

Blood pressure and heart murmurs in a rural population in the ...
Blood pressure and heart murmurs in a rural population in the ...
Blood pressure and heart murmurs in a rural population in the ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
BLOOD PRESSURE AND HEART MURMURS91apex beat was recorded as be<strong>in</strong>g palpable or not,<strong>and</strong> <strong>the</strong> <strong>in</strong>tercostal space <strong>in</strong> which it was located wasnoted. Cardiac <strong>murmurs</strong> were classified accord<strong>in</strong>gto <strong>the</strong>ir <strong>in</strong>tensity as recommended by Rose &Blackburn (14). No dist<strong>in</strong>ction was made betweenejection <strong>and</strong> pansystolic <strong>murmurs</strong>. Murmurs werealso classified accord<strong>in</strong>g to <strong>the</strong>ir area of maximum<strong>in</strong>tensity as apex <strong>and</strong> mitral, left lower border ofsternum (LLBS), pulmonary, aortic, or o<strong>the</strong>r.The age given by <strong>the</strong> subject was accepted if it didnot differ by more than 5 years from that previouslyrecorded at census. If <strong>the</strong> difference was more than5 years, <strong>the</strong> person was questioned on importantdates <strong>in</strong> <strong>the</strong> Republic's recent past; one fifth of <strong>the</strong>subjects were placed <strong>in</strong> a different age group fromthat determ<strong>in</strong>ed by <strong>the</strong> census.RESULTSIn all, 608 persons were exam<strong>in</strong>ed (333 men <strong>and</strong>275 women), <strong>the</strong> overall response rate be<strong>in</strong>g 86 %.These appeared to be no significant differences withregard to age, sex, or geographical location amongthose who did not respond. N<strong>in</strong>ety-five percent of<strong>the</strong> subjects had been resident <strong>in</strong> <strong>the</strong> area for 5 yearsor more, over 90% were farmers, <strong>and</strong> 79% of <strong>the</strong>women <strong>and</strong> 48 % of <strong>the</strong> men had had no formalprimary education.The distributions of systolic <strong>and</strong> diastolic blood<strong>pressure</strong>s for all males <strong>and</strong> all females (Fig. 1 <strong>and</strong> 2)were approximately normal, with close similaritiesbetween males <strong>and</strong> females. The skew to <strong>the</strong> rightis slight but is more marked for systolic than fordiastolic blood <strong>pressure</strong>.The mean systolic <strong>and</strong> diastolic blood <strong>pressure</strong>levels accord<strong>in</strong>g to age <strong>and</strong> sex are given <strong>in</strong> Table I<strong>and</strong> Fig. 3.Systolic blood <strong>pressure</strong>The men showed no significant rise <strong>in</strong> meansystolic blood <strong>pressure</strong> level with age, whereas forwomen <strong>the</strong>re was a consistent rise start<strong>in</strong>g belowTable 1. Mean systolic <strong>and</strong> diastolic(<strong>pressure</strong>s <strong>in</strong> kPa <strong>in</strong> paren<strong>the</strong>ses)blood <strong>pressure</strong>s <strong>in</strong> mmHg by age <strong>and</strong> sexMenWomen aAge group(years) Mean blood SD b Number Mean blood SD Number<strong>pressure</strong><strong>pressure</strong>Systolic25-34 120.1(16.0)11.2 81 117.6(15.6)15.5 6635-44 124.6(16.6)15.5 88 119.0(15.8)20.1 9445-54 122.7(16.3)21.8 75 124.3(16.5)19.1 5855-64 124.6(16.6)19.1 89 126.9(16.9)20.7 57Total 123.1(16.4)17.3 333 121.4(16.1)19.2 275Diastolic25-34 74.4(9.9)11.4 81 72.3(9.6)11.9 6635-44 77.0(10.2)11.6 88 74.8(9.9)11.3 9445-54 76.1(10.1)14.8 75 76.2(10.1)15.1 5855-64 77.5(10.3)13.2 89 75.9(10.1)13.5 57Total 76.3(1 0.1)12.7 333 74.7(9.9)12.8 275a Difference <strong>in</strong> mean blood <strong>pressure</strong> between women aged 25-34 years <strong>and</strong> those aged 55-64 yearsby <strong>the</strong> Student t test = 0.01 > P > 0.005.b SD = st<strong>and</strong>ard deviation.
