Guide to PKU - Mead Johnson Nutrition
Guide to PKU - Mead Johnson Nutrition
Guide to PKU - Mead Johnson Nutrition

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Mead</strong> <strong>Johnson</strong> MetabolicsParents’ <strong>Guide</strong> <strong>to</strong> <strong>PKU</strong>An Informational <strong>Guide</strong> <strong>to</strong> DietaryManagement of Individuals with <strong>PKU</strong>This booklet is intended by <strong>Mead</strong> <strong>Johnson</strong> <strong>to</strong> be provided <strong>to</strong> you by your healthcareprofessional as part of his or her care plan in the dietary management of <strong>PKU</strong>. Your healthcareprofessional is your primary source of information and advice. Always discuss with yourhealthcare professional any information you receive and any changes you wish <strong>to</strong> make.
Preface<strong>PKU</strong> is an abbreviation for phenylke<strong>to</strong>nuria, a metabolicdisorder which affects about 1 in 10,000 children. It is an inheriteddisorder which can be treated very successfully. We at <strong>Mead</strong> <strong>Johnson</strong>hope this booklet will help you learn more about <strong>PKU</strong>.We put Parents’ <strong>Guide</strong> <strong>to</strong> <strong>PKU</strong> <strong>to</strong>gether because we know how“lost” you may be feeling right now. What is <strong>PKU</strong>? How did our babyget it? Will our child grow and develop normally? How will we dealwith this disorder? You are probably looking for answers <strong>to</strong> these andother questions. We hope that some of your questions about the recentdiagnosis of your child will be answered here.In Parents’ <strong>Guide</strong> <strong>to</strong> <strong>PKU</strong>, we have drawn on our experienceproviding metabolic formulas for children with <strong>PKU</strong>. Your experiencesand your child will not be exactly like other families, but we hope thatyou and your family can benefit from what we have learned. We havealso included the words of some parents who are truly living with <strong>PKU</strong>so that you might hear their experiences for yourself.For simplicity, we have alternated “he” and “she” when referring <strong>to</strong>your child since both boys and girls will benefit from this information.<strong>Mead</strong> <strong>Johnson</strong> <strong>Nutrition</strong>als gives special thanks <strong>to</strong> The Children’s Hospital InheritedMetabolic Diseases Clinic (affiliated with University of Colorado Health Sciences Center)for their help in providing information contained in this booklet.2
Table of ContentsIntroduction 4What Is <strong>PKU</strong>? 4Will Our Child Grow and Develop Normally? 4How Did Our Child Get <strong>PKU</strong>? 5How Do We Know Our Child Has <strong>PKU</strong>? 7How Will We Manage Our Child’s <strong>PKU</strong>? 8The <strong>PKU</strong> Diet 8Regular Clinic Visits 8First Steps In Treatment 9How Will This Affect Our Family? 10What Can We Expect As Our Child Grows? 11Infancy: Birth <strong>to</strong> 12 Months of Age 11Toddlers: Ages 1 <strong>to</strong> 3 Years 12Preschoolers: Ages 3 <strong>to</strong> 5 Years 13Grade School: Ages 6 <strong>to</strong> 12 Years 13Adolescents: Ages 12 <strong>to</strong> 18 Years 14Maternal <strong>PKU</strong>: When Your DaughterIs Ready To Have Children 15Questions Parents Often Ask 16Tips For Parents 19Hints While Traveling 19Helping Your School-AgedChild With The Diet 20Glossary Of Terms Associated With <strong>PKU</strong> 21Where To Go For More Information 223
IntroductionWhat is <strong>PKU</strong>?<strong>PKU</strong> is an abbreviation forphenylke<strong>to</strong>nuria, a metabolic disorderin which the affected personlacks an enzyme that breaks downa component of protein in foods.To understand <strong>PKU</strong>, we have<strong>to</strong> start with amino acids—thebuilding blocks of proteins. Someamino acids are essential, whichmeans the body cannot makethem and they must be suppliedby the diet. Phenylalanine is anessential amino acid which ispresent in most protein-containingfoods; it is also converted by thebody in<strong>to</strong> another amino acidcalled tyrosine. Phenylalanine isoften abbreviated <strong>to</strong> “Phe”(pronounced “Fee”). Bothphenylalanine and tyrosine areneeded for normal growth anddevelopment. The person with<strong>PKU</strong> doesn’t have the enzyme(phenylalanine hydroxylase) that thebody uses <strong>to</strong> make this conversionfrom phenylalanine <strong>to</strong> tyrosine.Because the body can’t get ridof the excess amounts of phenylalanine(Phe) in normal ways(ie, by converting it <strong>to</strong> tyrosine),phenylalanine builds up in theblood and other body tissues, andsome is converted <strong>to</strong> substancescalled phenylke<strong>to</strong>nes, which areexcreted in the urine. This processof the body trying <strong>to</strong> get rid ofexcess phenylalanine is where <strong>PKU</strong>gets its name: phenylke<strong>to</strong>nuria orphenylke<strong>to</strong>nes in the urine. Thehigh level of phenylalanine,phenylke<strong>to</strong>nes, and low tyrosinelevels result in poor growth andmental development.Will Our Child Growand Develop Normally?With proper dietary managementand early identification,your child can grow and developnormally. Your child is likely <strong>to</strong>develop at the same rate as otherchildren his age, <strong>to</strong> be equallyintelligent, and <strong>to</strong> do as wellin school.Without dietary treatment,your child could develop moreslowly and could become mentallyretarded. Many studies have showna relationship between the degreeof dietary control, blood Phelevels, and the child’s IQ, so itis very important <strong>to</strong> follow theinstructions you are givenconcerning your baby’s diet <strong>to</strong>maintain “safe” blood Phe levels.<strong>PKU</strong> is a chronic disorder,which means your child will need<strong>to</strong> follow a special diet for all ofchildhood and in<strong>to</strong> adulthood.The most healthy persons with<strong>PKU</strong> are those who control their4
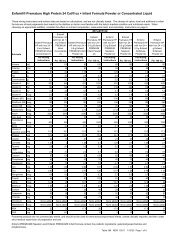
lood phenylalanine levels for life.It is especially important that girlscontrol their blood phenylalaninelevels because high levels of phenylalaninein a pregnant mother’sblood can cause serious problemsfor a developing fetus. Remainingon the diet for life is stronglyrecommended for all individualswith <strong>PKU</strong>.How Did OurChild Get <strong>PKU</strong>?You are probably wonderinghow your child got <strong>PKU</strong>. You mayhave other children who do nothave <strong>PKU</strong>, and it’s possible thatno one in your family has everhad <strong>PKU</strong> as far back as anyonecan remember.<strong>PKU</strong> is a genetic disorder,which means it is inherited fromthe parents. To understand howyour child “got” <strong>PKU</strong>, it’s helpful<strong>to</strong> know something about chromosomesand genes. Every cell inthe body contains 23 pairs ofchromosomes (a <strong>to</strong>tal of 46 individualchromosomes) which haveall the genetic information thebody needs. One chromosome ofevery pair is inherited from thefather, and one chromosome ofevery pair is inherited from themother. These chromosomes aremade up of genes which are linedup on the chromosomes like beadson a string. The genes are arrangedin pairs just like the chromosomesare. Genes work <strong>to</strong> determinephysical characteristics (such as eyecolor and hair color) and provide“instructions” for developing andmaintaining the body, such asmaking phenylalanine hydroxylase.In genetic terms, <strong>PKU</strong> is anau<strong>to</strong>somal recessive disorder.Au<strong>to</strong>somal means that it is notlocated on the “x” or “y” chromosomethat determines gender.Recessive means that both parentsmust contribute a non-workinggene for <strong>PKU</strong> in order for thechild <strong>to</strong> have <strong>PKU</strong>. If only oneparent