Download - Belgian Cancer Registry
Download - Belgian Cancer Registry
Download - Belgian Cancer Registry
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
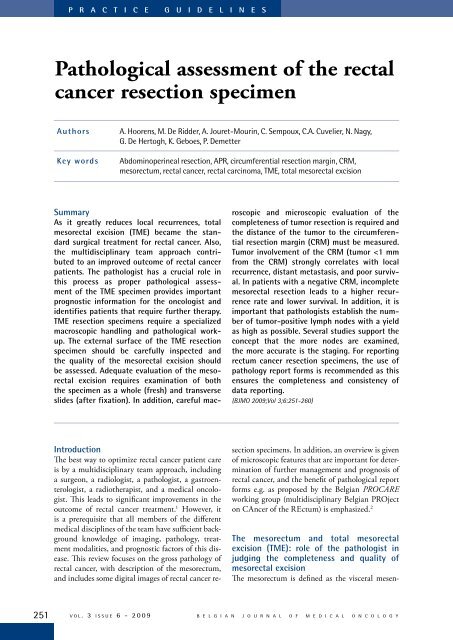
ABFigure 1. Anterior (A) and posterior (B) view of a TME resection specimen.tery surrounding the rectum. It is a fatty connectivetissue layer, enveloped by a thin fascia. It is thecontinuity of the mesosigmoid which progressivelysurrounds the whole rectum under the peritonealreflection of the pouch of Douglas. It contains theblood vessels as well as the lymphatic ducts andlymph nodes of the rectum. In 1982, Heald et alintroduced the concept of “Total Mesorectal Excision(TME)”, leading to improved patient outcome,particularly with regard to local recurrence. 3 Thisconcept includes 2 aspects: firstly, an anatomicalsharp dissection under direct vision in the planethat separates the visceral mesorectal fascia from theparietal pelvic fascia (“the holy plane”), without anytearing or disruption of the mesorectal circumferentialfascia and with preservation of the surroundingnerve plexuses; and secondly, the resection of themesorectum down to the striated pelvic floor (thelevator muscles), avoiding to leave in place its mostdistal part, potentially the site of foci of tumor celldeposits. This also facilitates low anastomosis andsphincter-preservation. For cancer of the upperthird of the rectum a “Partial Mesorectal Excision(PME)” can be performed. 4 In this case the mesorectaldissection is conducted 5 cm distally to the loweredge of the tumor (measured in situ) in a plane at90° to the rectal wall with sharp mesorectal dissection,differencing this procedure from the formerlyperformed conventional blunt digital dissection ofanterior resection (AR).A multidisciplinary team approach has led to significantimprovements in outcome of rectal cancertreatment. 1 The pathologist has a crucial role in thisprocess, not only by determining the pathologicalstage of rectal cancer, but also by the assessmentof the completeness of tumor resection and assessmentof the quality of the mesorectal excision. 5,6Macroscopic as well as microscopic evaluation ofthe circumferential resection margin of the (TME)specimen by the pathologist has been shown to beof paramount importance. 5,6 The circumferentialresection margin (CRM) is the surgically-createdplane of dissection produced during the removalof the rectum from its surrounding tissue. It is thenon-peritonealised bare area of the resection specimen.The largest area is located posteriorly, whereit begins much higher than anteriorly, at the mesocolonof the sigmoid and extends downwards as anenlarging triangle. 7 Below the peritoneal reflectionit becomes a circumferential margin and extendsdownwards to the bottom of the mesorectum andthe distal excision margin or, in an APR, down toB E L G I A N J O U R N A L O F M E D I C A L O N C O L O G Y v o l . 3 i s s u e 6 - 2 0 0 9 252
P R A C T I C E G U I D E L I N E SFigure 2. Severely irregular mesorectum in an APR specimen: the muscle layer is visible about 1 cm below the peritoneal reflection.The description of the quality of the mesorectal surface in an APR specimen is limited to the description of the rectumabove the sphincters.the anal skin (Figure 1). 7 Tumor involvement of theCRM is the single most important factor for predictingthe risk of local recurrence in rectal cancerpatients. 6,8-10 It is also important in the predictionof distant metastasis and overall survival. 10 Tumorswithin 1 mm of the surgically created margin havea greatly increased risk of recurrence. 8,9 One studystill showed a high incidence of recurrence at 2 mm,but this finding could not be confirmed in subsequentstudies. 1,11,12For very low primary rectal tumors an abdominoperinealresection (APR) is required. Mesorectal excisionin this case will remove lymphatic, vascular,and neural pathways of metastasis, but there will oftenbe involvement of the surgical resection marginat the level of the sphincters. 