Read the full story - TEDx UWollongong
Read the full story - TEDx UWollongong
Read the full story - TEDx UWollongong

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
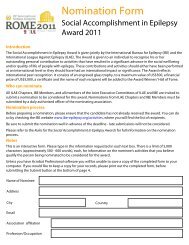
News ReviewGetting ahead ofepilepsyYou’ve no doubt heardabout <strong>the</strong> bionic eye and<strong>the</strong> cochlear implant —some of <strong>the</strong> most famousdevelopments in <strong>the</strong> fast-growingworld of medical bionics.But Professor Mark Cook is quietlyoptimistic that an even biggergroup of patients — <strong>the</strong> 15 millionpeople worldwide whose lives aredisabled by uncontrolled epilepsy— have reason to hope <strong>the</strong>y couldbe offered new, more effective<strong>the</strong>rapies in <strong>the</strong> not-too-distantfuture, thanks to developments inneurobionics.Currently, of <strong>the</strong> one in 100people worldwide who sufferrecurrent seizures throughout <strong>the</strong>irlives, about one-third cannot beadequately treated with availablemedications or surgical <strong>the</strong>rapies,<strong>the</strong> Melbourne neurologist andworld leader in epilepsy treatmenttold <strong>the</strong> recent TeDx Wollongongevent at <strong>the</strong> university of Wollongong,NSW.“A lot of <strong>the</strong> problem with epilepsyrelates to its unpredictability.We have to soak people in medicationsto prevent seizures that mightbe occurring for only a few minutesa year,” says Professor Cook,head of neurology at St vincent’sHospital, Melbourne and chair ofmedicine at <strong>the</strong> university of Melbourne.“It prevents <strong>the</strong>m driving, stopsCould developments in medical bionics lead researchersto <strong>the</strong> ‘Holy Grail’ for treating epilepsy?Megan Howe<strong>the</strong>m from working, threatens<strong>the</strong>ir safety, costs <strong>the</strong>ir life sometimes.”But imagine if people with epilepsycould know when a seizurewas going to occur. And whatif <strong>the</strong> drugs to treat <strong>the</strong> seizurecould be delivered directly to <strong>the</strong>affected part of <strong>the</strong> brain, exactlywhen <strong>the</strong>y are needed. or, evenbetter, what if <strong>the</strong> seizure could beaverted completely?A compact, driven man with<strong>the</strong> knack of explaining exactlywhat his complex research couldmean to patients, Professor Cooktold <strong>the</strong> conference that groundbreakingAustralian research intoimplantable devices is now makingthat kind of control over thisunpredictable condition a real possibility.one of <strong>the</strong> first implantabledevices to be trialled in humans —including 15 Australian patients— is <strong>the</strong> Seizure Advisory System,which predicts when a seizure islikely to occur.Developed by uS companyNeurovista, <strong>the</strong> system involvesneurologist ProfessorMark Cook tells <strong>the</strong>wollongong TeDx eventhow neurobionicscould help people wi<strong>the</strong>pilepsy.permanently implanting electrodeson <strong>the</strong> surface of <strong>the</strong> brainto monitor electrical activity 24hours a day. A pacemaker-likedevice implanted under <strong>the</strong> claviclerecords <strong>the</strong> information andtransmits <strong>the</strong> records, analysesand real-time ambulatory ieeGdata to a small pager-sized devicethat <strong>the</strong> patient carries with <strong>the</strong>m.It has a series of coloured lights:blue indicates a very low risk ofseizures, white indicates a mediumrisk and red indicates a very highrisk.“If effective, it would remove alot of <strong>the</strong> disability from peoplewith seizures — it might let <strong>the</strong>mget to work, play sport, conceivablyeven drive. It might be thatyou can provide <strong>the</strong>rapies when<strong>the</strong>ir status changes on <strong>the</strong> recording,”Professor Cook says.While <strong>the</strong> device hasn’t proved<strong>the</strong> answer for all <strong>the</strong> Australiantrial participants — some have hadit removed and some have gone onto have surgery — for young TasmanianJason Dent it has been lifechanging.In an interview with epilepsyAustralia 10 months after <strong>the</strong>device was implanted, Jason saidthat when a red light appeared on<strong>the</strong> monitor, he took fast-actingmedication. As a result, <strong>the</strong> seizuresthat had previously dom-cont’d next pagewww.australiandoctor.com.au 10 August 2012 | Australian Doctor | 21