passes on the gene for<strong>PKU</strong>, the child will not have anysymp<strong>to</strong>ms of <strong>PKU</strong>, but will be a“carrier” and still be able <strong>to</strong> passthat gene along <strong>to</strong> his or her children.Since the parents are usually“carriers” of the disorder, they willhave no symp<strong>to</strong>ms of <strong>PKU</strong> and maynot even know they are carriers.In fact, <strong>PKU</strong> may have beenpassed down silently through bothfamilies for many generations—that is, no one in either familymay have known they carry thegene. It’s only when two carriershave children <strong>to</strong>gether that inherita non-working copy of the genefrom both parents that the disorderis expressed with clinical symp<strong>to</strong>ms.Although untreated <strong>PKU</strong>can cause mental retardation, itdoes not indicate a family his<strong>to</strong>ryof mental retardation. <strong>PKU</strong> canbe very successfully treated, andchildren with <strong>PKU</strong> can grow anddevelop normally, both mentallyand physically.Figure 1 illustrates how <strong>PKU</strong>is inherited. For a child <strong>to</strong> have<strong>PKU</strong>, each parent must be a carrier5
of the disorder, which is shownas “Pp” in Figure 1. A carrier hasone working gene (P) for producingthe enzyme phenylalaninehydroxylase and one non-workinggene (p) which does not producethe enzyme, but no symp<strong>to</strong>msof <strong>PKU</strong>.In every pregnancy, the eggand the sperm combine <strong>to</strong> makea fetus. One of the mother’s genesfor a trait (P or p in this case) fromthe egg and one of the father’sgenes (P or p) from the sperm go<strong>to</strong> make the fetus. The inheritanceof genes is a completely randomprocess, and if the baby inheritstwo p genes, he will be born with<strong>PKU</strong>. This child (pp, in geneticterms) requires nutritional management<strong>to</strong> keep excess phenylalaninefrom being <strong>to</strong>xic <strong>to</strong> his body.As shown in Figure 1, whentwo carriers for the non-workinggene have children <strong>to</strong>gether, thereis a one in four chance (25%) thatthey will have a child with <strong>PKU</strong>.Likewise, there is a 75% chancethey will have a baby who doesnot have <strong>PKU</strong>; this child may bea carrier (Pp) like the parentsor may have two working (PP)genes. These odds don’t meanthat a family of four childrenwill have one child with <strong>PKU</strong>,because the chances are thesame with every pregnancy.PpNon-AffectedCarrierNon-AffectedCarrierWith every child, the odds in thisexample are one in four of having<strong>PKU</strong>.Because <strong>PKU</strong> is hereditary,everyone in the families of bothparents should know about thepresence of <strong>PKU</strong>. This will helpmake certain that all babies bornin<strong>to</strong> the family are screened for<strong>PKU</strong> at birth. Families should talkwith genetic counselors for themost up-<strong>to</strong>-date information onthe genetic aspects of <strong>PKU</strong>.How Recessive Inheritance WorksppAffectedChildPpP=Working Genep= <strong>PKU</strong> GenePpPpNon-AffectedCarrierNon-AffectedCarrierPPNon-AffectedFigure 1: Two <strong>PKU</strong> (pp) genes areneeded for a child <strong>to</strong> be affected.Each child has a 25% chance ofbeing affected. If one parent is affectedby <strong>PKU</strong>, then each child has a 50%chance of being affected.6
How Do We KnowOur Child Has <strong>PKU</strong>?Children with <strong>PKU</strong> are firstidentified from elevated bloodphenylalanine levels detected withnewborn screening tests. Thesetests are convenient, inexpensive,and allow early identification ofseveral genetic diseases. <strong>PKU</strong>screening is manda<strong>to</strong>ry for allnewborns in the United Statesand in many other countries. Byscreening in the first days of life,infants with <strong>PKU</strong> can receivetreatment immediately. Promptdetection and treatment areextremely important becausemost problems associated withuntreated <strong>PKU</strong> can be preventedif treatment is started early.To perform the tests, a fewdrops of blood are taken from thebaby’s heel and absorbed on<strong>to</strong> apiece of special blotter paper.The blood is usually taken inthe newborn nursery.Several labora<strong>to</strong>ry tests are used<strong>to</strong> screen for <strong>PKU</strong>, the most commonof which is called the Guthrietest. This test uses a certain strainof bacteria which needs phenylalanine<strong>to</strong> live. If there is excessphenylalanine in the baby’s blood,as in a baby with <strong>PKU</strong>, the bacteriawill grow. The more phenylalaninethere is in the blood, themore the bacteria will grow aroundthe blotter paper. The amount ofbacteria can then be compared <strong>to</strong>established standards <strong>to</strong> determinethe phenylalanine level in the baby’sblood. Tandem mass spectrometryis also used in some states <strong>to</strong>screen for <strong>PKU</strong>.If results of screening tests showelevated phenylalanine levels(positive), another blood sample iscollected and a repeat test is run <strong>to</strong>confirm the results. Positiveresults on the screening testdon’t diagnose the child with<strong>PKU</strong>, but they do indicate a needfor further tests. More completeconfirma<strong>to</strong>ry tests are done byyour baby’s doc<strong>to</strong>r or a clinic thatspecializes in treating <strong>PKU</strong>.High levels of phenylalanine inthe blood can indicate yet anothertype of genetic disorder which issimilar <strong>to</strong> <strong>PKU</strong>, but extremely rare.It is important <strong>to</strong> distinguish thisgroup of patients from childrenwith <strong>PKU</strong> because they must betreated with certain medicationsin addition <strong>to</strong> a special diet. Theclinic doc<strong>to</strong>rs will perform severaltests on your baby <strong>to</strong> be sure thediagnosis of <strong>PKU</strong> was correct.In the 1930s, Fölling and othersidentified in severely mentallyretarded patients a condition ofhigh phenylpyruvic acid in theirurines. This was later shown <strong>to</strong> bedue <strong>to</strong> the patient’s inability <strong>to</strong>utilize phenylalanine. However, itwas not until the 1950s that dietscould be developed <strong>to</strong> treat the highlevels of phenylalanine in infants.Before simplified screening for<strong>PKU</strong> became available early in the1960s, infants with <strong>PKU</strong> oftenwere not treated with special dietsuntil their parents noticed the babywas not developing normally. Bythat time, brain damage hadalready occurred.The development of a simplesensitive test <strong>to</strong> pick up phenylalaninein the blood and an effectivediet resulted in the state-mandatedscreening program that picked upyour baby’s elevated phenylalaninelevels. Studies were carried out <strong>to</strong>determine if and when the specialdiet could be discontinued. Theresearch showed that diet wasneeded for life <strong>to</strong> assure the infantreaches his or her maximummental abilities. Today, babies with<strong>PKU</strong> can develop as normally astheir unaffected siblings and go on<strong>to</strong> lead normal successful lives, aslong as the special diet prescribedis followed. Research continues <strong>to</strong>be carried out looking for alternatives<strong>to</strong> diet. Until that goal isreached, special diets will be theonly solution <strong>to</strong> help preventmental retardation.7
