sample letter to households summer food service program
sample letter to households summer food service program
sample letter to households summer food service program

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
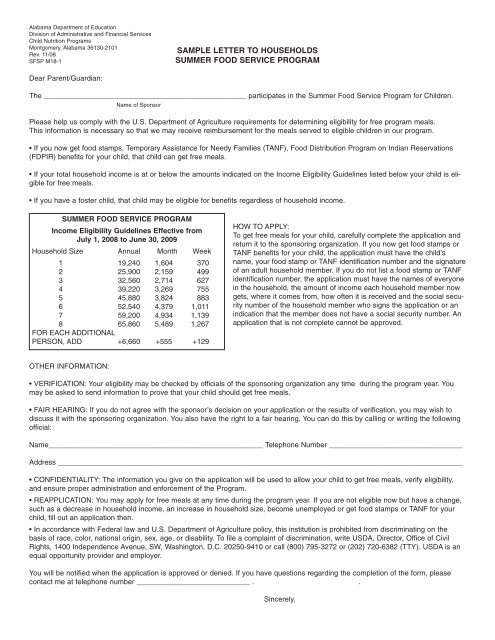
Alabama Department of EducationDivision of Administrative and Financial ServicesChild Nutrition ProgramsMontgomery, Alabama 36130-2101Rev. 11/08SFSP M18-1SAMPLE LETTER TO HOUSEHOLDSSUMMER FOOD SERVICE PROGRAMDear Parent/Guardian:The __________________________________________________ participates in the Summer Food Service Program for Children.Name of SponsorPlease help us comply with the U.S. Department of Agriculture requirements for determining eligibility for free <strong>program</strong> meals.This information is necessary so that we may receive reimbursement for the meals served <strong>to</strong> eligible children in our <strong>program</strong>.• If you now get <strong>food</strong> stamps, Temporary Assistance for Needy Families (TANF), Food Distribution Program on Indian Reservations(FDPIR) benefits for your child, that child can get free meals.• If your <strong>to</strong>tal household income is at or below the amounts indicated on the Income Eligibility Guidelines listed below your child is eligiblefor free meals.• If you have a foster child, that child may be eligible for benefits regardless of household income.SUMMER FOOD SERVICE PROGRAMIncome Eligibility Guidelines Effective fromJuly 1, 2008 <strong>to</strong> June 30, 2009Household Size Annual Month Week1 19,240 1,604 3702 25,900 2,159 4993 32,560 2,714 6274 39,220 3,269 7555 45,880 3,824 8836 52,540 4,379 1,0117 59,200 4,934 1,1398 65,860 5,489 1,267FOR EACH ADDITIONALPERSON, ADD +6,660 +555 +129HOW TO APPLY:To get free meals for your child, carefully complete the application andreturn it <strong>to</strong> the sponsoring organization. If you now get <strong>food</strong> stamps orTANF benefits for your child, the application must have the child’sname, your <strong>food</strong> stamp or TANF identification number and the signatureof an adult household member. If you do not list a <strong>food</strong> stamp or TANFidentification number, the application must have the names of everyonein the household, the amount of income each household member nowgets, where it comes from, how often it is received and the social securitynumber of the household member who signs the application or anindication that the member does not have a social security number. Anapplication that is not complete cannot be approved.OTHER INFORMATION:• VERIFICATION: Your eligibility may be checked by officials of the sponsoring organization any time during the <strong>program</strong> year. Youmay be asked <strong>to</strong> send information <strong>to</strong> prove that your child should get free meals.• FAIR HEARING: If you do not agree with the sponsor’s decision on your application or the results of verification, you may wish <strong>to</strong>discuss it with the sponsoring organization. You also have the right <strong>to</strong> a fair hearing. You can do this by calling or writing the followingofficial:Name_____________________________________________________ Telephone Number _________________________________Address ____________________________________________________________________________________________________• CONFIDENTIALITY: The information you give on the application will be used <strong>to</strong> allow your child <strong>to</strong> get free meals, verify eligibility,and ensure proper administration and enforcement of the Program.• REAPPLICATION: You may apply for free meals at any time during the <strong>program</strong> year. If you are not eligible now but have a change,such as a decrease in household income, an increase in household size, become unemployed or get <strong>food</strong> stamps or TANF for yourchild, fill out an application then.• In accordance with Federal law and U.S. Department of Agriculture policy, this institution is prohibited from discriminating on thebasis of race, color, national origin, sex, age, or disability. To file a complaint of discrimination, write USDA, Direc<strong>to</strong>r, Office of CivilRights, 1400 Independence Avenue, SW, Washing<strong>to</strong>n, D.C. 20250-9410 or call (800) 795-3272 or (202) 720-6382 (TTY). USDA is anequal opportunity provider and employer.You will be notified when the application is approved or denied. If you have questions regarding the completion of the form, pleasecontact me at telephone number ____________________________ . .Sincerely,