13,14 The tapering of themesorectum towards the levators emphasizes thatthere is less tissue for the carcinoma to transverse beforeinvolving the surgical plane of resection in thelow mesorectum and anal canal. In addition, goodvisualization and access are limited with the classicalapproach of APR and it was shown that the planeof resection lies within the sphincter muscle, thesubmucosa, or lumen in more than one third of theAPR cases. In the remainder, the plane of resectionlies on the sphincteric muscles. 14 This predisposes tocircumferential resection margin (CRM) involvement,except in the very early stages. In addition, ahigh intra-operative perforation rate was observed. 14Neoadjuvant therapy has an important place here indownsizing the tumor, enabling complete resection.Moreover, a more radical operation with a predominantlyperineal surgical approach, creating a CRMoutside the levators and giving wider clearance is beingconsidered for low rectal tumors. 13,14Gross external appearance of the surgicallyresected specimen: macroscopic inspectionThe first task of the pathologist when receiving thesurgical excision specimen following TME is thevisual inspection of the completeness of resectionof the mesorectum. 5-8,15 Preferentially, the resectionspecimen should be examined in the fresh, unfixedstate. More importantly however, is that it shouldbe delivered unopened to the pathologist. The externalsurface of the TME should be carefully inspectedand the quality of the mesorectal excisionshould be assessed and can be graded (complete,nearly complete, incomplete). 5,6 The mesorectalsurface of a good resection should be smoothwith a good bulk of mesorectum. There should beno coning near the distal margin. Defects at thesurface should be less than 5 mm deep. In case ofperforation of the resection specimen or in case themuscular layer is visible exteriorly, the resectionis classified as incomplete (Figure 2). In the PRO-CARE protocol the following terminology is used:smooth and regular, mildly irregular or severely irregular(Table 1). 2 This slightly adapted terminologywas introduced to avoid misinterpretation ofthe notion of “incomplete” resection, as in case ofadvanced tumor growth it is not always possible toavoid margin involvement. A Dutch study demonstratedthat despite extensive surgical training only57% of operations were judged to be complete excisionsand nearly one quarter (24%) were classifiedas incomplete excisions. 5 In resection specimens reportedto be incomplete, there was a significantlyhigher rate of circumferential margin involvementand a higher rate of overall recurrence and local tumorrecurrence. 5 In patients with a positive CRM,253v o l . 3 i s s u e 6 - 2 0 0 9B E L G I A N J O U R N A L O F M E D I C A L O N C O L O G Y
Table 1. Grading of the quality of mesorectal excision in TME specimens as proposed in the PROCARE guidelines.Both the specimen as a whole (fresh) and transverse slices (after fixation) should be examined in orderto allow adequate evaluation of the mesorectal excision.Smooth, regular - intact mesorectum with only minor irregularities of a smooth mesorectal surface- no defect deeper than 5 mm- no coning toward the distal margin of the specimen*- a smooth circumferential resection margin on slicingMildly irregular - moderate bulk to the mesorectum, but irregularity of the mesorectal surface- moderate coning of the specimen allowed*- the muscularis propria invisible at every site, with the exception of the insertion of thelevator musclesSeverely irregular - little bulk to the mesorectum with defects down onto the muscularis propria and/orvery irregular circumferential resection margin on slicing* Coning refers to the tendency for the surgeon to cut towards the rectum wall during distal dissection, rather thanstaying outside of the visceral mesorectal fascia; this gives a conical appearance to the surgical resection specimen.assessment of the quality of surgery added nothingto the prediction of local recurrence above CRMinvolvement alone. However, in patients with anegative CRM and incomplete resection, the overallrecurrence rate was doubled from 15 to 29% andsurvival decreased from 91 to 77%. 5 No prognosticdifference was observed between patients witha complete mesorectum compared to those with anearly complete mesorectum. 