How Will We Manage <strong>PKU</strong>?The <strong>PKU</strong> DietYour child’s special <strong>PKU</strong> dietis extremely important. Withoutdietary treatment, your child couldbecome severely retarded. Withcareful dietary treatment, yourchild can be healthy and developnormally.In the <strong>PKU</strong> diet your child willbe on, foods that contain proteinand are, therefore, high in phenylalanine(Phe) are typically excludedfrom the diet. These include cow’smilk, meats, eggs, cheeses, nuts,peanut butter, soy drinks, and <strong>to</strong>fu.Instead, your child’s diet will consis<strong>to</strong>f a prescribed special medicalfood and low-protein foods.This prescribed special medicalfood is essential since protein andits component amino acids areneeded for normal growth anddevelopment. Nearly all proteinsare high in phenylalanine. Becausea person with <strong>PKU</strong> can’t breakdown phenylalanine <strong>to</strong> tyrosine,regular food protein will causethem <strong>to</strong> have <strong>to</strong>o much phenylalanineand not enough tyrosine intheir blood. Therefore, infants andchildren need a protein source freeof phenylalanine but high in tyrosine.The special medical foodhas little or no phenylalanine, ishigh in tyrosine, and provides agood source of vitamins andminerals. Your metabolic clinicteam will prescribe the appropriatespecial medical food for your child.Because each child has a uniqueabsolute requirement for phenylalanine,the metabolic clinic teamwill prescribe a diet tailor-made foryour child. The prescribed specialmedical food, such as a dietarypowder from the Phenyl-Free ®family of special medical foods, isthe mainstay of management of<strong>PKU</strong>. The metabolic clinic teamwill work with you <strong>to</strong> make sureyour child gets the appropriateamounts of special medical foods,as well as other foods, as your childgrows and develops. It is vitallyimportant for your child’s growthand mental development <strong>to</strong> followthe metabolic clinic’s direction onfeeding your child.Your child’s needs changeduring growing up. The metabolicclinic team will help you design adiet <strong>to</strong> provide all the calories,phenylalanine, protein, vitamins,and minerals your child needs <strong>to</strong>grow. The special medical food willnot supply all your child’s needs.As your baby grows and begins <strong>to</strong>eat solid foods, foods such as fruits,vegetables, and low-protein pastaswill be added <strong>to</strong> the diet. Thevariety of foods and dishes yourchild can enjoy is quite large.Recipes have been developedalready by other parents ofchildren with <strong>PKU</strong>. The metabolicclinic team will help you find theserecipes and ingredients.The diet for <strong>PKU</strong> is quitesimple <strong>to</strong> prepare once youunderstand what your child canand cannot eat. The metabolicclinic team will teach you how <strong>to</strong>plan your child’s daily meals. Theywill ask you <strong>to</strong> keep careful recordsof how much your child is eatingin order <strong>to</strong> balance this intake withthe amount of phenylalanine andprotein needed for growth andmental development. For yourchild <strong>to</strong> develop normally, the dietmust be maintained consistentlyand accurately. The metabolicclinic team will work closely withyou <strong>to</strong> help you in this goal.Regular Clinic VisitsMuch of your child’s treatmentfor <strong>PKU</strong> may occur at a clinic thatspecializes in this disorder, and youwill be asked <strong>to</strong> bring your childwith <strong>PKU</strong> <strong>to</strong> the clinic regularly.Your baby’s pediatrician will getreports of the clinic’s dietinstructions and your child’s bloodresults. In general, <strong>PKU</strong> clinicsdon’t handle illnesses unrelated<strong>to</strong> <strong>PKU</strong> or give routine baby shots,so it’s important for you <strong>to</strong>have a primary care provider or8
pediatrician for your baby’s othermedical care. The <strong>PKU</strong> clinic teamcan help you find a local pediatricianif necessary.The <strong>PKU</strong> clinic team willregularly need information sochanges in the diet can be made<strong>to</strong> match what your child needs<strong>to</strong> grow and develop normally.This information includes recordsof your child’s food and specialmedical food intakes, height, andweight. The clinic will also want<strong>to</strong> measure blood levels of phenylalanineregularly <strong>to</strong> make sure thatyour child has every chance ofnormal development. These visitswill give you an opportunity <strong>to</strong>discuss any questions you may havewith the metabolic clinic’s team,and the team <strong>to</strong> share with you thelatest information on <strong>PKU</strong>.Just as in the treatment of anydisease, doc<strong>to</strong>rs and nutritionistsvary in their procedures for managingphenylke<strong>to</strong>nuria. A particularclinic may differ from the followingdescription, but there willprobably be many similarities.First Steps in TreatmentFollowing the initial positiveresult for <strong>PKU</strong>, your baby will bestarted on a diet very low inphenylalanine <strong>to</strong> get his bloodphenylalanine level down quickly.This may take several days. If youare breastfeeding, the metabolicclinic doc<strong>to</strong>r will ask you not <strong>to</strong>breastfeed your baby during thistime. However, you are encouraged<strong>to</strong> continue breastfeedingyour child after his blood phenylalaninelevels are lowered, if youwish. Your baby’s metabolic clinicteam will help you plan a diet thatincludes breast milk.Next, your baby will be put ona prescribed diet, and blood levelsof phenylalanine will be checkedfrequently <strong>to</strong> be sure they aren’t <strong>to</strong>ohigh or <strong>to</strong>o low. Growth anddevelopment will be carefullyfollowed as well. Frequent visits<strong>to</strong> the clinic will be required <strong>to</strong>see how your baby is progressing.Many <strong>PKU</strong> clinics have ateam approach, and you may haveappointments with several membersof your baby’s treatment teamon the same appointment day. Thenutritionist will probably be yourprimary contact—he or she willmoni<strong>to</strong>r the therapy, adjust thediet prescription as necessary, andprovide advice when problemsarise. A physician will examineyour baby and help with problemsolving.A nurse will weigh andmeasure your child <strong>to</strong> be sure thediet is meeting growth needs. Asyour child gets older, a psychologistmay evaluate him periodically<strong>to</strong> make sure his psychologicaldevelopment is normal. A socialworker or counselor may meet withyour family <strong>to</strong> help you adjust <strong>to</strong>living with <strong>PKU</strong>.The services the clinic providesare essential <strong>to</strong> you <strong>to</strong> maximizeyour child’s development. Be assuredthe clinic team members are veryinterested in the health and developmen<strong>to</strong>f your child. You willwant <strong>to</strong> work closely with them inorder <strong>to</strong> assure your child’s maximumprogress. This will includekeeping accurate records of yourchild’s food and special medicalfood intake, cooperating with theclinic in getting the required numberof blood tests, and keepingclinic appointments. Providing therequested blood test, keeping clinicappointments, and following theclinic’s diet for your child areessential. The healthy developmen<strong>to</strong>f your child depends onthese steps.9
