ADULT HIV / AIDS CONFIDENTIAL CASE REPORT FORM - Epi
ADULT HIV / AIDS CONFIDENTIAL CASE REPORT FORM - Epi
ADULT HIV / AIDS CONFIDENTIAL CASE REPORT FORM - Epi

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
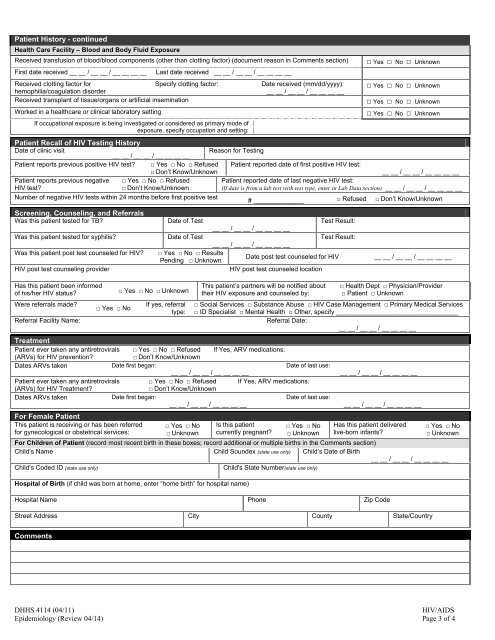
Patient History - continuedHealth Care Facility – Blood and Body Fluid ExposureReceived transfusion of blood/blood components (other than clotting factor) (document reason in Comments section)First date received __ __ / __ __ / __ __ __ __Received clotting factor forSpecify clotting factor:hemophilia/coagulation disorderReceived transplant of tissue/organs or artificial inseminationWorked in a healthcare or clinical laboratory settingLast date received __ __ / __ __ / __ __ __ __If occupational exposure is being investigated or considered as primary mode ofexposure, specify occupation and setting:Date received (mm/dd/yyyy):__ __ / __ __ / __ __ __ __Patient Recall of <strong>HIV</strong> Testing HistoryDate of clinic visit__ __ / __ __ / __ __ __ __Reason for TestingPatient reports previous positive <strong>HIV</strong> test? □ Yes □ No □ Refused□ Don’t Know/UnknownPatient reported date of first positive <strong>HIV</strong> test:Patient reports previous negative<strong>HIV</strong> test?□ Yes □ No □ Refused□ Don’t Know/UnknownNumber of negative <strong>HIV</strong> tests within 24 months before first positive testScreening, Counseling, and ReferralsWas this patient tested for TB?Was this patient tested for syphilis?Was this patient post test counseled for <strong>HIV</strong>?<strong>HIV</strong> post test counseling providerHas this patient been informedof his/her <strong>HIV</strong> status?Were referrals made?Referral Facility Name:□ Yes □ No□ Yes □ No □ Unknown□ Yes □ No □ Unknown□ Yes □ No □ Unknown□ Yes □ No □ Unknown□ Yes □ No □ Unknown__ __ / __ __ / __ __ __ __Patient reported date of last negative <strong>HIV</strong> test:(If date is from a lab test with test type, enter in Lab Data section) __ __ / __ __ / __ __ __ __# ______________ □ Refused □ Don’t Know/UnknownDate of TestTest Result:__ __ / __ __ / __ __ __ __Date of TestTest Result:__ __ / __ __ / __ __ __ __□ Yes □ No □ ResultsDate post test counseled for <strong>HIV</strong>Pending □ Unknown<strong>HIV</strong> post test counseled locationIf yes, referraltype:This patient’s partners will be notified abouttheir <strong>HIV</strong> exposure and counseled by:__ __ / __ __ / __ __ __ __□ Health Dept □ Physician/Provider□ Patient □ Unknown□ Social Services □ Substance Abuse □ <strong>HIV</strong> Case Management □ Primary Medical Services□ ID Specialist □ Mental Health □ Other, specify __________________________________Referral Date:__ __ / __ __ / __ __ __ __TreatmentPatient ever taken any antiretrovirals □ Yes □ No □ Refused If Yes, ARV medications:(ARVs) for <strong>HIV</strong> prevention?□ Don’t Know/UnknownDates ARVs takenDate first began:Date of last use:__ __ / __ __ / __ __ __ __Patient ever taken any antiretrovirals □ Yes □ No □ Refused If Yes, ARV medications:(ARVs) for <strong>HIV</strong> Treatment?□ Don’t Know/UnknownDates ARVs takenDate first began:Date of last use:__ __ / __ __ / __ __ __ __For Female PatientThis patient is receiving or has been referredfor gynecological or obstetrical services:□ Yes □ No□ UnknownIs this patientcurrently pregnant?□ Yes □ No□ Unknown__ __ / __ __ / __ __ __ ____ __ / __ __ / __ __ __ __Has this patient deliveredlive-born infants?□ Yes □ No□ UnknownFor Children of Patient (record most recent birth in these boxes; record additional or multiple births in the Comments section)Child’s Name Child Soundex (state use only) Child’s Date of Birth__ __ / __ __ / __ __ __ __Child’s Coded ID (state use only)Child's State Number(state use only)Hospital of Birth (if child was born at home, enter “home birth” for hospital name)Hospital Name Phone Zip CodeStreet Address City County State/CountryCommentsDHHS 4114 (04/11)<strong>HIV</strong>/<strong>AIDS</strong><strong>Epi</strong>demiology (Review 04/14) Page 3 of 4