news ReVIewfrom previous pageinated his life — occurringsuddenly and without warning —had completely stopped.“I feel more confident in <strong>the</strong>things that I do from day to dayand I enjoy <strong>the</strong> fact that I am nothaving seizures every fortnight,”he said. “I feel like I have morecontrol over my life, as before <strong>the</strong>seizure would come with no warningand stop me doing <strong>the</strong> thingsthat I love doing, like my cricketand timekeeping at <strong>the</strong> local footygames.”Professor Cook says Jason’simplant remains in place and,hope<strong>full</strong>y, can stay <strong>the</strong>re forever.“Suddenly this changes everything.”In fact, <strong>the</strong> potential of <strong>the</strong>sedevices goes beyond simply predicting<strong>the</strong> onset of a seizure.“Conceivably you could usedevices like <strong>the</strong>se to actually control<strong>the</strong> release of drugs,” says ProfessorCook.To try and make this vision areality, he approached nanobionicspioneer Professor Gordon Wallace,founder and director of <strong>the</strong>university of Wollongong IntelligentPolymer Research Institute,and told him he wanted to “putdrugs where <strong>the</strong>y work”.Not having to give antiepilepticssystemically could avoid <strong>the</strong> damagingside effects medication hason <strong>the</strong> CNS and elsewhere in <strong>the</strong>body.“So that’s what we do. We putThe potential of <strong>the</strong>sedevices goes beyondsimply predicting <strong>the</strong>onset of a seizure.<strong>the</strong> drugs we have in polymers andwe implant <strong>the</strong>m — at <strong>the</strong> momentin animals only … over <strong>the</strong> surfaceof <strong>the</strong> brain in <strong>the</strong> part where <strong>the</strong>seizures come from.”eventually, <strong>the</strong> electrically activatedpolymers might be able toactually drive drug release, he says.“Conceivably, we could constructpolymer implants, which could notonly release <strong>the</strong> drug but detect <strong>the</strong>seizure and use <strong>the</strong> energy in <strong>the</strong>seizure itself to release <strong>the</strong> <strong>the</strong>rapy.ELB0185_AD_193x540. pdf Page 1 20/ 06/ 12, 11: 22 AMepilepsy: <strong>the</strong> impactAmong epileptic people and <strong>the</strong>ir family members55%had been injured asa result of a seizure,with 64% of thoserequiring hospitaltreatment for <strong>the</strong>irinjuries48%considered <strong>the</strong>y hadbeen unfairly treatedbecause of <strong>the</strong>irepilepsy at somestage in <strong>the</strong>ir lives16%had <strong>full</strong>-time jobseven though <strong>the</strong>majority were ofworking ageThis would be remarkable.”49%were living below<strong>the</strong> current povertylineFindings of survey of 343 participants on <strong>the</strong> Australian epilepsy Research Register, 87% of whom were people wi<strong>the</strong>pilepsy and 13% were family members and carers.Source: ‘Out of <strong>the</strong> Shadows’: Needs, Perceptions and Experiences of People Living with Epilepsy inAustralia. Findings from Wave 2 of <strong>the</strong> Longitudinal Survey, epilepsy Foundation of victoria, March 2012.78%faced medicinecosts between $11and $300 per monthMarriage of two worldsThe epilepsy research he is conductingwith <strong>the</strong> Intelligent PolymerResearch Institute and <strong>the</strong>Bionics Institute at <strong>the</strong> universityof Melbourne marks a longoverduemarriage of two scientificworlds, says Professor Cook.“I have always been interestedin how to join <strong>the</strong> medical sciencesand <strong>the</strong> material sciences. It is difficultto understand what is possibleif you have never had exposureto what people in this area cando.”While <strong>the</strong>re are still big hurdlesto overcome — <strong>the</strong> formation ofsuitable polymers for diffusing <strong>the</strong>drugs, finding <strong>the</strong> optimal medicationsand ensuring <strong>the</strong> implantsare safe to use in humans — <strong>the</strong>reis an air of optimism among thosein <strong>the</strong> field.Human studies of <strong>the</strong> drug-61%were on multiplemedicines forepilepsy33%reported <strong>full</strong> control(ie, no seizuresover 12 months)infused implants are a couple ofyears away but Professor Cooksays it is entirely plausible that wecould see such devices available totreat uncontrolled epilepsy within5-10 years.And if <strong>the</strong> polymer implantsdo not prove <strong>the</strong> answer, he saysano<strong>the</strong>r approach to suppressingseizures — electrical stimulation of<strong>the</strong> brain — is also under investigationin a project run by <strong>the</strong> BionicsInstitute in collaboration withSt vincent’s Hospital, Melbourne.Ra<strong>the</strong>r than predicting seizures,<strong>the</strong> implantable stimulator devicewill monitor <strong>the</strong> electrical activityof <strong>the</strong> brain via electrodes.If abnormal neural activity isdetected, a <strong>the</strong>rapeutic waveformis <strong>the</strong>n delivered to <strong>the</strong> right partof <strong>the</strong> brain to stop <strong>the</strong> seizure (seeimage above).