Community Score Card Process in Gambia: Brochure
Community Score Card Process in Gambia: Brochure
Community Score Card Process in Gambia: Brochure
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
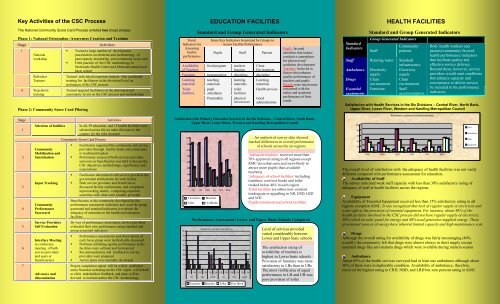
Key Activities of the CSC <strong>Process</strong>The National <strong>Community</strong> <strong>Score</strong> <strong>Card</strong> <strong>Process</strong> entailed two broad phases.Phase 1: National Orientation /Awareness Creation and Tra<strong>in</strong><strong>in</strong>gStage Activities134NationalworkshopRefresherTra<strong>in</strong>ersStep-downtra<strong>in</strong><strong>in</strong>gPhase 2: <strong>Community</strong> <strong>Score</strong> <strong>Card</strong> Pilot<strong>in</strong>g• Tra<strong>in</strong>ed a large number of developmentpractitioners on elements and methodology ofparticipatory monitor<strong>in</strong>g and community score card• Field practice of the CSC methodology <strong>in</strong>Serekunda Health Center and Mohammendan lowerbasic schoolTra<strong>in</strong>ed <strong>in</strong>dividuals/corporate tra<strong>in</strong>ers who conductedtra<strong>in</strong><strong>in</strong>g for facilitators at the divisional level ontechniques of the CSC processTra<strong>in</strong>ed targeted facilitators at the divisional andcommunity levels on the CSC process and methodologyStage Activities1234567Selection of facilities<strong>Community</strong>Mobilization andSensitizationInput Track<strong>in</strong>g<strong>Community</strong>Performance<strong>Score</strong>cardService ProvidersSelf EvaluationInterface Meet<strong>in</strong>g(a conferencemeet<strong>in</strong>g of bothservice providersand users orbeneficiaries)Advocacy anddissem<strong>in</strong>ationIn all, 59 education and 15 health facilities wereselected across the six ma<strong>in</strong> divisions <strong>in</strong> thecountry for the pilot program<strong>Community</strong> <strong>Score</strong> <strong>Card</strong> <strong>Process</strong>• Facilitators organized the community and serviceproviders through facility heads and communityor traditional leaders• Prelim<strong>in</strong>ary session of both services providersand users or beneficiaries was held to discuss theCSC objectives, methodology, significance andexpectations• Facilitators determ<strong>in</strong>ed with service providers thegovernment entitlements for each facility• Both service providers and beneficiariesdiscussed facility entitlements, and completed<strong>in</strong>put track<strong>in</strong>g matrix –compar<strong>in</strong>g expectedamenities with what were actually providedBeneficiaries or the community developed facilityperformance assessment <strong>in</strong>dicators and used the groupgenerated and standard <strong>in</strong>dicators to evaluate theadequacy of amenities <strong>in</strong> the health and educationfacilitiesBy way of performance assessment, service providersevaluated their own performance us<strong>in</strong>g standard andgroup generated <strong>in</strong>dicators• Performance assessments and observations ofeach focus group were methodically discussed• Problems <strong>in</strong>hibit<strong>in</strong>g quality performance <strong>in</strong> thefacilities were collated and harmonized• Recommendations and feedback to serviceproviders were proposed• Action plans were mutually developedProject completion report will be widely publishedand a National workshop on the CSC report will beheldto elicit stakeholders feedback, and plans will bedevised to <strong>in</strong>stitutionalize the CSC methodologyStand.Indicators forAssess<strong>in</strong>gfacilityperformanceAvailabilityof TeachersEDUCATION FACILITIESStandard and Group Generated IndicatorsSome Key Indicators Generated by Groups toAssess Facility PerformancePupils Staff Parentsfood programteachershous<strong>in</strong>gCleanEnvironmentFurniture transportation discipl<strong>in</strong>e discipl<strong>in</strong>eLearn<strong>in</strong>gmaterialsToiletfacilitiesteach<strong>in</strong>gmaterialspupilattendancePunctualitylearn<strong>in</strong>gmaterialstoiletfacilitiesphysical<strong>in</strong>frastructureLearn<strong>in</strong>gmaterialsHealth servicesGoodadm<strong>in</strong>istrationPupils favoredamenities that <strong>in</strong>duceconducive atmospherefor physical andacademic