ENDO 3 Adrenal
ENDO 3 Adrenal
ENDO 3 Adrenal

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
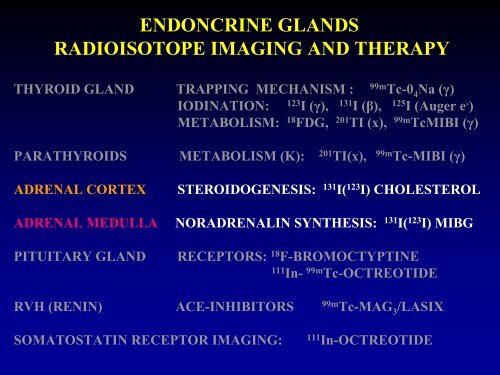
<strong>ENDO</strong>NCRINE GLANDS<br />
RADIOISOTOPE IMAGING AND THERAPY<br />
THYROID GLAND TRAPPING MECHANISM :<br />
99m<br />
Tc-0 4 Na (γ)<br />
IODINATION: 123 I (γ), 131 I (β), 125 I (Auger e - )<br />
METABOLISM: 18 FDG, 201 TI (x), 99m TcMIBI (γ)<br />
PARATHYROIDS METABOLISM (K): 201 TI(x),<br />
99m<br />
Tc-MIBI (γ)<br />
ADRENAL CORTEX<br />
ADRENAL MEDULLA<br />
STEROIDOGENESIS: 131 I( 123 I) CHOLESTEROL<br />
NORADRENALIN SYNTHESIS: 131 I( 123 I) MIBG<br />
PITUITARY GLAND RECEPTORS: 18 F-BROMOCTYPTINE<br />
111<br />
In- 99m Tc-OCTREOTIDE<br />
RVH (RENIN) ACE-INHIBITORS 99m Tc-MAG 3 /LASIX<br />
SOMATOSTATIN RECEPTOR IMAGING: 111 In-OCTREOTIDE
EMBRYOLOGY OF THE ADRENAL GLANDS
CORTEX:<br />
ADRENAL IMAGING<br />
131<br />
I( 123 I) CHOLESTEROL or NP-59<br />
(On/Off Dexamethasone Suppression)<br />
Carcinomas Do Not Visualize<br />
MEDULLA:<br />
131<br />
I ( 123 I) META-IODO-BENZYL-GUANIDINE or MIBG<br />
Carcinomas Visualize with MIBG<br />
MEDULLA also:<br />
111<br />
In-SOMATOSTATIN ANALOGUE<br />
or Octreotide
CORTEX:<br />
1) Hydrocortisone: (Cushing’s)<br />
ADRENAL GLANDS<br />
Normal<br />
glands<br />
lesion<br />
response<br />
to DXM<br />
suppression<br />
a) Hypertrophy (bilateral).….. hypertrophic + +<br />
b) Tumor (benign)…………… suppressed - +<br />
2) Aldosterone: Aldosteronoma (Cohn’s).. suppressed - +<br />
3) Androgens: ……....Congenital <strong>Adrenal</strong> Hypertrophy - +<br />
4) Carcinomas ………………………… NL - -<br />
NP-59<br />
imaging<br />
Octreo or<br />
MIBG<br />
MEDULLA:<br />
1) Norepinephrine: Pheochromocytoma….. NL -<br />
imaging<br />
+<br />
2) Carcinomas (Neuroblastoma)…………… NL - +
ADRENAL CORTEX
HYPOTHALAMIC PITUITARY ADRENAL AXIS
ADRENOCORTICAL SCINTIGRAPHY PROTOCOL<br />
PATIENT PREPARATION<br />
DEXAMETHASONE 8 mg/day from day -5 to day +3<br />
LUGOL’S SOLUTION 5 drops/day from day -2 to day + 8<br />
INJECTION<br />
Day 1: 0.5-1.0 mCi 131 I( 123 I) CHOLESTEROL (NP-59)<br />
IMAGING<br />
Days +2 (+3) : Scan on dexamethasone suppression<br />
Days +5 (+7) : Scan off dexamethasone suppression<br />
FOR BETTER LOCALIZATION<br />
a) MAG 3 Renal Scan<br />
b) SPECT/CT
CORTICAL SCINTIGRAPHY NP-59<br />
24 hours<br />
48 hours<br />
On Dexamethasone<br />
Normal <strong>Adrenal</strong>s
CORTICAL SCINTIGRAPHY NP-59<br />
Off Dexamethasone<br />
Normal <strong>Adrenal</strong>s
ADRENOCORTICAL IMAGING<br />
USE OF RENAL SCAN TO LOCALISE LESIONS<br />
MAG3 RENAL SCAN<br />
Appropriate localization<br />
Normal <strong>Adrenal</strong>s
ADRENOCORTICAL ADENOMA NP59<br />
FUSION<br />
+ =<br />
+<br />
<strong>Adrenal</strong> Scan Renal Scan<br />
=<br />
Fusion Image
Children with virulism<br />
131<br />
I-NP59 studies
CONGENITAL ADRENAL HYPERTROPHY<br />
NP-59 scans from 3 children with Congenital <strong>Adrenal</strong> Hypertrophy
ECTOPIC ADRENAL TISSUE<br />
IN TESTES OR OVARIES<br />
NP-59 scans from 3 children with suspected Ectopic <strong>Adrenal</strong> tissue in the testes
Patient hypertensive<br />
r/o aldosterone producing tumor (s)<br />
131<br />
I-NP59 study
RADIO-CHOLESTEROL 131 I-NP59 SCANS<br />
liver<br />
bowel<br />
