louisiana standardized credentialing application - MultiPlan
louisiana standardized credentialing application - MultiPlan
louisiana standardized credentialing application - MultiPlan

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
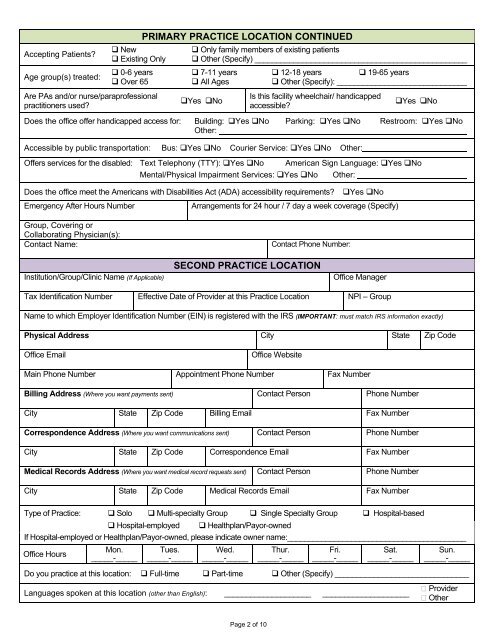
Accepting Patients?Age group(s) treated: New Existing Only 0-6 years Over 65Are PAs and/or nurse/paraprofessionalpractitioners used?PRIMARY PRACTICE LOCATION CONTINUED Only family members of existing patients Other (Specify) _________________________________________________ 7-11 years All AgesYes No 12-18 years 19-65 years Other (Specify): ______________________________Is this facility wheelchair/ handicappedaccessible?Yes NoDoes the office offer handicapped access for: Building: Yes No Parking: Yes No Restroom: Yes NoOther:Accessible by public transportation: Bus: Yes No Courier Service: Yes No Other:Offers services for the disabled: Text Telephony (TTY): Yes No American Sign Language: Yes NoMental/Physical Impairment Services: Yes No Other:Does the office meet the Americans with Disabilities Act (ADA) accessibility requirements?Emergency After Hours NumberYes NoArrangements for 24 hour / 7 day a week coverage (Specify)Group, Covering orCollaborating Physician(s):Contact Name:Contact Phone Number:Institution/Group/Clinic Name (If Applicable)SECOND PRACTICE LOCATIONOffice ManagerTax Identification Number Effective Date of Provider at this Practice Location NPI – GroupName to which Employer Identification Number (EIN) is registered with the IRS (IMPORTANT: must match IRS information exactly)Physical Address City State Zip CodeOffice EmailOffice WebsiteMain Phone Number Appointment Phone Number Fax NumberBilling Address (Where you want payments sent) Contact Person Phone NumberCity State Zip Code Billing Email Fax NumberCorrespondence Address (Where you want communications sent) Contact Person Phone NumberCity State Zip Code Correspondence Email Fax NumberMedical Records Address (Where you want medical record requests sent) Contact Person Phone NumberCity State Zip Code Medical Records Email Fax NumberType of Practice: Solo Multi-specialty Group Single Specialty Group Hospital-based Hospital-employed Healthplan/Payor-ownedIf Hospital-employed or Healthplan/Payor-owned, please indicate owner name:__________________________________________Office HoursMon._____-_____Tues._____-_____Wed._____-_____Thur._____-_____Fri._____-_____Sat._____-_____Sun._____-_____Do you practice at this location: Full-time Part-time Other (Specify) _______________________________Languages spoken at this location (other than English): ____________________ ____________________ Provider OtherPage 2 of 10