5It is important to realize that there is less mesorectaltissue anteriorly and laterally than posteriorly.7 In addition the size of the mesorectum varieswidely between individuals and is related to severalfactors such as to body mass, gender, and degree ofcachexia. 16In an APR specimen, the description of the qualityof the mesorectal surface is limited to the descriptionof the rectum above the sphincter.Handling the TME specimenThe relation of the tumor to the serosal surfaceshould be determined, i.e. above, at, or belowthe peritoneal reflection. After examination ofthe external surface, the resection margin shouldbe painted with india ink. The resection specimenis opened anteriorly above the peritonealreflection starting at its proximal end withoutextension into the tumor. This allows effectiveevaluation of the anterior CRM that would otherwisebe destroyed by the opening process. Ideally,the resection specimen should be pinnedout on a corkboard to avoid shrinkage and leftfloating with the cork upwards in formalin fixativefor at least 48 hours. 18 Placement of gauze orpaper tissue wick soaked in formalin within thelumen of the intact bowel segment is necessaryto enhance fixation. After fixation, the resectionspecimen should be sectioned in parallel cuts of3-4 mm intervals, perpendicularly to the lengthof the bowel. The long fixation time is required tomake the tissue firmer and facilitates serial crosssectionalslicing of the specimen. This allows theassessment of the deepest point of tumor invasionand to measure the distance to the place where thetumor is closest to the CRM. The number of tissueblocks to be taken from the tumor is 3 at minimum.2 At least one tissue block should include thetransition from the surrounding normal mucosa tothe tumor and at least one tissue block should betaken of the deepest point of invasion. 2,19 The latterpermits microscopic confirmation and refinementof gross observations at the area of greatest macroscopicconcern. It is known that, in particular afterradiotherapy, the presence of fibrosis may makemacroscopic assessment of the tumor inaccurate. Itis often impossible to distinguish therapy-inducedfibrosis from tumor invasion. 20 In this case, sufficienttissue blocks should be taken from all macroscopicallysuspected areas in order not to miss thedeepest point of invasion. No distinction should bemade between various modes of involvement of theCRM, continuous spread, discontinuous tumordeposits, or involved lymph nodes. The orientationof grossly suspicious nodes that are closely relatedto the CRM should thus be preserved in sections.Tissue slices can be embedded as large-area (giant)blocks or as conventional small blocks. Formalinfixation will allow additional molecular pathologicalexamination.B E L G I A N J O U R N A L O F M E D I C A L O N C O L O G Y v o l . 3 i s s u e 6 - 2 0 0 9 254
P R A C T I C E G U I D E L I N E SFigure 3. Cross-sections of the TME resection specimen shown in Figure 1 (upper left is proximal, lower right is distal); qualityof mesorectal excision: smooth, regular.Important to note is that both the specimen as awhole (fresh) and the transverse slides (after fixation)should be examined in order to allow adequateevaluation of the mesorectal excision (Figure 3).Digital imaging of the exterior surface prior to cuttingand of whole transverse slides can be performedto document the findings.If the tumor is located close to the distal or proximalsection margins, it is advisable to demonstrate therelationship of the tumor to the margin by takingsections perpendicular to the margin.Node-positive patients may benefit from chemotherapy.It is important to establish the number oftumor-positive lymph nodes with a yield as high aspossible. 6 All lymph nodes should be submitted formicroscopic examination. At least 12 lymph nodesshould be found and embedded according to thecurrent TNM guidelines. 21-23 It may, however, bedifficult to find enough lymph nodes in rectal cancerspecimens, especially after preoperative radiochemotherapy.24,25 However, a high motivation tofind as many nodes as possible must be maintained,since several studies support the concept that themore nodes are examined, the more accurate is thestaging. 6 When less than 7 lymph nodes have beenanalysed, the proportion of cancers with lymphnode involvement is underestimated. 