been met. Median<br />
duration of follow-up: 3.9 years.<br />
84% of patients in both groups were hypertensive<br />
1.Colhoun HM et al. on behalf of the CARDS investiga<strong>to</strong>rs. Lancet<br />
2004; 364: 685-696.
CADUET.. The Dual Efficacy in a Single Pill<br />
Gemini data show that Caduet reduces components of CV risk across a<br />
broad range of patients you see every day<br />
n=1220<br />
14 week<br />
These results demonstrate that treatment with Caduet either <strong>alone</strong>, or in<br />
addition <strong>to</strong> existing antihypertensive agents, is an effective and safe<br />
treatment <strong>to</strong> reduce <strong>to</strong>tal CHD risk.<br />
Physicians were able <strong>to</strong> titrate from 5 mg/10 mg <strong>to</strong> 10 mg/80 mg.<br />
Erdine S, et al. Single-pill amlodipine / a<strong>to</strong>rvastatin helps patients of diverse ethnicity attain recommended goals for blood <strong>pressure</strong> and lipids (the Gemini-AALA<br />
,1-15.2008study). Journal of Human Hypertension.<br />
CADUET.. The Dual Efficacy in a Single Pill<br />
Caduet - significantly reduced blood <strong>pressure</strong> and LDL-C<br />
JEWEL l Study - 1138 patients with hypertension and dyslipidaemia<br />
16 week<br />
Caduet effectively reduced sys<strong>to</strong>lic BP (SBP) and low-density lipoprotein cholesterol<br />
(LDL-C) levels, and enabled more patients <strong>to</strong> achieve BP and LDL-C goals.<br />
Physicians were able <strong>to</strong> titrate from 5 mg/10 mg <strong>to</strong> 10 mg/80 mg.<br />
Curran MP. Amlodipine/A<strong>to</strong>rvastatin A Review of its Use in the Treatment of Hypertension and Dyslipidaemia and the Prevention of Cardiovascular Disease. Drugs<br />
2010; 70 (2): 191-213
CADUET.. The Dual Efficacy in a Single Pill<br />
AVALON trial, 847 patient with hypertension and dyslipidemia at the end of<br />
week 8. mean dose was 7.6/ 28.4 mg<br />
Mean LDL-C ** reduction<br />
Mean reduction in SBP(mmHg)<br />
Mean reduction in DBP(mmHg)<br />
-12.5<br />
-8.2<br />
-37.2%<br />
- Messerli FH, BaKris GL, et al. Efficacy and Safety of Coadministered Amlodipine and A<strong>to</strong>rvastatin in Patients With Hypertension and Dyslipidemia<br />
Results of the AVALON Trial. Clin Hypertens. 2006;8:571–581<br />
<strong>Is</strong> <strong>treating</strong> <strong>Blood</strong> <strong>pressure</strong> <strong>alone</strong> <strong>enough</strong> <strong>to</strong> <strong>protect</strong> <strong>your</strong><br />
hypertensive patient?<br />
Does the elevation of blood <strong>pressure</strong> increase the atherogenecity<br />
of cholesterol-rich lipoproteins ?<br />
Want <strong>to</strong> go beyond blood <strong>pressure</strong> in patients with hypertension?<br />
EBM.<br />
<strong>Is</strong> it just an antihypertensive treatment + statin?<br />
Who are those hypertensive patients at high CVD risk?<br />
Conclusion.
<strong>Is</strong> it just an antihypertensive<br />
t i<br />
treatment + statin?<br />
Or<br />
Should we select molecules with<br />
synergistic benefits?<br />
Synergistic effect of CADUET on nitric oxide release<br />
from human endothelial cells<br />
Adapted from Mason RP. Cerebrovasc Dis. 2003;16(suppl 3):11-17.