HOW TO COMPLETE THE SUMMER FOOD SERVICE PROGRAMMEAL BENEFIT INCOME ELIGIBILITY FORM(For Camps and Closed Enrolled Sites)Please complete the following form using the instructions below.Sign the form and return it <strong>to</strong> ________________________________________________NAME OF SPONSORIf you need help, call _______________________________________________________TELEPHONE NUMBERFollow these instructions, if your household gets FOOD STAMPS, TANF or FDPIR:Part 1: List participant's name and a Food Stamp, TANF or FDPIR case number.Part 2: Skip this part.Part 3: Skip this part.Part 4: Sign the form. A Social Security Number is not necessary.Part 5: Answer this question if you choose <strong>to</strong>.If you are applying on behalf of a FOSTER CHILD, use a separate application for each foster child andfollow these instructions:Part 1: Enter the child's name.Part 2: Enter child’s personal use monthly income. If foster child does not receive personal use income, enter zero.If you have questions, contact ___________________________.Part 3: Skip this part.Part 4: Sign the form. A Social Security Number is not necessary.Part 5: Answer this question if you choose <strong>to</strong>.ALL OTHER HOUSEHOLDS, including WIC <strong>households</strong>, follow these instructions:Part 1: List each participant's name.Part 2: Skip this part.Part 3: Follow these instructions <strong>to</strong> report <strong>to</strong>tal household income from last month.Column A-Name: List the first and last name of each person living in your household, related or not (suchas grandparents, other relatives, or friends who live with you). You must include yourself and all childrenliving with you. Attach another sheet of paper if you need <strong>to</strong>.Column B-Gross income last month and how often it was received. Next <strong>to</strong> each person's name, listeach type of income received last month, and how often it was received.In Box 1, list the gross income each person earned from work. This is not the same as take-home pay.Gross income is the amount earned before taxes and other deductions. The amount should be listedon your pay stub, or your boss can tell you. Next <strong>to</strong> the amount, write how often the person got it (weekly,every other week, twice a month, or monthly.In box 2, list the amount each person got last month from welfare, child support, alimony.In box 3, list Social Security, pensions, and retirement.In box 4, list ALL OTHER INCOME SOURCES including Worker's Compensation, unemployment, strikebenefits, Supplemental Security Income (SSI), Veteran's benefits (VA benefits), disability benefits, regularcontributions from people who do not live in your household. Report net income for self-owned business,farm, or rental income. Next <strong>to</strong> the amount, write how often the person got it. If you are in the MilitaryHousing Privatization Initiative, do not include this housing allowance.Column C-Check if no income: If the person does not have any income, check the box.Part 4: An adult household member must sign the form and list his or her Social Security Number, or mark the boxif he or she doesn't have one.Part 5: Answer this question if you choose <strong>to</strong>.Privacy Act Statement: This explains how we will use the information you give us.Non-discrimination Statement: This explains what <strong>to</strong> do if you believe you have been treated unfairly.Oc<strong>to</strong>ber 2008SFSP Meal Benefit Income Eligibility Form Instructions
