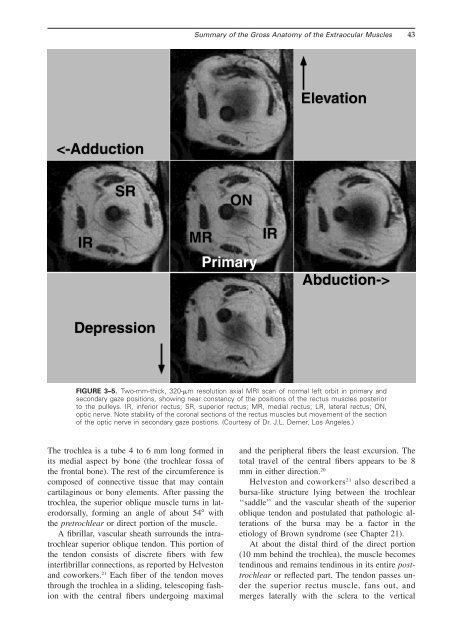
<strong>Summary</strong> <strong>of</strong> <strong>the</strong> <strong>Gross</strong> <strong>Anatomy</strong> <strong>of</strong> <strong>the</strong> <strong>Extraocular</strong> <strong>Muscles</strong> 43FIGURE 3–5. Two-mm-thick, 320-m resolution axial MRI scan <strong>of</strong> normal left orbit in primary andsecondary gaze positions, showing near constancy <strong>of</strong> <strong>the</strong> positions <strong>of</strong> <strong>the</strong> rectus muscles posteriorto <strong>the</strong> pulleys. IR, inferior rectus; SR, superior rectus; MR, medial rectus; LR, lateral rectus; ON,optic nerve. Note stability <strong>of</strong> <strong>the</strong> coronal sections <strong>of</strong> <strong>the</strong> rectus muscles but movement <strong>of</strong> <strong>the</strong> section<strong>of</strong> <strong>the</strong> optic nerve in secondary gaze postions. (Courtesy <strong>of</strong> Dr. J.L. Demer, Los Angeles.)The trochlea is a tube 4 to 6 mm long formed inits medial aspect by bone (<strong>the</strong> trochlear fossa <strong>of</strong><strong>the</strong> frontal bone). The rest <strong>of</strong> <strong>the</strong> circumference iscomposed <strong>of</strong> connective tissue that may containcartilaginous or bony elements. After passing <strong>the</strong>trochlea, <strong>the</strong> superior oblique muscle turns in laterodorsally,forming an angle <strong>of</strong> about 54 with<strong>the</strong> pretrochlear or direct portion <strong>of</strong> <strong>the</strong> muscle.A fibrillar, vascular sheath surrounds <strong>the</strong> intratrochlearsuperior oblique tendon. This portion <strong>of</strong><strong>the</strong> tendon consists <strong>of</strong> discrete fibers with fewinterfibrillar connections, as reported by Helvestonand coworkers. 21 Each fiber <strong>of</strong> <strong>the</strong> tendon movesthrough <strong>the</strong> trochlea in a sliding, telescoping fashionwith <strong>the</strong> central fibers undergoing maximaland <strong>the</strong> peripheral fibers <strong>the</strong> least excursion. Thetotal travel <strong>of</strong> <strong>the</strong> central fibers appears to be 8mm in ei<strong>the</strong>r direction. 20Helveston and coworkers 21 also described abursa-like structure lying between <strong>the</strong> trochlear‘‘saddle’’ and <strong>the</strong> vascular sheath <strong>of</strong> <strong>the</strong> superioroblique tendon and postulated that pathologic alterations<strong>of</strong> <strong>the</strong> bursa may be a factor in <strong>the</strong>etiology <strong>of</strong> Brown syndrome (see <strong>Chapter</strong> 21).At about <strong>the</strong> distal third <strong>of</strong> <strong>the</strong> direct portion(10 mm behind <strong>the</strong> trochlea), <strong>the</strong> muscle becomestendinous and remains tendinous in its entire posttrochlearor reflected part. The tendon passes under<strong>the</strong> superior rectus muscle, fans out, andmerges laterally with <strong>the</strong> sclera to <strong>the</strong> vertical
44 Physiology <strong>of</strong> <strong>the</strong> Sensorimotor Cooperation <strong>of</strong> <strong>the</strong> Eyesinsertion forms a curved concave line toward <strong>the</strong>origin <strong>of</strong> <strong>the</strong> muscle. Its anterior margin is about10 mm behind <strong>the</strong> lower edge <strong>of</strong> <strong>the</strong> insertion <strong>of</strong><strong>the</strong> lateral rectus muscle; its posterior end is 1 mmbelow and 1 to 2 mm in front <strong>of</strong> <strong>the</strong> macula (Fig.3–7). Near its insertion <strong>the</strong> posterior border <strong>of</strong> <strong>the</strong>muscle is related to <strong>the</strong> inferior vortex vein.Unlike <strong>the</strong> o<strong>the</strong>r extraocular muscles, especially<strong>the</strong> superior obliques, which have both muscularand tendinous components, <strong>the</strong> inferioroblique is almost wholly muscular. It forms anangle <strong>of</strong> about 51 with <strong>the</strong> vertical plane <strong>of</strong> <strong>the</strong>globe.FIGURE 3–6. Relationships <strong>of</strong> tendons <strong>of</strong> superioroblique muscle. Measurements are in millimeters. (Modifiedfrom Fink WH: Surgery <strong>of</strong> <strong>the</strong> Vertical <strong>Muscles</strong> <strong>of</strong><strong>the</strong> Eyes, ed 2. Springfield, IL, Charles C Thomas, 1962.)meridian, forming a concave curved line toward<strong>the</strong> trochlea (Fig. 3–6). The anterior end <strong>of</strong> <strong>the</strong>insertion lies 3.0 to 4.5 mm behind <strong>the</strong> lateral end<strong>of</strong> <strong>the</strong> insertion <strong>of</strong> <strong>the</strong> superior rectus muscle and13.8 mm behind <strong>the</strong> corneal limbus. The posteriorend <strong>of</strong> <strong>the</strong> insertion lies 13.6 mm behind <strong>the</strong>medial end <strong>of</strong> <strong>the</strong> insertion <strong>of</strong> <strong>the</strong> superior rectusmuscle and 18.8 mm behind <strong>the</strong> corneal limbus.The width <strong>of</strong> <strong>the</strong> insertion <strong>of</strong> <strong>the</strong> superior obliquemuscle varies greatly (from 7 to 18 mm, Fink 14 )but is 11 mm on average. The medial end <strong>of</strong> <strong>the</strong>insertion lies about 8 mm from <strong>the</strong> posterior pole<strong>of</strong> <strong>the</strong> globe. Near its insertion <strong>the</strong> posterior border<strong>of</strong> <strong>the</strong> muscle is related to <strong>the</strong> superior vortex vein.The length <strong>of</strong> <strong>the</strong> direct part <strong>of</strong> <strong>the</strong> superioroblique muscle is about 40 mm and that <strong>of</strong> <strong>the</strong>reflected tendon is about 19.5 mm. From a physiologicand kinematic standpoint, <strong>the</strong> trochlea is <strong>the</strong>origin <strong>of</strong> <strong>the</strong> muscle.The inferior oblique muscle is <strong>the</strong> shortest <strong>of</strong>all <strong>the</strong> eye muscles, being only 37 mm long. Itarises in <strong>the</strong> anteroinferior angle <strong>of</strong> <strong>the</strong> bony orbitin a shallow depression in <strong>the</strong> orbital plate <strong>of</strong> <strong>the</strong>maxilla near <strong>the</strong> lateral edge <strong>of</strong> <strong>the</strong> entrance into<strong>the</strong> nasolacrimal canal. The origin is readily locatedby drawing a perpendicular line from <strong>the</strong>supraorbital notch to <strong>the</strong> lower orbital margin.The muscle continues from its origin backward,upward, and laterally, passing between <strong>the</strong> floor<strong>of</strong> <strong>the</strong> orbit and <strong>the</strong> inferior rectus muscle. Itinserts by a short tendon (1 to 2 mm) in <strong>the</strong>posterior and external aspect <strong>of</strong> <strong>the</strong> sclera. Thewidth <strong>of</strong> <strong>the</strong> insertion varies widely (5 to 14 mm,Fink 14 ) and may be around 9 mm on average. TheFascial SystemTenon’s CapsuleThe eyeball is suspended within <strong>the</strong> orbit by asystem <strong>of</strong> fasciae. The way in which this isachieved represents an ideal solution to <strong>the</strong> problem<strong>of</strong> suspending a spheroid body in a coneshapedcavity. The bulk <strong>of</strong> <strong>the</strong> system is made up<strong>of</strong> Tenon’s capsule, which is a condensation <strong>of</strong>fibrous tissue that covers <strong>the</strong> eyeball from <strong>the</strong>entrance <strong>of</strong> <strong>the</strong> optic nerve to near <strong>the</strong> corneallimbus, where it is firmly fused with <strong>the</strong> conjunctiva.Except for this area <strong>of</strong> fusion, <strong>the</strong> two structuresare separated by <strong>the</strong> subconjunctival space.Tenon’s capsule is also separated from <strong>the</strong> sclera.Between <strong>the</strong> two is <strong>the</strong> episcleral space (Tenon’sspace), which can be readily injected (Fig. 3–8).On its outer aspect <strong>the</strong> capsule is intimately relatedto <strong>the</strong> orbital reticular tissue. Its posterior edge isFIGURE 3–7. Course <strong>of</strong> inferior oblique muscle and <strong>the</strong>relationships <strong>of</strong> its tendon. Measurements are in millimeters.(Modified from Fink WH: Surgery <strong>of</strong> <strong>the</strong> Vertical<strong>Muscles</strong> <strong>of</strong> <strong>the</strong> Eyes, ed 2. Springfield, IL, Charles CThomas, 1962.)