What Can We ExpectAs Our Child Grows?A baby with <strong>PKU</strong> who hasbeen treated from the first monthof life can be expected <strong>to</strong> growand develop much like any otherhealthy infant. Keep in mind thatall babies develop at their own rate,and even in the same family a childmay start walking or talking at adifferent age than a brother orsister did.Always feel free <strong>to</strong> discussquestions about your baby’s developmentwith your physician andthe staff at your child’s <strong>PKU</strong> clinic.Clinic specialists are available <strong>to</strong>help you manage your child’s dietthroughout the stages of development,and you can benefit fromtheir experiences with other <strong>PKU</strong>children. You may even be able <strong>to</strong>find a support group of <strong>PKU</strong>families in your area, which couldhelp you and your child discovercreative ways <strong>to</strong> deal with <strong>PKU</strong>.Since no child is just likeanother, what follows is only aguide <strong>to</strong> helping achieve normaldevelopment. It gives you an ideaof what your baby might be doingnow and what you can lookforward <strong>to</strong> in the future.Infancy: Birth <strong>to</strong> 12 Monthsof AgeBabies change very rapidlyduring the first year of life. Asparents, you will want <strong>to</strong> pay closeattention <strong>to</strong> your baby so you don’tmiss any new developments.Watch your baby—not becauseof the <strong>PKU</strong>—but because it’s fun<strong>to</strong> watch her develop.By 3 months of age, your babywill be more responsive <strong>to</strong> peopleand will smile and coo in response<strong>to</strong> your smiling and talking.Increased muscle strength andcoordination allow easy movemen<strong>to</strong>f legs and arms. When lying onhis s<strong>to</strong>mach, your baby will lifthis head and shoulders <strong>to</strong> watchwhat is going on in the room. Bythis time, you will probably feelcomfortable mixing the specialmedical food and keeping trackof your baby’s formula or breastmilk intake.At 4 <strong>to</strong> 6 months, you will beintroducing pureed foods. Yourclinic’s nutritionist will probablysuggest starting with purees ofvegetables and fruits. The additionof solid foods at this stage maymake the diet more difficult foryou until you’re used <strong>to</strong> determiningthe amount of phenylalaninein food.Most 6-month-olds havedoubled their birth weight. Bettercontrol of back and neck musclesmeans your baby will be able <strong>to</strong> sitwith only minimal support. Yourbaby will enjoy playing with hishands and simple <strong>to</strong>ys. Mostthings that your baby can holdwill go straight in<strong>to</strong> his mouth,including foods that are withinreach. You will want <strong>to</strong> have lowproteinfoods available so yourbaby can experiment with selffeeding.Low-protein foods withtexture will help support chewingand oral mo<strong>to</strong>r development and<strong>to</strong> respond <strong>to</strong> hunger withoutaffecting blood Phe levels.By 12 months, your baby willhave tripled his birth weight andwill be able <strong>to</strong> get around quitewell by crawling or walking whileholding on<strong>to</strong> furniture. He willplay more with <strong>to</strong>ys and be able<strong>to</strong> pick up the tiniest things leftwithin his reach. By this age, manybabies will also be saying a fewsimple words.As your baby grows, her growthrate will decrease. Because she isgrowing slower, she will naturallyeat less. Work with your metabolicclinic team <strong>to</strong> balance your child’sdiet with her appetite and hersocial and physical needs. You willwant <strong>to</strong> establish a pattern of mealsso she will begin <strong>to</strong> understandhunger and satiety. Feeding maybecome more difficult. When this11
occurs, feed the special metabolicproduct first followed by the lowproteinfoods your baby likes.Your baby is also developing socialskills. You will need <strong>to</strong> balanceyour approval and disapproval ofyour baby’s behavior. Food andfeeding should not become a placewhere excessive playing, pleading,or anger occurs. You could establisheating as a good area for yourbaby <strong>to</strong> assert her emerging senseof will.By the time your child reaches12 months of age, you will want<strong>to</strong> keep forbidden foods well ou<strong>to</strong>f reach. He will be much moreactive and able <strong>to</strong> explore. Youwill want <strong>to</strong> make sure that nodangerous household materialsare accessible <strong>to</strong> be picked upand placed in his mouth.Toddlers: Ages 1 <strong>to</strong> 3 YearsBy 18 months of age, yourchild will probably be able <strong>to</strong> walkalone, drink from a cup, and try<strong>to</strong> feed himself. He will try <strong>to</strong>“talk” and will understand theword “no.” His decreased appetite,desire <strong>to</strong> feed himself, and highlevel of activity will require attentiveparenting. It is important <strong>to</strong>avoid these tensions as much aspossible by positive developmentalapproaches.Establishing regular meals andsnack times, allowing extra timefor self-feeding, and <strong>to</strong>lerating theresulting mess can help your<strong>to</strong>ddler’s mo<strong>to</strong>r and social skills.Feed the special metabolic productfirst <strong>to</strong> assure adequate intake ofprotein. Try new low-protein foodsand recipes <strong>to</strong> make mealtimesmore interesting for your baby.Your <strong>to</strong>ddler will enjoy fingerfoods. By offering finger foodslowest in phenylalanine for feedingherself, it will simplify the task ofcalculating the amount of phenylalanineconsumed and enable thechild <strong>to</strong> have “more.”Two and 3 year olds are quiteactive. They progress from walkingup and down stairs with help <strong>to</strong>unlocking the front door andgoing for a “walk” on their own.The 2 year old can put twowords <strong>to</strong>gether and can make hiswants known. The 3 year old usessentences of several words andcan point <strong>to</strong> his eyes and ears.The older <strong>to</strong>ddler can go fromhappy <strong>to</strong> sad and back again at amoment’s notice. This doesn’tmean your child’s phenylalaninelevels are high, but that he isacting his age. The desire forindependence and the tantrumsthat go along with this age arealso typical and are not the resul<strong>to</strong>f <strong>PKU</strong>. If you do have anyconcerns, however, please discussthem with your clinic specialists.By 2 <strong>to</strong> 3 years, your child may12
know there are foods he can andcannot have, and you should startteaching him about his diet. Butrealize that a 3 year old does notunderstand why some foods arenot good for him (especially whenhe sees other people eating them),and he cannot be expected on hisown <strong>to</strong> refrain from eating them.Many families establish an “askbefore you eat” rule. Develop anapproach <strong>to</strong> understanding “yes”or “no” but not “maybe.”Preschoolers: Ages 3 <strong>to</strong> 5 YearsYour 3 or 4 year old isobviously no longer a baby. Hemay ride a tricycle and wash hishands unassisted. Tantrums andstubborn behavior can continuethrough 3 and 4 years of agebecause these children often want<strong>to</strong> do more than they are capableof doing and become frustrated.This frustration (not their <strong>PKU</strong>)may lead <strong>to</strong> whining and crying.Throughout the preschoolyears, your child will graduallybecome better able <strong>to</strong> understandsome things about his diet. Try <strong>to</strong>answer as many of his questions asyou can, even if it seems like youare answering the same questionsover and over. It is very importantthat you are consistent. Generally,your child will be happiest with aschedule. Promote formula firstand consistency in foods andportion size. Remember, that asyour child grows, he will havemore and more opportunities <strong>to</strong>make inappropriate food choices.Good eating patterns should befirmly established before opportunities<strong>to</strong> make inappropriate foodchoices present themselves.At age 3, your child can begin<strong>to</strong> learn about <strong>PKU</strong> as well as hisspecial diet, and he should understandthe idea of “yes” foods and“no” foods. Reading books <strong>to</strong>getherfor children with <strong>PKU</strong> can helpyou begin <strong>to</strong> teach your child aboutwhy he must follow a special diet.(See bibliography for resources.)As your child is able, you maywant <strong>to</strong> allow him <strong>to</strong> choose someof his foods and help with theirpreparation. Five and 6 year oldswill have a general idea of what isallowed on their diet but probablywon’t be able <strong>to</strong> decide if foodsthat are new <strong>to</strong> them are allowed.By 5 or 6 years, your child will bemore cooperative about his diet,particularly if he has learned thatyou won’t bend the rules.Grade School: Ages 6 <strong>to</strong> 12 YearsBy grade school, your child willbe mastering skills that she begandeveloping at earlier ages. Shewill need less help taking care ofherself and gradually will becomeindependent in eating, dressing,and bathing. Your child may like13