developmentTeachers believed <strong>in</strong>factors that enhancequality performance ofteachers and pupilsParents were much moreconcerned with thesafety and academicperformance of theirwardsSatisfaction with Primary Education Services <strong>in</strong> the Six Divisions – Central River, North Bank,Upper River, Lower River, Western and Kanif<strong>in</strong>g Metropolitan Council8070605040302010080706050403020100CR NB URD LR WD KMCTearchers BenchesToiletTextBooksPerformance Assessment: Lower and Upper Basic Schools ComparedSatisfaction with Education ServicesLB UB LB UB LB UB LB UB LB UB LB UBCR NB URD LR WD KMCTeachers Benches Toilet Text BookAn analysis of survey data showedmarked differences <strong>in</strong> overall performanceof schools across the six regions‘Adequate teachers’ received more than70% approval rat<strong>in</strong>g <strong>in</strong> all regions exceptKMC (an urban area and more likely toattract more pupils than availableteachers)‘Adequacy of school facilities’ <strong>in</strong>clud<strong>in</strong>gfurniture, core text books and toiletranked below 40% <strong>in</strong> each regionToilet facilities are either non- existent<strong>in</strong>adequate or appall<strong>in</strong>g <strong>in</strong> NB, URD, LRDand WDPupils enrolment and school facilitiesi ll i KMCLevel of services providedvaried considerably betweenLower and Upper basic schoolsThe satisfaction rat<strong>in</strong>g ofavailability of teachers ishighest <strong>in</strong> Lower basic schoolsProvision of furniture was moresatisfactory <strong>in</strong> LBs than <strong>in</strong> UBsThe most visible area of equalperformance <strong>in</strong> LB and UB waspoor provision of toiletStandardIndicatorsHEALTH FACILITIESStandard and Group Generated IndicatorsSatisfaction with Health Services <strong>in</strong> the Six Divisions – Central River, North Bank,Upper River, Lower River, Western and Kanif<strong>in</strong>g Metropolitan Council100806040200Group Generated IndicatorsStaff<strong>Community</strong>/patientsStaff Runn<strong>in</strong>g water Standard<strong>in</strong>frastructureAmbulance ElectricitysupplyElectricitysupplyDrugs CleanCleanenvironment environmentEssentialequipmentsFurniture StaffaccommodationPerformance Assessment (standard <strong>in</strong>dicators)CRD NBD URD LRD WD KMCBoth health workers andpatients/community favoredhealth performance <strong>in</strong>dicatorsthat facilitate quality andeffective service delivery.Beyond these, however, serviceproviders would want conditionsthat enhance capacity andconvenience to deliver servicebe <strong>in</strong>cluded <strong>in</strong> the performance<strong>in</strong>dicators.StaffAmbulancedrugsEquipmentThe overall level of satisfaction with the adequacy of health facilities was not vastlydifferent compared with performance assessment for education.Availability of StaffThe survey <strong>in</strong>dicated weak staff capacity with less than 30% satisfactory rat<strong>in</strong>g ofadequacy of staff at health facilities across the regions.EquipmentAvailability of Essential Equipment received less than 15% satisfactory rat<strong>in</strong>g <strong>in</strong> allregions exception KMC. It was recognized that lack of regular supply of electricity andwater affects the provision of essential equipment. For <strong>in</strong>stance, about 40% of thehealth facilities <strong>in</strong>volved <strong>in</strong> the CSC process did not have regular supply of electricity,20% relied on solar panel for energy and 40% used generator-supplied energy. Theseprovisional sources of energy have <strong>in</strong>herent limited capacity and high ma<strong>in</strong>tenance cost.DrugsAlthough the overall rat<strong>in</strong>g for availability of drugs was fairly encourag<strong>in</strong>g (40%overall), the community felt that drugs were almost always <strong>in</strong> short supply exceptessential drugs like anti-malaria drugs which were available dur<strong>in</strong>g malaria seasonAmbulanceAbout 69% of the health services surveyed had at least one ambulance although about30% of them were <strong>in</strong> deplorable condition. Availability of ambulance, therefore,received the highest rat<strong>in</strong>g <strong>in</strong> CRD, NBD, and LRD but zero percent rat<strong>in</strong>g <strong>in</strong> KMC.
