


Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
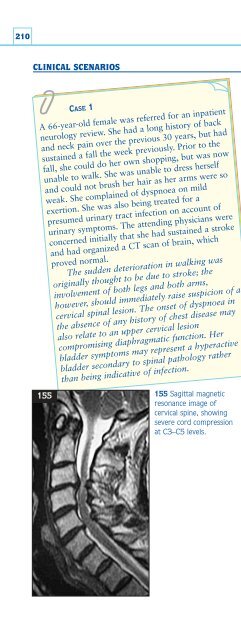
210CLINICAL SCENARIOS155CASE 1A 66-year-old female was referred for an inpatientneurology review. She had a long history of backand neck pain over the previous 30 years, but hadsustained a fall the week previously. Prior to thefall, she could do her own shopping, but was nowunable to walk. She was unable to dress herselfand could not brush her hair as her arms were soweak. She complained of dyspnoea on mildexertion. She was also being treated for apresumed urinary tract infection on account ofurinary symptoms. The attending physicians wereconcerned initially that she had sustained a strokeand had organized a CT scan of brain, whichproved normal.The sudden deterioration in walking wasoriginally thought to be due to stroke; theinvolvement of both legs and both arms,however, should immediately raise suspicion of acervical spinal lesion. The onset of dyspnoea inthe absence of any history of chest disease mayalso relate to an upper cervical lesioncompromising diaphragmatic function. Herbladder symptoms may represent a hyperactivebladder secondary to spinal pathology ratherthan being indicative of infection.155 Sagittal magneticresonance image ofcervical spine, showingsevere cord compressionat C3–C5 levels.The patient was alert and fully orientated.Cardiovascular and respiratory examinationswere normal although the patient was breathlesson minimal exertion. Cranial nerve examinationwas unremarkable. Examination of the upperlimbs revealed increased tone bilaterally,symmetrically reduced power of all movements,and brisk biceps, supinator, and triceps jerks.Sensory testing was normal. In the lower limbs,tone was increased, and there was mildweakness of all movements with increasedreflexes and upgoing plantars.Examination confirmed UMN signs involvingall four limbs: together with the sphincterdisturbance (mid-stream specimens of urine wereconsistently sterile) this would immediately alertthe clinician to a spinal cord lesion at the cervicallevel. Dyspnoea had become prominent and wasanother localizing symptom (muscles ofrespiration are supplied at C3,4, and 5 levels).Speed of onset was quicker than would beexpected for a demyelinating or inflammatorylesion. (In any event, demyelination is rare at thisage.) The timing of the weakness, comingimmediately after a fall, was felt to be more thancoincidental, and it appeared likely that therehad been significant mechanical damage to thecervical spine sustained during (or perhapscontributing to) her fall.MRI of cervical spine showed there to besevere spondylitic and degenerative changes, mostpronounced at higher levels (155). Referral wasmade to the neurosurgeons, who initially refusedto offer operation in view of the risk ofexacerbation. She deteriorated over the next fewweeks, with increasing weakness in both armsand a worsening in respiratory function.It was decided that a conservative policyposed an unacceptably high risk to herrespiratory function. Decompression was carriedout in order to prevent further deterioration, butshe did surprisingly well; she regained hermobility, and has now begun to mobilizeoutdoors with the aid of a zimmer frame.