<strong>to</strong> ride a bicycle and visit withfriends at their homes.The thought processes of thegrade-school child are constantlydeveloping, and she will understandtime periods and how <strong>to</strong> seethings from another’s perspective.She will learn <strong>to</strong> deal with morethan one detail at a time and <strong>to</strong>relate one idea <strong>to</strong> another. At thisage, your child will reason and usesimple logic and should be encouraged<strong>to</strong> apply new math skills<strong>to</strong> her diet as she learns them.Children in early elementaryschool should begin <strong>to</strong> keep trackof their phenylalanine intake, as wellas help with making their formula.It is reasonable and necessary <strong>to</strong>involve your child more and morein his diet as he reaches school age.By later elementary school, yourchild should understand whatlevels of blood phenylalanine areacceptable and should be trackinghis own levels. As your childunderstands more about <strong>PKU</strong> andis more involved in his diet, youcanprovide opportunities for him <strong>to</strong>make decisions for himself,including calculations of Phe infoods. Parents should work withtheir children with <strong>PKU</strong> <strong>to</strong> choosefoods and plan menus, record theirdiets on the diet records, and dotheir own finger sticks for bloodsamples. The more involved yourchild is in his treatment, the morelikely he will have the knowledgeand skills <strong>to</strong> make more appropriatechoices independently. Childrenthis age prepare formula and takeresponsibility for drinking it.Adolescents: Ages 12 <strong>to</strong> 18 YearsYour adolescent may want <strong>to</strong>be independent, but he still needsparental guidance and direction.At this stage, your child should bedeveloping responsibility for hisown diet and food choices. This isgood training, not only for thechild with <strong>PKU</strong>, but also for allchildren.Most adolescents are fullycapable of understanding both<strong>PKU</strong> and the diet. Your teenagerwill be able <strong>to</strong> read and write withease and <strong>to</strong> perform math calculationsas required <strong>to</strong> manage hisdiet. He should be keeping hisown diet records and beingresponsible for clinic appointments.One aspect of adolescencethat will make dietary compliancemore difficult, however, is theneed for peer approval. Manyadolescents don’t want <strong>to</strong> be seenas any different from their friends,and having <strong>PKU</strong> can make themfeel different. These concerns maymake it difficult for them <strong>to</strong> makeappropriate food choices. Continue<strong>to</strong> actively parent your adolescent.Provide positive support and helphim develop strategies for dealingwith his peers—your child has noreason <strong>to</strong> feel different if he hasthe skill, knowledge, self-esteem,and parental support you haveprovided.14
Maternal <strong>PKU</strong>:When Your Daughter IsReady To Have ChildrenIn the past, children with <strong>PKU</strong>were usually permitted <strong>to</strong> discontinuetreatment (and have elevatedblood phenylalanine levels) beforeadolescence. However, severalstudies have shown that childrenwho discontinue treatment or havehigh Phe levels have more difficultieswith thinking processes andmath skills. Other studies havefound that elevated blood phenylalaninelevels in older patientswere associated with behavior andlearning problems which werereversed when the patientsreturned <strong>to</strong> more restricted diets.For these reasons, most clinics arenow recommending that personswith <strong>PKU</strong> remain on the diet forlife. This “diet for life,” whichmeans good Phe levels for life, isa strong recommendation—discontinuing treatment is notadvised at any age.As they begin their menstrualcycles, girls with <strong>PKU</strong> shouldunderstand the effect <strong>PKU</strong> canhave on developing babies.High blood levels of phenylalanineare very damaging <strong>to</strong> adeveloping fetus.Researchers have found that, asthe mother’s blood phenylalaninelevels increase, her chance ofhaving a baby with an abnormallysmall head and mental retardationalso increased. Incidence of lowbirth weight and congenitalheart disease appears <strong>to</strong> increasemarkedly when serum phenylalaninelevels are consistently abovethe “good level.” In women whohave not stayed on the diet, it isnecessary <strong>to</strong> reinstate dietarytherapy before conception. Theprognosis for having a normalchild is better, but it is criticalthat diet therapy begins beforeconception. The fetus is verysensitive <strong>to</strong> high levels ofphenylalanine. The early monthsof pregnancy are believed <strong>to</strong> bethe most crucial for normaldevelopment.For these reasons, it’s veryimportant that women with<strong>PKU</strong> follow their phenylalanine-restricted diet before conceivingand throughout pregnancy.Because it’s so difficult <strong>to</strong> go back<strong>to</strong> the diet after being off it, it isespecially important that womencontrol their blood phenylalaninefor a lifetime.15
Questions Parents Often AskDid something happen duringmy pregnancy that could havecaused my baby <strong>to</strong> be bornwith <strong>PKU</strong>?No. <strong>PKU</strong> is inherited fromboth parents. Only when theuniting sperm and egg bothcontain the gene for <strong>PKU</strong> willthe baby develop this condition.How can you tell who is acarrier of <strong>PKU</strong>?When a child is born with <strong>PKU</strong>,we know that both parents are carriersfor the altered <strong>PKU</strong> gene.Consult with your genetic counselorabout determining who else inyour families may be carriers.Siblings of a child with <strong>PKU</strong>have a 50% chance of being carriersfor <strong>PKU</strong>. Therefore, they maywant <strong>to</strong> have carrier testing doneon themselves before they begin afamily. If they know they are carriersof <strong>PKU</strong> but are unsure of the<strong>PKU</strong> status of their spouses, theywill want <strong>to</strong> be certain that earlyscreening is done on any childrenthey may have.If we have one child with <strong>PKU</strong>,how will this affect the possibilityof having future children with<strong>PKU</strong>?When both parents are carriersfor the altered gene, there is a onein four chance with each pregnancythat <strong>PKU</strong> will occur. Therefore,you have a 25% chance of havinga baby with <strong>PKU</strong> each time youare pregnant.How many people in the generalpopulation are carriers of <strong>PKU</strong>?One in 50 <strong>to</strong> one in 70. Thisnumber is slightly higher in somepopulations and lower in others.Every person carries several geneswhich, like the <strong>PKU</strong> gene, cancause a variety of inherited disorders.Carriers for the altered <strong>PKU</strong>gene are not different from thegeneral population nor do theyhave any abnormalities resultingfrom being a carrier.What will happen <strong>to</strong> my childwith <strong>PKU</strong> when she marriesand has children?If the father is a carrier for thealtered <strong>PKU</strong> gene, a child theyhave would have a 50% chance ofhaving <strong>PKU</strong>. If the father is nota carrier, none of their childrenwould have <strong>PKU</strong>, but all childrenwould be carriers.What is “Maternal <strong>PKU</strong>?”This is the term given <strong>to</strong> thespecial problems that can occurwhen a woman with <strong>PKU</strong> haschildren. Women with <strong>PKU</strong> need<strong>to</strong> understand that if they becomepregnant when their blood phenylalaninelevels are high, there is agreater chance the baby may beborn with birth defects or developmentaldelays. Being on a very lowphenylalanine diet prior <strong>to</strong> conceptionand throughout pregnancyreduces the risk of these problems.If we have a child with <strong>PKU</strong> inthe family, how will this affectthe lives of our other children?Having a child with specialhealth needs causes some changesin attitudes and family routine.For example, eating habits mayhave <strong>to</strong> be adjusted, and the childwith <strong>PKU</strong> may seem <strong>to</strong> get moreattention than the childrenwithout <strong>PKU</strong>. Parents have <strong>to</strong> be16