Tumor left adrenal gland<br />
Aldosteronoma<br />
of the left adrenal gland(Cohn’s)
A patient with Cushing’s Syndrome<br />
131<br />
I-NP59 study
CUSHING’S ADENOMA LEFT ADRENAL<br />
SUPPRESSION OF THE RIGHT ADRENAL<br />
liver<br />
bowel<br />
bowel<br />
liver<br />
Left adrenal cortical tumor. What about the right adrenal<br />
The right adrenal is suppressed
A patient with Cushing’s Syndrome<br />
131<br />
I-NP59 study
ADRENOCORTICAL HYPERPLASIA<br />
liver<br />
Both adrenal glands large/prominent off Dexamethasone
Patient hypertensive<br />
r/o aldosterone producing tumor (s)<br />
131<br />
I-NP59 study
R/O ALDOSTERONOMA:<br />
Bilateral <strong>Adrenal</strong> Hyperplasia<br />
Tc-99m-MAG3 I-131-NP59
RADIO-CHOLESTEROL 131 I-NP59 SCANS<br />
INTERPRETATION DEPENDS ON PATIENT PREPARATION<br />
IF NO DEXAMETHASONE WAS GIVEN = THE STUDY IS NORMAL<br />
ON LOW DOSE DEXAMETHASONE = BILAT. ADRENAL HYPERPLASIA<br />
ON HIGH DOSE DEXAMETHASONE = BILATERAL ADENOMAS<br />
Tc-99m-MAG3 I-131-NP59
A patient with Cushing’s Syndrome<br />
131<br />
I-NP59 study
ADRENOCORTICAL ADENOMA NP59<br />
liver<br />
bowel<br />
Left adrenal gland large/prominent<br />
Right adrenal suppressed
ADRENAL MEDULLA
EMBRYOLOGY OF THE ADRENAL MEDULLA
IMAGING ADRENAL MEDULARY LESIONS<br />
131/123<br />
I meta-iodo-benzyl guanidine (MIBG)<br />
It is associated with the neurosecretory granules of the<br />
cytoplasmic portion of the adrenal medulla<br />
INDICATIONS<br />
• Pheochromocytomas: sensitivity 85%, specificity > 99%<br />
• Neuroblastomas: Sensitivity is greater than 90%<br />
for soft tissue, bone, or bone marrow involvement<br />
METHOD<br />
Patient preparation: Stop medications with sympathetic action<br />
Inject 500µCi (5-10mCi) 131 I ( 123 I)-MIBG and scan at 48hr (+72hr)<br />
MAG 3 Renal Scan or SPECT/CT<br />
LESION LOCALIZATION
A patient with hypertension is studied to exclude<br />
Pheochromocytoma
MIBG NORMAL STUDIES<br />
Total body studies<br />
because<br />
pheochromocytomas<br />
may involve<br />
the adrenal glands,<br />
sympathetic ganglia,<br />
or other sites<br />
Normal <strong>Adrenal</strong><br />
visualization
MIBG NORMAL STUDY<br />
PHYSIOLOGIC ADRENAL VISUALIZATION<br />
24Hr (low count image) 48Hr<br />
48Hr Repeat Study
PHEOCHROMOCYTOMA
SENSITIVITY OF MIBG FOR PHEOCHROMOCYTOMA<br />
15yo boy with Pheo (k=autotransplanted kidney) 75yo man with recurrent<br />
malignant metast Pheo<br />
Cancer 1984; 34(2):86
A patient with clinical and laboratory findings<br />
suggesting Pheo<br />
and a CT showing lesion in the left adrenal
PHEOCHROMOCYTOMA<br />
MIBG study<br />
Anterior<br />
Posterior
PHEOCHROMOCYTOMA<br />
MIBG study<br />
48hr post 0.750mCi 131 I-MIBG
ADRENAL MEDULLARY PHEOCHROMOCYTOMA
PHEOCHROMOCYTOMA<br />
“Ectopic”<br />
Renal Scan<br />
MIBG study
57yo man s/p L adrenalectomy for Pheochromocytoma
MALIGNANT METASTATIC<br />
PHEOCHROMOCYTOMA<br />
MIBG study<br />
Ant<br />
Post<br />
Post<br />
Ant<br />
Ant<br />
Ant
MALIGNANT PHEOCHROMOCYTOMA<br />
METASTATIC TO LUNGS<br />
45yo woman s/p resection of pheochromocytoma
123<br />
I-MIBG SPECT/CT for PHEOCHROMOCYTOMA<br />
10yo boy with laboratory presentation raising the<br />
question of Pheochromocytoma.<br />
MRI is negative. Patient allergic to iodine.