Caduet … Early Improvements in Arterial Wall<br />
Compliance<br />
AVALON-AWC AWC * study strongly<br />
suggests that a greater early<br />
vascular benefit can be<br />
obtained from simultaneous<br />
treatment with amlodipine and<br />
a<strong>to</strong>rvastatin, vs. either agent<br />
<strong>alone</strong>, in patients with<br />
hypertension and<br />
dyslipidemia.<br />
11.70%<br />
19.30%<br />
1.30%<br />
3.10%<br />
Placebo A<strong>to</strong>rvastatin Amlodipine Caduet 5/10<br />
Effect of treatment on small artery compliance (c2) At week 8,<br />
1- Cohn JN. AVALON-AWC: Arterial Wall Compliance in the A<strong>to</strong>rvastatin and Amlodipine in Patients With Elevated Lipids and Hypertension Trial. Am J<br />
Hypertens 2009; 22:137-44.<br />
Caduet … Reversal of LDL-induced Endothelial Dysfunction<br />
Endothelial dysfunction contributes <strong>to</strong> mechanisms of atherogenesis and its<br />
clinical manifestations, including coronary artery disease. 1<br />
Effect of Caduet ®1<br />
100%<br />
90%<br />
80%<br />
60%<br />
40%<br />
20%<br />
0%<br />
‐20%<br />
‐40%<br />
‐60%<br />
% increase in NO ¤<br />
% d ti i i ONOO º<br />
‐50%<br />
Caduet partially res<strong>to</strong>red the NO level of LDL*-induced dysfunctional<br />
endothelium. 1<br />
Effect of Caduet may be enhanced by antioxidant properties related <strong>to</strong> their<br />
intermolecular actions in the cell membrane and an increase in the<br />
expression and coupling of endothelial nitric oxide synthase. 1<br />
¤ NO: Nitric Oxide,<br />
º ONOO-: Cy<strong>to</strong><strong>to</strong>xic Peroxynitrite<br />
*LDL: Low-density Lipoprotein<br />
1- Mason RP. A rationale for combination therapy in risk fac<strong>to</strong>r management: a mechanistic perspective. The American Journal of<br />
Medicine. 2005; 118(12A): 54S-61S.
ASCOT: Integration of antihypertensive regimens with<br />
statin<br />
Primary endpoint: Nonfatal MI and fatal CHD<br />
Courtesy of Appel G, 2006.<br />
Adapted from Dahlöf B et al. www.ascotstudy.org.<br />
.Baghdasarian SB, Thompson PD, Shi H, et al. effect of amlodipine and enalapril on cardiovascular events in normotensive<br />
coronary artery disease patients with concomitant statin use in the CAMELOT Trial(abstr) J AM Coll Cardiol 2006;47(Suppl 1):310A.
A single, once-daily tablet for improved<br />
adherence and compliance<br />
CARPE study: Caduet 2-Pill Combination<br />
Therapies on Adherence 1<br />
1. Nichol MB et al. J Clin Hypertens 8; 4: S6 Abstract P-526A.<br />
<strong>Is</strong> <strong>treating</strong> <strong>Blood</strong> <strong>pressure</strong> <strong>alone</strong> <strong>enough</strong> <strong>to</strong> <strong>protect</strong> <strong>your</strong><br />
hypertensive patient?<br />
Does the elevation of blood <strong>pressure</strong> increase the atherogenecity<br />
of cholesterol-rich lipoproteins ?<br />
Want <strong>to</strong> go beyond blood <strong>pressure</strong> in patients with hypertension?<br />
EBM.<br />
<strong>Is</strong> it just an antihypertensive treatment + statin?<br />
Who are those hypertensive patients at high CVD risk?<br />
Conclusion.