careful not <strong>to</strong> center their attentionon the child with <strong>PKU</strong>, particularlyat mealtimes. Older brothers andsisters may try <strong>to</strong> “mother”the child with <strong>PKU</strong>, and siblingsmay even taunt the child withfoods he cannot eat. Parents willhave <strong>to</strong> make it very clear thatsuch behavior is not acceptable.What is the <strong>PKU</strong> diet?It is a diet low in phenylalanine,which is the amino acid that thechild’s body cannot use properly.The specific diet for your child willbe specially designed by your metabolicphysician and nutritionist.The diet is designed <strong>to</strong> meet yourchild’s individual needs for growthand development. The dietincludes a protein substitute, suchas Phenyl-Free ® 1 or Phenyl-Free 2dietary powder, which provides themissing protein but has little or nophenylalanine. In addition <strong>to</strong> theseproducts, patients are given a prescribedspecific amount of phenylalaninefrom breast milk, regularinfant formula, or solid foods <strong>to</strong>provide enough phenylalanine forgrowth. Measured amounts offruits, vegetables, cereals, lowproteinbreads, pasta, and specialdesserts are added <strong>to</strong> the diet as thechild gets older.Is the diet expensive?The formula costs more thanregular infant formula because itis specially designed for medicalpurposes. However, because of theimportance of formula for yourchild’s mental and physical development,most health insuranceplans pay for it. In some states, thespecial medical formula is providedby the State Department of Health.In other states, these products areprovided on a sliding fee scale,based on ability <strong>to</strong> pay. The socialworker, nutritionist, or nurse atthe <strong>PKU</strong> clinic can usually helpidentify a payment method.Can I breastfeed mybaby with <strong>PKU</strong>?Yes. Breast milk is lower inphenylalanine than either infantformulas or cow’s milk, and it canprovide the supplemental amountsof phenylalanine required for yourbaby’s growth when used with aspecial phenylalanine-free formulasuch as Phenyl-Free 1. Many newbornbabies with <strong>PKU</strong> can be fedwith breast milk and phenylalanine-freeformulas and still keeptheir blood levels in an acceptablerange. All babies with <strong>PKU</strong> musthave their diet intake and bloodphenylalanine levels moni<strong>to</strong>redclosely. You’ll want <strong>to</strong> discuss yourdecision <strong>to</strong> breastfeed your babywith <strong>PKU</strong> with your baby’sdoc<strong>to</strong>r and dietitian.Why are diet diaries kept?Diet diaries are records of foodintake which serve as guides for theclinic team when adjusting yourchild’s diet. These diaries are anecessary management <strong>to</strong>ol. It isthe only way for the nutritionist <strong>to</strong>know exactly what your child hasbeen eating or drinking so thatappropriate changes can be made<strong>to</strong> assure the proper levels ofblood phenylalanine.How long will my child with<strong>PKU</strong> be on the diet?Medical experts state thatmaintaining the restricted dietthroughout life is preferable. Datafrom the National CollaborativeStudy of Children Treated for <strong>PKU</strong>show that intellectual ability andacademic achievement in schoolare negatively affected when bloodlevels are persistently high beforethe age of six years. Other studieshave shown that children whomaintained acceptable levels ofblood phenylalanine through age10 had higher IQ scores thanchildren who didn’t have low Phelevels. A “diet for life” approach iscurrently recommended.17
What happens if my child with<strong>PKU</strong> refuses <strong>to</strong> eat part or all ofhis prescribed diet?If this goes on for only afew days, it is not a problem.However, if the child gets in<strong>to</strong> apattern of eating only one kindof food, the prescribed amountsof food and formula may not beingested. Don’t worry if this goeson for a day or two. If youdevelop a pattern of specialmetabolic products along withregular meals, your child will probablynot refuse <strong>to</strong> eat for a longerperiod than one or two days. If shedoes, it’s a good idea <strong>to</strong> check withthe metabolic clinic team <strong>to</strong> ruleout a health problem requiringtreatment. Call your <strong>PKU</strong> clinicfor help in adjusting the diet duringthese times, rather than trying<strong>to</strong> adjust the diet yourself. Staff atthe clinic will suggest other ways <strong>to</strong>get your child <strong>to</strong> eat and <strong>to</strong> assureadequate intake in cases of fever,vomiting, and/or diarrhea, or otherchildhood diseases which result inloss of appetite.Will my child get sick if he doeseat some high-protein food?No. There may be an elevationin blood phenylalanine levels thatwill gradually decrease if furtherPhe intake is restricted. However,frequently high levels of bloodphenylalanine can affect yourchild’s development, even thoughhe may not show obvious physicalsigns of <strong>to</strong>xicity.What are “good” bloodphenylalanine levels?Most clinics generally regardthe range of 2-6 mg/dL as “good”blood phenylalanine levels. Pleaseconsult your clinic about what isa good level for your child.What causes blood phenylalaninelevels <strong>to</strong> go up?In most cases, elevated phenylalaninelevels may indicate thatyour child is eating more phenylalanine-containingfoods than heshould eat <strong>to</strong> meet his growthneeds. If your child is not gettingenough of his special metabolicproduct, his body will break downmuscle and other protein s<strong>to</strong>res,thereby releasing phenylalaninein<strong>to</strong> the blood. Illness can alsocause this breakdown and makeblood phenylalanine levels rise. Ifyour child is growing rapidly, hemay need extra amounts of food orspecial metabolic product, whichcan cause a change in bloodphenylalanine.What causes blood phenylalaninelevels <strong>to</strong> go down?When a child’s diet is changedfrom regular food <strong>to</strong> a phenylalanine-restricteddiet, levels of bloodphenylalanine will go down.18Generally, when a child’s prescribeddiet is appropriate for herage and rate of growth, and thediet is closely adhered <strong>to</strong>, phenylalaninelevels should be within thedesired range. A level below therange suggests your child is noteating all her “Phe foods.”Will my child become retarded?With early dietary treatment,careful dietary management, andresulting good blood Phe levels,the chances are very good that yourchild will grow and developnormally.Will my child with <strong>PKU</strong> lookor act differently than otherchildren?If he has received early treatmentand adhered <strong>to</strong> the dietprescribed by your metabolic clinicstaff, your child with <strong>PKU</strong> shouldnot look or act differently thanother children.Will my child be sickly?Having <strong>PKU</strong> will not causeyour child <strong>to</strong> have poor health.Will my child be able <strong>to</strong> go <strong>to</strong>regular schools?If your child is treated early andcarefully, his <strong>PKU</strong> will not preventhim from attending regular schools.