Alabama Department of EducationDivision of Administrative and Financial ServicesFood Distribution and Special Nutrition ProgramsMontgomery, Alabama 36130-2101Rev. 11/08SFSP M18-2SUMMER FOOD SERVICE PROGRAMMEAL BENEFIT ELIGIBILITY FORM(For Camps and Closed Enrolled Sites)Page 1 of 2Part 1. Children enrolled in Camp or Closed Enrolled Sites. (Use a separate application for each foster child.)NamesFood Stamp, TANF, FDPIR number, (if any).(First, Middle Initial, Last) Skip <strong>to</strong> Part 4 if you listed a case #.Part 2. Foster ChildIn certain cases, foster children are eligible for free and reduced-price meals regardless of household income. If a foster child liveswith you, check this box ❏ and then list the amount of the child’s personal use monthly income. $__________________________Please contact _______________________________________ at _____________________ if you have questions. Skip <strong>to</strong> Part 4.NAME OF SPONSORPHONE NUMBERPart 3. Total Household Gross Income — You must tell us how much and how often.B. Gross income and how often it was receivedA. Name Example: $100/month $100/twice a month $100/every other week $100/week(List everyone in household, 1. Earnings from work 2. Welfare, child 3. Social Security,including children) before deductions support, alimony pension, retirement 4. All other incomeExample: Jane Smith $200 / weekly $150 / weekly $100 / monthly $ ______ / ______$ ______ / ______ $ ______ / ______ $ ______ / ______ $ ______ / ______$ ______ / ______ $ ______ / ______ $ ______ / ______ $ ______ / ______$ ______ / ______ $ ______ / ______ $ ______ / ______ $ ______ / ______$ ______ / ______ $ ______ / ______ $ ______ / ______ $ ______ / ______$ ______ / ______ $ ______ / ______ $ ______ / ______ $ ______ / ______$ ______ / ______ $ ______ / ______ $ ______ / ______ $ ______ / ______$ ______ / ______ $ ______ / ______ $ ______ / ______ $ ______ / ______Part 4. Signature and Social Security Number (Adult must sign.)An adult household member must sign this form. If Part 3 is completed, the adult signing the form must also list his or her SocialSecurity Number or mark the “I do not have a Social Security Number” box. (See Privacy Act Statement on the back of this page.)I certify that all information on this form is true and that all income is reported. I understand that this information is being given for thereceipt of Federal funds. I understand that SFSP officials may verify the information. I understand that if I purposely give false information,the participant(s) receiving meals may lose the meal benefits, and I may be prosecuted under State of Federal criminal laws._______________________________________________ _________________________________________ ________________SIGN HERE PRINT NAME DATE__________________________________________________________________________________________ ________________ADDRESSPHONE NUMBER____ ____ ____–____ ____–____ ____ ____ ____❏ I do not have a Social Security NumberSOCIAL SECURITY NUMBERPart 5. Participant’s ethnic and racial identities (Optional)Mark one ethnic identify:Mark one or more racial identities:Hispanic or Latino❏ Not Hispanic or Latino Asian ❏ White❏ Black or African American American Indian or Alaska Native❏ Native Hawaiian or Other Pacific IslanderC.Check ifNOIncome❏❏❏❏❏❏❏❏FOR OFFICIAL USE ONLYAnnual Income Conversion: Weekly x 52, Every Two Weeks x 26, Twice A Month x 24, Monthly x 12Total Income: __________________ Per ❏Week, ❏Every 2 Weeks, ❏Twice A Month, ❏Month ❏Year Household Size: _____________Eligibility Determination: ❏ FS/TANF/FDPIR ❏ Eligible ❏ Ineligible Reason for Ineligibility: ❏ Incomplete Application ❏ Income Too High❏ Temporary Approval Time Period: ______________________ (expires after _________ days) Date Withdrawn: ______________________________________________________________DETERMINING OFFICIAL SIGNATURE________________________DATE