26 Determinationof the lymph node ratio in node-positive coloncancer may be an alternative. 27 There is insufficientscientific evidence to recommend micro-dissectiontechniques or fat clearance to increase the numberof harvested lymph nodes. 21 Furthermore, associatedlesions such as polyps and IBD also need tobe sampled. 21Histological examinationThe histological type of the tumor according to theWHO classification is reported and the tumor isgraded. 28 Different grading systems are used in theliterature. 28 Either a 4 or a 2-tiered descriptive systemcan be used. The 4-tiered system divides thetumors into well, moderate, or poorly differentiatedand undifferentiated tumors. The 2-tiered descriptivesystem reports tumors as either high grade(poorly and undifferentiated tumors) or low grade(well and moderately differentiated tumors). In the2-tiered descriptive system, the high grade correspondsto less than 50% of glandular structures ofthe surface analysed. Signetring cell colorectal carcinomas(composed for more than 50% of signetringcells) and mucinous colorectal adenocarcinomas(more than 50% of the lesion composed ofpools of extracellular mucin-containing malignantepithelium as acinar structures, strips of cells, orsingle cells) are by definition poorly differentiated,while medullary carcinoma of the colon byconvention is considered as undifferentiated carcinoma.28 For accurate grading of colorectal adenocarcinomassuperficial and deep parts of the tumormust be included. 19The depth of tumor invasion, the number of lymphnodes involved and metastatic disease must be reported.21 It is recommended to include the pTNMclassification system, which is used in many internationaltrials (Table 2). The depth of invasion isdescribed in relation to the anatomical structures,i.e. mucosa, submucosa, muscularis propria, mesorectaltissue, and serosa. The number of positivelymph nodes as well as the total number of exam-255v o l . 3 i s s u e 6 - 2 0 0 9B E L G I A N J O U R N A L O F M E D I C A L O N C O L O G Y
Table 2. Pathological TNM classification according to the 5 th edition of TNM - pTNM5.TTXT0TisT1T2T3T4NNXN0N1N2MMXM0M1Primary tumorprimary tumor cannot be assessedno evidence of primary tumorcarcinoma in situ: intraepithelial or invasion of lamina propriatumor invades submucosatumor invades muscularis propriatumor invades through muscularis propria into subserosa or into non-peritonealized periodicor rectal tissuetumor directly invades other organs or structures and/or perforates visceral peritoneumRegional lymph nodesregional lymph nodes cannot be assessedno regional lymph node metastasismetastasis in 1 to 3 regional lymph nodesmetastasis in 4 or more regional lymph nodesDistant metastasesdistant metastasis cannot be assessedno distant metastasisdistant metastasisined lymph nodes must be included. Data are insufficientto recommend the routine use of tissuelevels or special/ancillary techniques. 21 Importantto know is that many involved lymph nodes aresmall, sometimes only a few millimeters in size. 29This can explain the poor correlation with predictionof involved lymph nodes preoperatively byMRI. 30 If the pathologists are using the 6 th editionof TNM, his correlation may even be worse, owingto the classification of all round extramural tumordeposits as completely involved lymph nodes withoutresidual lymphoid tissue. 23 Extramural tumordeposits with an irregular contour are consideredas vascular invasion. In the 5 th edition of TNM,extramural deposits that are not obviously withinlymph nodes are regarded as discontinuous extensionsof the main tumor if they measure 3 mm in diameter. 22 Whilst the evidence for thisdefinition is weak, it does at least have the advantageof being quantitative and, therefore, reproducibleand it may increase pathologist/radiologistagreement. 30 The UK and much of Scandinaviarefused to move to TNM6 as the evidence base isinadequate for the classification of lymph node andvenous invasion, and in addition, the interobservervariability is poor. 30 It has also been advocated bythe PROCARE working group to stick to the 3 mmrule of the TNM5 classification. 2The distance to the circumferential regression margin(CRM) must be measured. A positive CRM isdefined as tumor extension (either continuous ordiscontinuous) or the presence of a positive lymphnode