Tips For ParentsThe following tips are compiledfrom the experiences ofmany families living with <strong>PKU</strong>.As you become more comfortablewith the <strong>PKU</strong> diet, you likely willdiscover other ways <strong>to</strong> effectivelymanage the disorder. You shouldalways discuss ideas with the clinicfirst before making any changes.• Remember that you aren’tmanaging the diet of yourchild alone. The whole family,as well as neighbors andfriends, should be instructedabout diet restrictions.• Estimate how long yoursupply of formula will last,then order early so you don’thave <strong>to</strong> worry about runningout. Remember that you maynot be able <strong>to</strong> go out <strong>to</strong> thes<strong>to</strong>re and buy an extra can ofPhenyl-Free ® 1, Phenyl-Free 2,or any other <strong>PKU</strong> formula ifyou run out.• Don’t change <strong>to</strong>o many thingsat one time during the transitionfrom pureed foods <strong>to</strong> selffeeding.Work in consultationwith your clinic nutritionist sothis transition can be completedeasily and in a stepwise manner.• Keep in mind that duringillness or fever, bloodphenylalanine levels mayrise. Consult your clinic forguidance on how <strong>to</strong> minimizethis effect of illness.• Include your child’s needs inthe family meal plan. Try <strong>to</strong>make meals containing foodsthat your child can eat.• Keep reconstituted products ina well-marked container that isdifferent from any other containerin the refrigera<strong>to</strong>r sothat your child can easilyidentify “her” milk substitute.• Involve your child with <strong>PKU</strong>in the management of his owndiet when possible. This couldinclude helping <strong>to</strong> mix his formula,making his sandwich forlunch, or making treats from alow-protein cookie or cakerecipe.• Be consistent in your approach<strong>to</strong> the diet. A matter-of-factbut firm attitude will helpyour child adjust more easily<strong>to</strong> diet restrictions. Keep inmind that all children testtheir parents, and your childwith <strong>PKU</strong> probably will be nodifferent. When diet restrictionsare followed regularly,forbidden foods may lose someof their appeal.• Avoid the habit of snackingcontinuously. If your childneeds <strong>to</strong> eat between meals,make that snack an event of itsown which you or a caregiversupervises. You may want <strong>to</strong>have a “tea party” when yourchild wakes up from his afternoonnap. He will be lessinclined <strong>to</strong> help himself <strong>to</strong>snack foods when he knowsthere will be a defined snacktime.• Don’t let your child sampleunallowed foods just <strong>to</strong> tastethem. Your child is better offnever having tasted foods that,once tried, may become evenmore appealing.• Never let your child know youfind the smell or taste of theformula objectionable.Hints While Traveling• Always take morePhenyl-Free 1, Phenyl-Free 2,or any other <strong>PKU</strong> formulathan you will need when youleave home, since it may bevery difficult for you <strong>to</strong> get itin another state or country.• Put premeasured amounts offood in<strong>to</strong> small containers <strong>to</strong>simplify calculating yourchild’s intake.19
• Measure the Phenyl-Free ® 1,Phenyl-Free 2, Phenyl-Free 2HP,or any other <strong>PKU</strong> formula in<strong>to</strong>individual baggies or other smallplastic bags. You may find that asmall shaker works well for mixingthe products.• Once your child is eating foodsfrom the table, you can ordervegetables and fruit for him atrestaurants so he feels like eatingout is a treat.• Always carry low-phenylalaninesnacks, such as fruit, low-proteincookies, and candy. If your familyhas ice cream, get a non-milk,iced popsicle for your child with<strong>PKU</strong>.Helping Your School-AgedChild With The Diet• Teach your child how <strong>to</strong> dealwith questions about his dietfrom classmates. Think up goodanswers <strong>to</strong>gether before he startsschool.• Be sure your child’s teachers andlunchroom supervisor know ofthe diet for <strong>PKU</strong> and its importance<strong>to</strong> his health. Most schoolpersonnel will be very happy <strong>to</strong>help. It may be useful for you <strong>to</strong>give the teacher a guide <strong>to</strong> whatkinds of snack foods your childcan have. Children often bringcupcakes or cookies <strong>to</strong> school <strong>to</strong>celebrate birthdays or other holidays,and if your child can alsohave a special treat then he won’tfeel so different from his friends.• With some practice, you can helpyour child pack a lunch thatlooks like other kids’ lunches. Ifyou put cold formula in an insulatedlunch bag in the morning,it will usually stay cold untillunch time. Measure out thefoods your child should eat andpack these in small containers orbaggies. Low-protein bread forsandwiches, raw vegetables, fruits,and low-protein cookies can helphis lunch look “normal.” If yourchild knows <strong>to</strong> bring home anyuneaten foods from his lunch,you can keep better track of whathe needs for supper <strong>to</strong> meet hisdaily requirements.• Encourage your child <strong>to</strong> participatein school activities, eventhough arrangements may have<strong>to</strong> be made for meals. The dietfor <strong>PKU</strong> should be treated as asmall inconvenience in an otherwisenormal life.• Develop the habit of treatingeach day as important <strong>to</strong> thehealth of your child. In addition<strong>to</strong> keeping a 3-day diet recordbefore blood tests, it is helpful <strong>to</strong>keep a daily food diary. This willhelp you stay in the habit ofrecording your child’s diet. Aspiral-bound notebook kept inthe kitchen works well for thispurpose, and you can also note ifyour child is sick. Then, when hisblood level is high, you can goback through the food diary andtry <strong>to</strong> determine what caused it.• Teach your child the need <strong>to</strong> beaware of what she eats and beconsistent in drinking the specialmetabolic product. Help yourchild learn <strong>to</strong> make appropriatefood choices.20