“It might liberate us altoge<strong>the</strong>rof <strong>the</strong> need to take medications totreat epilepsy,” he suggests.DIagRaM of a DeVICe (lefT): arrays of electrodes surgically implanted on<strong>the</strong> surface of <strong>the</strong> brain will monitor <strong>the</strong> complex patterns of brain activity.These signals will be sent to a processor (similar to a bionic ear stimulator)and proceed to detect/predict <strong>the</strong> epileptic seizure. once a seizure is detected,a <strong>the</strong>rapeutic electrical stimulus can be applied to <strong>the</strong> electrodes in <strong>the</strong>appropriate area of <strong>the</strong> brain to suppress <strong>the</strong> seizure.Image courtesy of Bionics Institute.The new research is finally shininga light at <strong>the</strong> end of a long tunnelfor <strong>the</strong> many people who haveunpredictable and debilitatingepileptic seizures, says epilepsyAustralia chief executive DeniseChapman.Those people face constant anxietyabout when a seizure mightoccur, meaning both <strong>the</strong> loss of<strong>the</strong>ir independence and seriousrisks to <strong>the</strong>ir health.“I think it’s wonderful, it’s avery exciting development,” shesays. “What promise it can holdfor people with very difficult tocontrol epilepsy to have that controland independence, to feel <strong>the</strong>ycan contribute and get out andwork and participate in communitylife, “she says. “It could reallyopen doors.”In a recently published paper on<strong>the</strong>ir research into drug-infusedpolymer-based implants, ProfessorCook and fellow researchersstated: “The Holy Grail has sofar eluded researchers in <strong>the</strong> field,however, strong progress is beingmade.”So are <strong>the</strong>y truly within sight ofepilepsy’s Holy Grail?”“I used that term about beingable to predict seizures and peopleridiculed me,’’ Professor Cookadmits. “We’ve got <strong>the</strong> old systemwhere you ingest drugs and <strong>the</strong>ysoak <strong>the</strong> whole brain. Imagine ifyou could put <strong>the</strong> solution where<strong>the</strong> problem is. I think that is a bitof a <strong>the</strong>rapeutic Holy Grail.” lYou can view <strong>the</strong> <strong>TEDx</strong>Wollongong conference@talks online via www.tedxuwollongong.com, or watch Professor MarkCook’s presentation here: www.tedxuwollongong.com/Mark-CookPBS Information. Restricted Benefi t. For <strong>the</strong> treatmentof Major Depressive Disorder. CYMBALTA is not PBSreimbursed for <strong>the</strong> treatment of Generalised AnxietyDisorder or Diabetic Peripheral Neuropathic Pain.PLEASE REVIEW PRODUCT INFORMATION BEFORE PRESCRIBING.FULL PRODUCT INFORMATION IS AVAILABLE ON REQUESTFROM ELI LILLY.CYMBALTA (duloxetine HCl) 30 mg, 60 mg capsule. INDICATIONS: Treatment of MajorDepressive Disorder (MDD), Diabetic Peripheral Neuropathic Pain (DPNP), Generalised AnxietyDisorder (GAD). CONTRAINDICATIONS: Known hypersensitivity to duloxetine or its excipients,co-administration with MAOI or within 2 weeks after discontinuing MAOI, patients with hepaticimpairment, co-administration with potent CYP1A2 inhibitors. PRECAUTIONS: Clinicalworsening and suicide risk, hepatotoxicity (from LFT elevations to liver failure), substantialalcohol consumption, narrow angle glaucoma, hi<strong>story</strong> of mania, hi<strong>story</strong> of seizure disorder,hyponatraemia, abnormal bleeding , increased blood pressure, orthostatic hypotension/syncope,* serotonin syndrome. OTHER PRECAUTIONS: Pregnancy, including neonatal symptoms with 3rdtrimester use, lactation, children and adolescents, slowed gastric emptying. INTERACTIONS:Concurrent use with serotonergic drugs, CYP1A2 inhibitors (e.g fluvoxamine), CYP2D6substrates (e.g. thioridazine) and inhibitors, MAOI inhibitors, St Johns Wort, warfarin. ADVERSEEFFECTS: Nausea, dry mouth, GI upset, anorexia, fatigue, dizziness, somnolence, tremour,sweating increased, fl ushing, vision blurred, insomnia, sexual dysfunction, palpitations, chills,musculoskeletal pain, headache, lethargy, paraes<strong>the</strong>sia, anxiety, sleep disorder, agitation, yawning.Postmarketing events: restless legs syndrome, seizures on discontinuation, gynaecologicalbleeding. See <strong>full</strong> PI for o<strong>the</strong>rs. DOSAGE AND ADMINISTRATION: MDD & DPNP 60 mg oncedaily; GAD 30 mg to 120 mg once daily. Start with lower dose or administer with food to improveinitial tolerability. Lower dose in end stage renal disease. Taper dose on discontinuation. Basedon PI last amended on 17 Nov 2010. PBS Dispensed Price: 30 mg $38.22; 60 mg $50.42.* Please note changes in Product Information.References: 1. Paykel ES, et al. Psychol Med 1995;25(6):1171–1180. 2. Hirschfeld RMA, et al.Depress Anxiety 2005;21:170–7. 3. CYMBALTA Approved Product Information. 4. American PsychiatricAssociation, Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Text revision, Washington DC:American Psychiatric Association; 2000. Eli Lilly Australia Pty Ltd, ABN 39 000 233 992, 112 WharfRoad, West Ryde, NSW 2114. 06/12 AUCYM00437 ELB0185/ADIs treating mood symptoms enough? 1More patients achieved remission ifresidual symptoms were addressed. 1TREATING MOOD AND MORE † 2,3† Targeting many of <strong>the</strong> symptoms ms of depression –DSM-IV 422 | Australian Doctor | 10 August 2012 www.australiandoctor.com.auwww.australiandoctor.com.au 10 August 2012 | Australian Doctor | 23