Case Study<br />
– Female<br />
– 45 years old<br />
– Non smoker<br />
– BP : 145/95 mm Hg<br />
– FBS : 97 mg/dl (on treatment)<br />
– TC : 195 mg/dL<br />
– LDL : 118 mg/dL<br />
– HDL : 35 mg/dL<br />
– TG : 185 mg/dL<br />
– Diabetic Neuropathy<br />
Current Treatment:<br />
– Diet and<br />
exercise<br />
– ACE<br />
45 yr old Female<br />
Non-smoker<br />
Diabetes<br />
No LVH<br />
BP: 145/95<br />
mm Hg<br />
LDL cholesterol: (118mg/dL)<br />
HDL cholesterol: (35mg/dL)<br />
Diabetic<br />
10 year CHD risk: 20%
ADA 2009 Guidelines<br />
DIABETES CARE, VOLUME 32, SUPPLEMENT 1, JANUARY 2009<br />
Framingham: 10-Year Risk of CHD<br />
Age (years)<br />
Points<br />
30-3434 -9<br />
35-3939 -4<br />
40-44<br />
44 0<br />
45-4949 3<br />
50-5454 6<br />
55-5959 7<br />
60-6464 8<br />
65-6969 8<br />
70-7474 8 Smoking<br />
LDL-C<br />
mg/dL Could You Be at Risk mmol/L for a Cardiovascular Points<br />
Event?<br />
A Scorecard for Men<br />
3<br />
0<br />
5<br />
2<br />
4<br />
0<br />
14<br />
Framingham: 10-Year Risk of CHD after adding<br />
CCB ,Diuretic , or BB<br />
Age (years)<br />
Points<br />
30-34<br />
34 -9<br />
35-3939 -4<br />
40-4444 0<br />
45-49<br />
49 3<br />
50-5454 6<br />
55-5959 7<br />
60-6464 8<br />
65-6969 8<br />
70-7474 8<br />
LDL-C<br />
mg/dL Could You Be at Risk mmol/L for a Cardiovascular Points<br />
Event?<br />
A Scorecard for Men<br />
3<br />
0<br />
5<br />
0<br />
4<br />
0<br />
12<br />
Framingham: 10-Year Risk of CHD after adding<br />
Caduet 5/10<br />
Age (years)<br />
Points<br />
30-34<br />
34 -9<br />
35-3939 -4<br />
40-4444 0<br />
45-49<br />
49 3<br />
50-5454 6<br />
55-5959 7<br />
60-6464 8<br />
65-6969 8<br />
70-7474 8<br />
LDL-C<br />
mg/dL Could You Be at Risk mmol/L for a Cardiovascular Points<br />
Event?<br />
A Scorecard for Men<br />
3<br />
-3<br />
5<br />
0<br />
4<br />
0<br />
9<br />
ASCOT: Integration of antihypertensive regimens with<br />
statin ( CADUET)<br />
Primary endpoint: Nonfatal MI and fatal CHD<br />
P=0.001<br />
Significant effects<br />
evident within the<br />
first 3 months of<br />
treatment (p=0.02)<br />
A previously<br />
unseen 53%<br />
reduction<br />
in CV events in just<br />
3.3 years<br />
Courtesy of Appel G, 2006.<br />
Adapted from Dahlöf B et al. www.ascotstudy.org.
<strong>Is</strong> <strong>treating</strong> <strong>Blood</strong> <strong>pressure</strong> <strong>alone</strong> <strong>enough</strong> <strong>to</strong> <strong>protect</strong> <strong>your</strong><br />
hypertensive patient?<br />
Does the elevation of blood <strong>pressure</strong> increase the atherogenecity<br />
of cholesterol-rich lipoproteins ?<br />
Want <strong>to</strong> go beyond blood <strong>pressure</strong> in patients with hypertension?<br />
Evidence Based Medicine.<br />
<strong>Is</strong> it just an antihypertensive treatment + statin?<br />
Who are those hypertensive patients at high CVD risk?<br />
Conclusion.<br />
Conclusion<br />
AA Statin Should Be Given To All High Risk<br />
Hypertensive Patients<br />
Caduet (Amlodipine+A<strong>to</strong>rvastatin 10 mg) Reduced<br />
Fatal CHD and Non Fatal MI By 53% Within the First 3<br />
Months in Hypertensive Patient at High Risk<br />
Caduet Improves Endothelial Function which will<br />
help in Retarding the Atherosclerotic Process in<br />
Hypertensive Patients at high Risk.