Glossary Of TermsAssociated With <strong>PKU</strong>Amino acids are building blocksof proteins. Phenylalanine and tyrosineare amino acids. Some aminoacids are made by the body, but“essential” amino acids are not andmust be supplied in the diet. Phenylalanineis an essential amino acid.Au<strong>to</strong>somal recessive is a form ofinheritance requiring the presence oftwo genes for a trait in order for theindividual <strong>to</strong> show the trait. Personswith only one of an au<strong>to</strong>somal recessivegene pair are carriers of the traitbut are unaffected by the trait.Blood levels of phenylalanine aredetermined by tests done on bloodafter it is drawn from the heel, <strong>to</strong>e, orfinger. Blood levels of phenylalanineshould be in the range of 120-360umol/L (2-6 mg/dL).Collaborative study is a researchstudy on <strong>PKU</strong>. Because no one clinicin the country has enough patientswith <strong>PKU</strong> <strong>to</strong> answer all the questionswe have about the disorder, severalmajor medical centers collaborated ingathering data <strong>to</strong> learn more about<strong>PKU</strong> and improve treatmentmethods. This long-term projectdetermined much of what we nowknow about <strong>PKU</strong>, and researchcontinues at many <strong>PKU</strong> clinics.Enzymes are proteins responsiblefor causing or speeding up biochemicalreactions without being alteredthemselves by the reactions. Theenzyme phenylalanine hydroxylasecauses phenylalanine <strong>to</strong> be brokendown in<strong>to</strong> tyrosine.Equivalent or exchange is ameasured amount of food, such ascereal, vegetable, or fruit, that hasa certain amount of phenylalanine.Some clinics use an “exchange”system <strong>to</strong> calculate intake ofphenylalanine. An “exchange”contains approximately 15 milligramsof phenylalanine. Patients on dietsfor treatment of <strong>PKU</strong> should eat alimited number of exchanges per day,determined in consultation with theirnutritionist and based on their sizeand growth needs.Genetics is the study of howcharacteristics are inherited. Genescontain information the body uses <strong>to</strong>produce a specific trait or <strong>to</strong> performa particular body function.Growth measurements help youand the <strong>PKU</strong> clinic team know thatyour child is growing properly. Thesemeasurements are made at varioustimes for all children, not just forchildren with <strong>PKU</strong>. They typicallyinclude measures of your child’s height,weight, and head circumference.Guthrie test is a blood test usedin screening for <strong>PKU</strong>; newbornscreening is manda<strong>to</strong>ry in the UnitedStates. It does not actually diagnoseyour child with <strong>PKU</strong>, but it indicates<strong>to</strong> the physician that your child has ahigh probability of having <strong>PKU</strong>.Further tests are needed <strong>to</strong> make adefinite diagnosis.Hyperphenylalaninemiais a term meaning high levels ofphenylalanine in the blood. It21is a group of disorders in whichelevated blood phenylalanine levels area primary characteristic.Phenylalanine is one of severalamino acids that make up proteins.A certain amount of phenylalanineis needed for normal growth anddevelopment. Because the bodycannot make phenylalanine, it mustbe supplied in the diet. Phenylalanineis an “essential” amino acid.Phenylke<strong>to</strong>nuria (<strong>PKU</strong>) is aninherited disorder in which the bodylacks the enzyme needed <strong>to</strong> convertphenylalanine <strong>to</strong> tyrosine. In <strong>PKU</strong>,excess phenylalanine accumulates inthe blood and tissues and can damagethe brain and nervous system ifleft untreated.Tyrosine is an amino acid whichis needed for normal growth anddevelopment. It is typically madeby the body from phenylalanine, butthe person with <strong>PKU</strong> can’t make thisamino acid and must get it from hisdiet. Tyrosine is present in phenylalanine-freeformulas suchas Phenyl-Free ® 1, Phenyl-Free 2,and Phenyl-Free 2HP.
Where To Go For More InformationDiet ManagementA Babysitter’s <strong>Guide</strong> <strong>to</strong> <strong>PKU</strong>.Trahms CM, Cox C. Available fromthe <strong>PKU</strong> Clinic at the University ofWashing<strong>to</strong>n, Seattle, WA. Telephone:(206) 685-3015.Finger Foods are Fun. Trahms CM,Cox C, Luce P, Padgett D. Availablefrom the <strong>PKU</strong> Clinic at theUniversity of Washing<strong>to</strong>n, Seattle,WA. Telephone: (206) 685-3015.Games that Teach: Learning byDoing for Preschoolers with <strong>PKU</strong>.Trahms CM, Cox C, Luce P.Available from the <strong>PKU</strong> Clinic atthe University of Washing<strong>to</strong>n, Seattle,WA. Telephone: (206) 685-3015.New Parents’ <strong>Guide</strong> <strong>to</strong> <strong>PKU</strong>.Trahms CM, Luce P. Available fromthe <strong>PKU</strong> Clinic at the University ofWashing<strong>to</strong>n, Seattle, WA.Telephone: (206) 685-3015.A Teacher’s <strong>Guide</strong> <strong>to</strong> <strong>PKU</strong>.Kaufman M, Nardella M.Office of <strong>Nutrition</strong> Services, ArizonaDepartment of Health Services,1740 W. Adams Street,Phoenix, AZ 85007.Cookbooks & Food ListsChef Lophe’s Phe-NominalCookbook. Barr LA, Trahms CM.Available from the <strong>PKU</strong> Clinic atthe University of Washing<strong>to</strong>n,Seattle, WA.Telephone: (206) 685-3015.Low Protein Bread Machine Bakingfor <strong>PKU</strong>. Schuett VE. 92 recipes forlow protein bread baking using breadmachines. See www.pkunews.org forordering information.Low Protein Cookery for <strong>PKU</strong>,2nd edition. Schuett VE. Over450 recipes for the <strong>PKU</strong> diet withphenylalanine, protein, and caloriecontent; suggestions for managingthe diet. See www.pkunews.org forordering information.Low Protein Food List for <strong>PKU</strong>.Schuett VE. Over 3,000 foods(including brand names) withphenylalanine, protein, and caloriecontent. See www.pkunews.org forordering information.Making the Change from High Phe<strong>to</strong> Low Phe: Changing recipes <strong>to</strong>fit your low phenylalanine mealpattern. Fink KJ, Trahms CM.Available from the <strong>PKU</strong> Clinic atthe University of Washing<strong>to</strong>n, Seattle,WA. Telephone: (206) 685-3015.Creative Family Cooking.The Mid Atlantic Connection for<strong>PKU</strong> and Allied Disorders.P.O. Box 6086,Lancaster, PA 17607.General InformationCoping with <strong>PKU</strong>: results ofnarrative interviews with parents.Awiszus D, Unger I. Euro J Pediatr.1990;149(suppl 1):S45-51.Intellectual development in12-year-old children treated forphenylke<strong>to</strong>nuria. Azen CG, Koch R,Friedman EG, Berlow S, Coldwell J,Krause W, et al. Am J Dis Child.1991;145(1):35-39.After a positive Guthrie—what next? Dietary managementfor the child with phenylke<strong>to</strong>nuria.Clark BJ. Euro J Clin Nutr.1992;46(suppl 1):S33-39.Intelligence in mild atypical <strong>PKU</strong>.Costello PM, Beasley MG, TillotsonSL, Smith I. Euro J Pediatr.1994;153(4):260-263.Breast-feeding in the managemen<strong>to</strong>f the newborn withphenylke<strong>to</strong>nuria: a practicalapproach <strong>to</strong> dietary therapy.Greve LC, Wheeler MD, Green-Burgeson DK, Zorn EM. J Am DietAssoc. 1994;94(3):305-309.Maternal <strong>PKU</strong> collaborative study:the effect of nutrient intake onpregnancy outcome. Matalon R,Michals K, Azen C, et al. J InheritMetab Dis. 1991;14(3):371-374.Updated in 1996.Recommendations on the dietarymanagement of phenylke<strong>to</strong>nuria.Report of Medical Research WorkingCouncil Working Party on phenylke<strong>to</strong>nuria.Arch Dis Child.1993;68(3):426-427.22
For ordering information, call 800-BABY123 ororder online at www.s<strong>to</strong>re.enfamil.comLF870 REV 2/07©2007 <strong>Mead</strong> <strong>Johnson</strong> & Company