Recommendations from Service Providersand the <strong>Community</strong> for Improv<strong>in</strong>g Performance <strong>in</strong>Health FacilitiesEstablish a health committee represent<strong>in</strong>g the community and healthstaff to develop strategies and rules for enhanc<strong>in</strong>g efficient and effectivehealth services delivery <strong>in</strong> the communityHealth Committee should ensure government meets entitlementpackages <strong>in</strong>clud<strong>in</strong>g adequate supply of drugs, water, electricity,equipment, tra<strong>in</strong><strong>in</strong>g and supply of health workersHealth Committee should champion an agenda for promot<strong>in</strong>g cleanl<strong>in</strong>essand clean habit <strong>in</strong> and around health centersEstablish health supplemental fund<strong>in</strong>g program to ease reliance ongovernment support (<strong>in</strong>adequate and unpredictable government flowshave affected the quality of services provided <strong>in</strong> the hospital). In a fewcommunities, <strong>in</strong>dividuals took the <strong>in</strong>itiative and made voluntarycontributions to help repair broken facilities <strong>in</strong> the cl<strong>in</strong>ic.General Observations on the <strong>Community</strong> <strong>Score</strong> <strong>Card</strong><strong>Process</strong> <strong>in</strong> <strong>Gambia</strong>There was strong support for the CSC methodologyand an expressed <strong>in</strong>dication for the tool to benurtured for foster<strong>in</strong>g community empowerment andparticipation at the local levelThe CSC process succeeded <strong>in</strong> extract<strong>in</strong>g communitygrievances about the quality and adequacy of healthand education services at the community levelThe process created a great deal of awareness on therelevance of CRC and, empowered the community toappreciate the implementation of the communityscore card. Approximately 3,500 stakeholdersparticipated <strong>in</strong> the process at the communitylevel alone <strong>in</strong>clud<strong>in</strong>g teachers, pupils, healthworkers and the community.The pilot project revealed that both service providersand the community were adequately <strong>in</strong>formed aboutthe nature of and scope of their education and healthneedsLessons Learned and Correspond<strong>in</strong>g Recommendations<strong>Community</strong> EmpowermentPerhaps the most important lesson learned <strong>in</strong>the implementation of the CSC wascommunity empowerment through: <strong>in</strong>terfacemeet<strong>in</strong>g between service users and providersfor immediate feedback and mutuallydeveloped action plans.<strong>Community</strong> ParticipationThe CSC <strong>Process</strong> enabled maximumparticipation of a wide range of stakeholdersfrom various towns and villages. More than55 development practitioners took part <strong>in</strong> thenational refresher tra<strong>in</strong><strong>in</strong>g and about 3,500participants were <strong>in</strong>volved <strong>in</strong> the CSCprocess at the community level.Self-help spirit:The CSC process revived self-help spiritamong communities expressed largelythrough <strong>in</strong>stant <strong>in</strong>dividual voluntary f<strong>in</strong>ancialcontributions, and the emphasis oncommunity roles <strong>in</strong> address<strong>in</strong>g majority ofthe problems confront<strong>in</strong>g facilities <strong>in</strong> thecommunity.Awareness Creation<strong>Community</strong> members were enlightenedabout expected quantity and quality ofselected services <strong>in</strong> the their communitiesThe Scope of the CSC <strong>Process</strong>The CSC project was ambitious <strong>in</strong> terms ofcoverage. Though a pilot program, itexpanded across the entire country <strong>in</strong>volv<strong>in</strong>g59 education facilities and 15 health services.The CSC FocusPerformance <strong>in</strong>dicators were focused moreon measur<strong>in</strong>g quantity and less on qualityand output of the facilitiesData Management and AnalysisData management and analysis posedchallenge for the CSC result<strong>in</strong>g <strong>in</strong> somedelays <strong>in</strong> produc<strong>in</strong>g survey results.This not withstand<strong>in</strong>g, an evaluation ofparticipants perceptions on the entireCSC process, us<strong>in</strong>g post programevaluation questionnaire would haveprovided a fairly elaborate <strong>in</strong>formationon the general acceptability of themethodologyAn extensive community focusedprogram of this