Disability Benefit Claim Employer Statement - nbcrfli.org.za
Disability Benefit Claim Employer Statement - nbcrfli.org.za
Disability Benefit Claim Employer Statement - nbcrfli.org.za

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
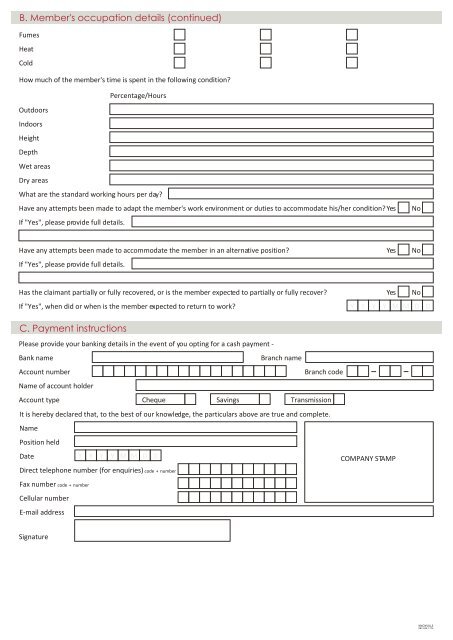
B. Member's occupation details (continued)FumesHeatColdHow much of the member's time is spent in the following condition?Percentage/HoursOutdoorsIndoorsHeightDepthWet areasDry areasWhat are the standard working hours per day?Have any attempts been made to adapt the member's work environment or duties to accommodate his/her condition? YesIf "Yes", please provide full details.NoHave any attempts been made to accommodate the member in an alternative position?If "Yes", please provide full details.YesNoHas the claimant partially or fully recovered, or is the member expected to partially or fully recover?If "Yes", when did or when is the member expected to return to work?YesNoY Y Y Y M M D DC. Payment instructionsPlease provide your banking details in the event of you opting for a cash payment -Bank nameBranch nameAccount numberBranch codeName of account holderAccount typeCheque Savings TransmissionIt is hereby declared that, to the best of our knowledge, the particulars above are true and complete.NamePosition heldDateY Y Y Y M M D DCOMPANY STAMPDirect telephone number (for enquiries) code + numberFax number code + numberCellular numberE-mail addressSignatureKNOXVILLE083 636 1774