123<br />
I-MIBG SPECT/CT<br />
Pheochromocytoma<br />
10 yo child with hypertension + lab work suggesting Pheochromocytoma
123<br />
I-MIBG SPECT/CT for PHEOCHROMOCYTOMA
MULTI-<strong>ENDO</strong>CRINE NEOPLASIA
MULTIPLE <strong>ENDO</strong>CRINE ADENOMATOSIS (MEA)<br />
Familial Syndromes<br />
Common: Neuroectodermal origin of glands involved<br />
(informational coding)<br />
1 Multiple Endocrine Neoplasia type I (MEN-I)<br />
Parathyroid Adenoma<br />
Pancreatic Islets (Zollinger-Ellison Syndrome)<br />
Pituitary (Hypo or Hyper Function)<br />
2 Multiple Endocrine Neoplasia type II (MEN-II)<br />
Parathyroid Adenoma<br />
Pheochromocytoma<br />
Medullary Thyroid Carcinoma
A Child with a history of resected Medullary thyroid carcinoma
BILATERAL PHEOCHROMOCYTOMAS<br />
MEN-II<br />
MIBG study<br />
24hr 48hr<br />
96hr
A Child with a history of resected Medullary thyroid<br />
carcinoma and Pheochromocytoma
RECURRENT PHEOCHROMOCYTOMA<br />
MEN-II<br />
MIBG study<br />
7/14 while taking Labetalol<br />
11/17 off medication
27yo man s/p thyroidectomy at age 15y for Medullary carcinoma<br />
and bilateral adrenalectomy at age 20y for pheochromocytomas
RECURRENT PHEOCHROMOCYTOMA<br />
MEN-IIb<br />
MIBG study
NEUROBLASTOMA
NM studies in NEUROBLASTOMA<br />
Bone Scan/(Liver-Renal scans)<br />
MIBG Total Body Imaging/Therapy<br />
Antibody Imaging/Therapy<br />
Somatostatin-analogue (Octreotide)
NEUROBLASTOMA<br />
Primary Tumor calcified
A 10 mo old child with proptosis
NEUROBLASTOMA PRIMARY TUMOR<br />
AND METASTASIS TO BONES<br />
Tc-99m MDP Bone scan
JNM 25(7): 773
A child with Neuroblastoma. Evaluate for metastases
131<br />
I-MIBG<br />
NEUROBLASTOMA Primary<br />
VISCERAL METASTASIS<br />
Anterior Posterior
NEUROBLASTOMA<br />
WITH VISCERAL METASTASIS<br />
131<br />
I-MIBG STUDY<br />
AND TcSC, TcDTPA<br />
SC+DTPA
A child with Neuroblastoma<br />
and positive bone marrow biopsy
NEUROBLASTOMA<br />
WITH BONE MARROW METASTASIS<br />
131<br />
I-MIBG<br />
Posterior total body images to better show the bone marrow
111<br />
In-OCTREOTIDE SCINTIGRAPHY<br />
Somatostatin(14AA)<br />
Octreotide=Oligopeptide analogue(8AA)<br />
Tumors with membrane somatostatin receptors<br />
Carcinoid Non-Small Cell Lung cancer<br />
Gastrinoma Meningiomas<br />
Insulinoma Pheochromocytoma<br />
Glucagonoma Apudomas non specified<br />
Paraganglioma Medullary thyroid carcinoma<br />
Granulomatous<br />
Autoimmune<br />
Sarcoidosis<br />
Wegener’s<br />
Tuberculosis<br />
Graves’ Thyroid<br />
Exophthalmos
111<br />
In-OCTREOTIDE SCINTIGRAPHY
A child with Neuroblastoma
111<br />
In-OCTREOTIDE SCINTIGRAPHY<br />
NEUROBLASTOMA<br />
Bone metastases of neuroblastoma
FDG-PET IN<br />
NEUROBLASTOMA
FDG-PET IN NEUROBLASTOMA<br />
FDG accumulates within most neuroblastomas<br />
It also accumulates within neuroblastomas<br />
which are MIBG negative
A child with Neuroblastoma
MIBG and FDG-PET<br />
in NEUROBLASTOMA<br />
tumor<br />
tumor<br />
tumor<br />
tumor<br />
Primary Tumor<br />
Skull metastasis
Recurrent Neuroblastoma in a 6 month old boy
FDG-PET IN<br />
NEUROBLASTOMA<br />
Recurrent Tumor
Neuroblastoma at diagnosis and 6mos after chemotherapy
FDG-PET IN NEUROBLASTOMA<br />
EFFECT OF THERAPY<br />
FDG-PET CT-Scan MIBG<br />
Baseline<br />
After Chemotherapy
A 17 year old girl with right shoulder pain
FDG-PET IN<br />
HEPATOBLASTOMA<br />
CT Scan FDG - PET<br />
necrotic<br />
tumor<br />
necrotic<br />
tumor<br />
Active viable tumor
PITUITARY GLAND TUMORS<br />
PET: 11 C-BROMOCRYPTINE<br />
SPECT: SOMATOSTATIN analogue<br />
( 111 I-OCTREOTIDE)