P R A C T I C E G U I D E L I N E SFigure 4. Slide of a large-area (giant) block, allowing tomeasure the distance of the tumor to the CRM (the resectionmargin is painted with india ink).used to indicate the presence of vascular or lymphaticinvasion. 22Distant metastasis is reported as M1 if confirmedat histological examination. Non-regional lymphnodes are classified as metastases and should be describedseparately. A positive cytological peritonealfluid is also classified as M1. 22Neoadjuvant radiochemotherapy changesThe pathologist should be informed about preoperativetreatment, as in case of neoadjuvant radiochemotherapy(ypTNM) it is advised to estimate tumorregression by means of a semiquantitative gradingsystem, e.g. the Dworak regression grade (Table 3),where regression of the primary tumor is semiquantitativelydetermined by the amount of viable tumorversus the amount of fibrosis, ranging from no evidenceof any treatment effect to a complete responsewith no viable tumor identified. 20 Regression gradingis important for prognosis with a complete responsehaving a better outcome than microscopic diseaseand the latter doing better than moderate, mild, orno regression. 20,30,32,33 Before concluding that there iscomplete response with no viable tumor identified,embedding of the whole suspicious area and the applicationof step sectioning is suggested. 20 To combinerigorous dissection with practicality, it is recommendedthat 5 initial blocks are taken from the siteof the tumor. If no tumor is present, the completesuspicious area should be embedded. If there is stillno tumor, then 3 levels should be cut through eachblock. If finally there is still no tumor found, then thepatient is reported as having a complete response. 34Pathological reporting of rectal cancer resectionspecimensUse of pathology report forms ensures the completenessand consistency of data reporting. This is notonly important for determination of individual patientprognosis and further treatment, but also forassessment of quality of rectal surgery, and the overallmanagement of the disease. Two pathological reportforms are proposed by the <strong>Belgian</strong> PROCAREworking group, one for PME, TME, or APR, anda second form for local (transanal) resection. Thelast updated version of the checklists can be downloadedfrom www.kankerregister.be (menu: procare/working) or www.registreducancer.be (menu: procare/working).The protocol for local resection specimensincludes the pathological subclassificationinto 3 levels of the depth of invasion in superficial(mucosal or submucosal) cancer (Table 4).ConclusionsTotal mesorectal excision (TME) became thestandard surgical treatment for rectal cancer, as itgreatly reduces local recurrences. 1,3 TME and a multidisciplinaryoncologic team approach have led tosignificant improvements in outcome of rectal cancertreatment. 1 Pathologists play a key role in thisprocess. Proper pathological assessment of the TMEspecimen provides important prognostic informationfor the oncologist and identifies patients thatrequire further therapy. 6,15TME resection specimens require a special pathologicalwork-up, as pathologists not only have to determinethe pathological stage of rectal cancer, butin addition they have to assess the completeness oftumor resection and the quality of the mesorectalexcision. 5,6 For this purpose it is important that theresection specimen is delivered unopened to the pathologist.5,6,8 Assessment of the quality of mesorectalexcision must be based on a macroscopic observationof the external surface as well as evaluation ofcross-sectional slides. 5,6 Careful macroscopic as wellas microscopic assessment of the distance of the tumorto the circumferential resection margin (CRM)is of high importance, as this is the most significantpredictor of local recurrence. 6,8-10 In patients witha negative CRM, incomplete mesorectal resectionleads to a higher recurrence rate and lower survival. 5For an adequate benefit of a multidisciplinary oncologicteam approach, it is necessary that all membersof the different medical disciplines of the teamhave sufficient background knowledge of imaging,257v o l . 3 i s s u e 6 - 2 0 0 9B E L G I A N J O U R N A L O F M E D I C A L O N C O L O G Y