SFSP Meal Benefit Eligibility Form — Page 2 of 2SUMMER FOOD SERVICE PROGRAM MEAL BENEFIT ELIGIBILITY FORM(For Camps and Closed Enrolled Sites)Privacy Act Statement: The Richard B. Russell National School Lunch Act requires the information on this application. You do nothave <strong>to</strong> give the information, but if you do not, we cannot approve your child for free or reduced price meals. You must include theSocial Security Number of the adult household member who signs the application. The Social Security Number is not required whenyou apply on behalf of a foster child or you list a Food Stamp, Temporary Assistance for Needy Families (TANF) Program or FoodDistribution Program on Indian Reservations (FDPIR) case number for your child or other FDPIR identifier or when you indicate thatthe adult household member signing the application does not have a Social Security Number. We will use your information <strong>to</strong> determineif your child is eligible for free or reduced price meals, and for administration and enforcement of the Program.___________________________________________________________________________________________________________Non-discrimination Statement: In accordance with Federal law and U.S. Department of Agriculture policy, this institution is prohibitedfrom discriminating on the basis or race, color, national origin, sex, age, or disability. To file a complaint of discrimination, write<strong>to</strong> USDA, Direc<strong>to</strong>r, Office of Civil Rights, 1400 Independence Avenue, SW, Washing<strong>to</strong>n DC 20250-9410 or call (800) 795-3272 or(202) 720-6382 (TTY). USDA is an equal opportunity provider and employer.Income <strong>to</strong> ReportEarnings From WorkWages/salaries/tipsStrike benefitsUnemployment compensationWorkman’s compensationNet income from self-owned business or farmWelfare/Child Support/AlimonyPublic assistance paymentsWelfare paymentsAlimony paymentsChild support paymentsPensions/Retirement/Social SecurityPensionsRetirement incomeSocial SecurityVeteran paymentsSupplemental Security IncomeOther Income/Self-employmentEarnings from second jobDisability benefitsInterest/DividendsCash withdrawn from SavingsIncome from Estates/Trusts/InvestmentsRegular contributions from persons not living in the householdNet Royalties/Annuities/Net Rental incomeAny other income that may be available <strong>to</strong> pay for the child’s mealsSummer Food Service Program IncomeEligibility GuidelinesUSDA’s Income Eligibility Guidelines for reduced price school meals—thebasis of SFSP meal eligibility—are equal <strong>to</strong> 185 percent of the Office ofManagement and Budget’s nonfarm income poverty guidelines. Householdswith income less than or equal <strong>to</strong> these values are eligible for free SummerFood Service Program meals.EFFECTIVE FROM JULY 1, 2008 TO JUNE 30, 2009Household Size Annual Month Week1 19,240 1,604 3702 25,900 2,159 4993 32,560 2,714 6274 39,220 3,269 7555 45,880 3,824 8836 52,540 4,379 1,0117 59,200 4,934 1,1398 65,860 5,489 1,267FOR EACHADDITIONALPERSON, ADD +6,660 +555 +129
Alabama Department of EducationDivision of Administrative and Financial ServicesFood Distribution and Special Nutrition ProgramsMontgomery, Alabama 36130-2101Rev.11/08SFSP M18-3EVALUATION SHEET FOR FREE AND REDUCED-PRICE MEAL APPLICATIONSBased on USDA Income Eligibility GuidelinesEffective July 1, 2008 – June 30, 2009Use the following scale when determining eligibility for free meal benefits in the Summer Food Service Program during FY 2009.Copies of this sheet should be given <strong>to</strong> all personnel who receive and evaluate applications for free and reduced-price meals.You may make as many copies of this sheet as needed.Summer Food Service Program IncomeEligibility GuidelinesUSDA’s Income Eligibility Guidelines for reduced price school meals—thebasis of SFSP meal eligibility—are equal <strong>to</strong> 185 percent of the Office ofManagement and Budget’s nonfarm income poverty guidelines. Householdswith income less than or equal <strong>to</strong> these values are eligible for free SummerFood Service Program meals.EFFECTIVE FROM JULY 1, 2008 TO JUNE 30, 2009Household Size Annual Month Week1 19,240 1,604 3702 25,900 2,159 4993 32,560 2,714 6274 39,220 3,269 7555 45,880 3,824 8836 52,540 4,379 1,0117 59,200 4,934 1,1398 65,860 5,489 1,267FOR EACHADDITIONALPERSON, ADD +6,660 +555 +129NOTE: To convert weekly income figures <strong>to</strong> annual figures, multiply weekly income by 52.To convert twice-monthly income figures <strong>to</strong> annual figures, multiply bi-weekly income by 24.To convert bi-weekly (every 2 weeks) income figures <strong>to</strong> annual figures, multiply income by 26.