Change of Address Form - eMedNY
Change of Address Form - eMedNY
Change of Address Form - eMedNY
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
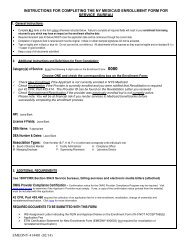
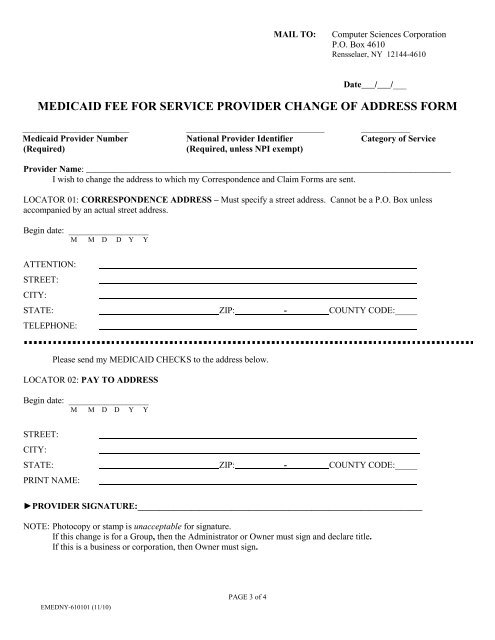
MAIL TO:Computer Sciences CorporationP.O. Box 4610Rensselaer, NY 12144-4610Date___/___/___MEDICAID FEE FOR SERVICE PROVIDER CHANGE OF ADDRESS FORM________________________ _______________________________ ___________Medicaid Provider Number National Provider Identifier Category <strong>of</strong> Service(Required)(Required, unless NPI exempt)Provider Name: __________________________________________________________________________________I wish to change the address to which my Correspondence and Claim <strong>Form</strong>s are sent.LOCATOR 01: CORRESPONDENCE ADDRESS – Must specify a street address. Cannot be a P.O. Box unlessaccompanied by an actual street address.Begin date: __________________M M D D Y YATTENTION:STREET:CITY:STATE: ZIP: -TELEPHONE:COUNTY CODE:_____Please send my MEDICAID CHECKS to the address below.LOCATOR 02: PAY TO ADDRESSBegin date: __________________M M D D Y YSTREET:CITY:STATE: ZIP: -PRINT NAME:COUNTY CODE:_____►PROVIDER SIGNATURE:________________________________________________________________NOTE: Photocopy or stamp is unacceptable for signature.If this change is for a Group, then the Administrator or Owner must sign and declare title.If this is a business or corporation, then Owner must sign.EMEDNY-610101 (11/10)PAGE 3 <strong>of</strong> 4