Table 3. Dworak regression grade. 20Grade 0 no regressionGrade 1 dominant tumor mass with obvious fibrosis and/or vasculopathyGrade 2 dominantly fibrotic changes with few tumor cells or groups (easy to find)Grade 3 very few (difficult to find microscopically) tumor cells in fibrotic tissue with or without mucous substanceGrade 4 no tumor cells, only fibrotic mass (total regression or response)Table 4. Pathological subclassification of the extent of invasion in superficial cancer.pTis - Primary tumor: invasion of lamina propriam1 superficial third of the mucosam2 middle third of the mucosam3 deepest third of the mucosapT1 - Primary tumor: invasion of submucosasm1 superficial third of the submucosa or invasion depth of less than 0.5 mmsm2 middle third of the submucosa or invasion depth of between 0.5 and 1 mmsm3 deepest third of the submucosa or invasion depth of more than 1 mmpathology, treatment modalities, and prognosticfactors of this disease. In this context, visiting thepathologist in the cut-up room, assisting in theevaluation of the circumferential resection margin,and studying pathological cross-sections can be useful,especially for both the training surgeon and theradiologist. Also digital imaging of the exterior surfaceprior to cutting and of whole transverse slideswill provide feedback to other medical disciplinesof the team.Careful analysis of the rectal cancer resection specimenwith grading and staging of the tumor needto be performed. 21 In particular, a high motivationto find as many lymph nodes as possible must bemaintained, as node-positive patients may benefitfrom chemotherapy. Also, several studies supportthe concept that the more nodes are examined, themore accurate is the staging. 6 It is also advised toreport the degree of tumor regression after neoadjuvantradiochemotherapy. 20,30,32,33 For regressiongrading to mean anything, it is however necessaryto standardize the assessment. Before concludingthat there is complete response with no viable tumoridentified, embedding of the whole suspicious areaand cutting of 3 levels through each tissue block issuggested. 20,34Use of pathology report forms for reporting rectumcancer resection specimens is highly recommended,as it ensures the completeness and consistency ofdata reporting.The next challenge now is the search for immunohistochemicalor molecular markers, that will identifypatients who respond favourably to preoperativetreatment to shrink or destroy the tumor preoperativelyand further increase the percentage of curativesurgery.References1. Quirke P. Training and quality assurance for rectal cancer:20 years of data is enough. Lancet 2003;4:695-701.2. PROCARE: multidisciplinary <strong>Belgian</strong> PROject on CAncer ofthe Rectum. Multidisciplinary guidelines for the treatment ofrectal cancer can be downloaded from www.kankerregister.be(menu: procare) or www.registreducancer.be (menu: procare).3. Heald RJ, Husband EM, Ryall RD. The mesorectum in rectalcancer surgery-the clue to pelvic recurrence? Br J Surg1982;69:613-6.4. Law WL, Chu KW. Anterior resection for rectal cancer withmesorectal excision. A prospective evaluation of 622 patients.Ann Surg 2004;240:260-8.5. Nagtegaal ID, Van de Velde CJ, Van der Worp E, Kapiteijn E,Quirke P, Van Krieken JH, et al. Macroscopic evaluation ofrectal cancer resection specimen: clinical significance of thepathologist in quality control. J Clin Oncol 2002;20:1729-34.6. Maugham NJ, Quirke P. Modern management of colorectalcancer - a pathologist's view. Scand J Surg 2003;92:11-9.7. Parfitt JR, Driman DK. The total mesrorectal excision specimenfor rectal cancer. A review of its pathological assessment.J Clin Pathol 2007;60:849-55.B E L G I A N J O U R N A L O F M E D I C A L O N C O L O G Y v o l . 3 i s s u e 6 - 2 0 0 9 258