k<strong>in</strong>d requires adequatetime for consultation and sensitization.Participants <strong>in</strong>dicated that extendedtime for sensitization would have beenappropriate.Importance of <strong>in</strong>formation shar<strong>in</strong>g,dissem<strong>in</strong>ation of project outcomes,advocacy efforts and plann<strong>in</strong>g for howto <strong>in</strong>stitutionalize CSC and socialaccountability processes at communitylevel would further resonate withcommunity driven <strong>in</strong>itiatives <strong>in</strong>address<strong>in</strong>g development problemsInstitutionalization of the of the CSCprocess would be critical <strong>in</strong> open<strong>in</strong>gopportunities for community membersto express grievances about the qualityof services providedThough nation wide coverage waslaudable, the program’s scope ought tobe considered <strong>in</strong> the context ofavailable resources and capacity. Forexample, the scale of the exercisepresented challenges which could berevisited, <strong>in</strong>clud<strong>in</strong>g balanc<strong>in</strong>g a focuson the use of the CSC as a datamanagement tool versus anempowerment processMeasur<strong>in</strong>g adequacy of services isimportant, but a CSC process that isdesigned to measure both quality andadequacy of services would fairlyreflect community preferences <strong>in</strong>identify<strong>in</strong>g performance targetsMak<strong>in</strong>g adequate provision for capacityand resource needs for datamanagement and analysis would greatlyenhance the CSC process. Qualitytra<strong>in</strong><strong>in</strong>g at the beg<strong>in</strong>n<strong>in</strong>g of exerciseand close supervision throughout theCSC exercise ought to be considered<strong>Community</strong> <strong>Score</strong> <strong>Card</strong><strong>in</strong><strong>Gambia</strong>Monitor<strong>in</strong>g and evaluat<strong>in</strong>g the effectiveness of poverty strategies arecritical elements <strong>in</strong> the efforts to achieve susta<strong>in</strong>able and equitabledevelopment. Under its Poverty Reduction Strategic Papers (PRSP),<strong>Gambia</strong> outl<strong>in</strong>ed its commitment to promot<strong>in</strong>g accountability,transparency and effectiveness through broad-based communityparticipation <strong>in</strong> monitor<strong>in</strong>g and evaluation. However, there are criticalchallenges that need to be addressed <strong>in</strong> order to pursue these goals moreresolutely and consistently – <strong>in</strong>clud<strong>in</strong>g the need to strengthen thecapacity of stakeholders and enhance citizen participation.In l<strong>in</strong>e with its broad development objectives, the government of <strong>Gambia</strong><strong>in</strong> collaboration with the Participation and Civic Engagement group ofSocial Development Department of the World Bank, developed theAccountability and Participatory Monitor<strong>in</strong>g and EvaluationProgram which seeks to broaden citizens’ capacity, create opportunityfor citizens’ participation and feedback on the quality, adequacy andefficiency of key services largely through the <strong>Community</strong> <strong>Score</strong> <strong>Card</strong>(CSC) process. The CSC is a community based monitor<strong>in</strong>g tool that isa hybrid of the techniques of social audit, community monitor<strong>in</strong>g andcitizen report cards. It has a strong focus on empowerment andaccountability as it <strong>in</strong>cludes an <strong>in</strong>terface meet<strong>in</strong>g between serviceproviders and the community that allows for immediate feedback.The CSC process <strong>in</strong> <strong>Gambia</strong>, though a pilot program, <strong>in</strong>volved 59 publicschools and 15 health services. A large spectrum of stakeholdersparticipated <strong>in</strong> the process- there were approximately 3,500 people from650 towns and villages at the community level <strong>in</strong>clud<strong>in</strong>g teachers,pupils, health workers and community members.-------------------------------February 2005-----------------------------------For more <strong>in</strong>formation on <strong>Community</strong> <strong>Score</strong> <strong>Card</strong> or Participation and Monitor<strong>in</strong>gtools contact:Ser<strong>in</strong>g Falu NjieCoord<strong>in</strong>ator,Strategy for Poverty Alleviation Coord<strong>in</strong>ation Office (SPACO)15/16 Mar<strong>in</strong>a Parade Banjul, <strong>Gambia</strong>Tel: 220 422 9761 Email: falugalas@hotmail.com orVisit http://www.worldbank.org/participation