P R A C T I C E G U I D E L I N E SKey messages for clinical practice1. A multidisciplinary team approach significantly improves the outcome of rectal cancer patients.The pathologist has a crucial role in this process, by assessment of the quality of themesorectal excision and the completeness of tumor resection.2. The proximity of the tumor to the circumferential resection margin (CRM) is the most importantfactor for predicting the risk of local recurrence in rectal cancer patients. Tumor involvement ofthe CRM strongly correlates with local recurrence, distant metastasis and poor survival.3. Macroscopic evaluation of the completeness of mesorectal excision has additional value in patientswithout CRM involvement. Incomplete mesorectal resection in patients with a negativeCRM leads to a higher recurrence rate and lower survival.4. The number of tumor-positive lymph nodes should be established with a yield as high as possible.Several studies support the concept that the more nodes are examined, the more accurateis the staging.5. Assessment of tumor regression post neoadjuvant treatment needs standardization. Beforeconcluding that there is complete response with no viable tumor identified, embedding of thewhole suspicious area and cutting of 3 levels through each tissue block is suggested.8. Quirke P, Durdey P, Dixon MF, Williams NS. Local recurrenceof rectal adenocarcinoma due to inadequate surgical resection.Histopathological study of lateral tumor spread and surgicalexcision. Lancet 1986;2:996-9.9. Adam IJ, Mohamdee MO, Martin IG, Scott N, Finan PJ, JohnstonD, et al. Role of circumferential margin involvement inthe local recurrence of rectal cancer. Lancet 1994;344:707-11.10. Wibe A, Rendedal PR, Svensson E, Norstein J, Eide TJ, MyrvoldHE, et al. Prognostic significance of the circumferentialresection margin following total mesorectal excision for rectalcancer. Br J Surg 2002;89:327-34.11. Nagtegaal ID, Marijnen CA, Kranenbarg EK, Van de VeldeCJ, Van Krieken JH, for the pathology review committee andthe cooperative clinical investigators. Circumferential margininvolvement is still an important predictor of local recurrencein rectal carcinoma: not one millimetre but two millimetres isthe limit. Am J Surg Pathol 2002;26:350-7.12. Birbeck KF, Macklin CP, Tiffin NJ, Parsons W, Dixon MF,Mapstone NP, et al. Rates of circumferential resection margininvolvement vary between surgeons and predict outcomes inrectal cancer surgery. Ann Surg 2002;235:449-57.13. Marr R, Birbeck K, Garvican J, Macklin CP, Tiffin NJ, ParsonsWJ, et al. The modern abdominoperineal excision. The next challengeafter total mesorectal excision. Ann Surg 2005;242:74-82.14. Nagtegaal ID, Van de Velde CJ, Marijnen CA, Van KriekenJH, Quirke P. Low rectal cancer: a call for a change of approachin abdominoperineal resection. J Clin Oncol 2005;23:9257-64.15. Nagtegaal ID, Van Krieken JH. The role of pathologists inthe quality control of diagnosis and treatment of rectal cancer-anoverview. Eur J <strong>Cancer</strong> 2002;38:964-72.16. Torkzad MR, Blomqvist L. The mesorectum: morphometricassessment with magnetic resonance imaging. Eur Radiol2005;15:1184-91.17. Quirke P, Dixon MF. The prediction of local recurrence inrectal adenocarcinoma by histopathological examination. IntJ Colorect Dis 1988;3:127-31.18. Williams N, Dixon M, Johnston D. Reappraisal of the 5 centimeterrule of distal excision for carcinoma of the rectum: astudy of distal intramural spread and patient' survival. Br JSurg 1983;70:150-4.19. Halvorsen TB. Tissue sampling and histological grading incolorectal cancer. Are routine sections representative? AP-MIS 1989;97:261-6.20. Dworak O, Keilholz L, Hoffmann A. Pathological featuresof rectal cancer after preoperative radiochemotherapy. Int JColorect Dis 1997;12:19-23.21. Compton CC; Updated protocol for the examination ofspecimens from patients with carcinomas of the colon andrectum, excluding carcinoid tumors, lymphomas, sarcomas,and tumors of the vermiform appendix. A basis for checklists.Arch Pathol Lab Med 2000;124:1016-25.22. TNM classification of malignant tumors. 5th ed. NewYork: Wiley; 1997.23. TNM classification of malignant tumors. 6th ed. NewYork: Wiley; 2002.24. Marijnen CA, Nagtegaal ID, Kranenbarg EK, Hermans J,Van de Velde CJ, Leer JW, et al. No downstaging after shorttermpreoperative radiotherapy in rectal cancer patients.J Clin Oncol 2001;19:1976-84.25. Rullier A, Laurent C, Capdepont M, Vendrely V, Bellean-259v o l . 3 i s s u e 6 - 2 0 0 9B E L G I A N J O U R N A L O F M E D I C A L O N C O L O G Y