92J. P. VAUGHANNE1]a11Qp_Males*---* Females__110-0-~~~~~~~~.~ ~- - 025-34 35-44 45-544e group <strong>in</strong> yearsSYSOLIC55-64 All a=Ie:eIJmen (r = 0.08, P>0.05) whereas, although it wasstill low for women, it was significant (r = 0.20,P
BLOOD PRESSURE AND HEART MURMURS93A stepwise multiple regression approach was used<strong>and</strong> a lower level of P
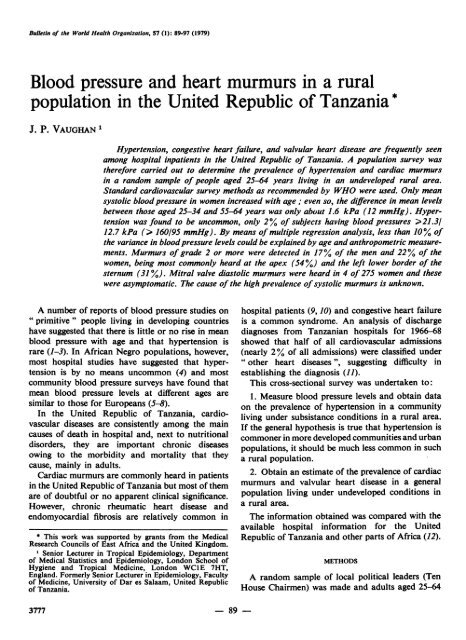
94J. P. VAUGHANln Apex <strong>population</strong> was typical of a <strong>rural</strong> area <strong>and</strong> that<strong>the</strong> survey itself was sound.In <strong>the</strong> present survey, a rise <strong>in</strong> blood <strong>pressure</strong> with[1 _age occurred only <strong>in</strong> women <strong>and</strong> even this rise was20. _ ~a comparatively small one. Two surveys carried outII <strong>in</strong> Nigeria (6, 7) showed that mean blood <strong>pressure</strong>s10lrose with age <strong>in</strong> both men <strong>and</strong> women, <strong>and</strong> Shaper& Saxton (8) found very similar f<strong>in</strong>d<strong>in</strong>gs among <strong>the</strong>Bag<strong>and</strong>a tribe <strong>in</strong> Ug<strong>and</strong>a. However, none of <strong>the</strong>se25-34 35-44 three surveys were carried out <strong>in</strong> a truly <strong>rural</strong>35A44 45-54 55-64AillygeAg4e group <strong>in</strong> years <strong>population</strong>.% FDAI25-34 35-44 45-54Age grup <strong>in</strong> years55-64Fig. 4. The percentage of all subjects <strong>in</strong> each age/sexgroup with systolic <strong>murmurs</strong> (Grade 1 or more) withmaximum <strong>in</strong>tensity at <strong>the</strong> apex or <strong>the</strong> left lower borderof <strong>the</strong> sternum.tomatic. Four were diagnosed as hav<strong>in</strong>g pure mitralstenosis with no evidence of mitral <strong>in</strong>competence or<strong>in</strong>volvement of <strong>the</strong> o<strong>the</strong>r <strong>heart</strong> valves. None hadcardiac failure <strong>and</strong> none had had hospital treatmentfor <strong>heart</strong> compla<strong>in</strong>ts. The fifth person had a soft,blow<strong>in</strong>g, early diastolic Grade 2 murmur maximum<strong>in</strong> <strong>the</strong> LLBS, suggest<strong>in</strong>g aortic <strong>in</strong>competence. Theprevalence of cl<strong>in</strong>ically detected mitral valvulardisease among women 25-64 years of age was, <strong>the</strong>refore,4 out of 275 (1.45%).DISCUSSIONThe survey area was chosen because <strong>the</strong> <strong>population</strong>was typical of <strong>the</strong> undeveloped <strong>rural</strong> areas of <strong>the</strong>United Republic of Tanzania. The sample wasr<strong>and</strong>om <strong>and</strong> <strong>the</strong> response rate high, with no evidencefor bias <strong>in</strong> <strong>the</strong> non-responders with regard to age,sex, or geographical area. The survey methodsfollowed st<strong>and</strong>ard recommended techniques <strong>and</strong>observers were supervised <strong>and</strong> monitored for variation<strong>and</strong> bias. The only significant bias was foundto be a tendency by two observers to read higherdiastolic <strong>pressure</strong>s. All <strong>the</strong>se factors suggest <strong>the</strong>The present survey is one of very few to reveallow blood <strong>pressure</strong>s <strong>in</strong> Africa, particularly <strong>in</strong>African Negro subsistence farm<strong>in</strong>g communities.Huiz<strong>in</strong>ga (2) mentions five communities <strong>in</strong> Africa<strong>in</strong> which blood <strong>pressure</strong> did not appear to rise withage. Two were <strong>in</strong>vestigated by <strong>the</strong> author: <strong>the</strong> Fali(nor<strong>the</strong>rn Cameroon) <strong>and</strong> <strong>the</strong> Kurumba (UpperVolta); two o<strong>the</strong>rs are <strong>the</strong> Ituri Forest pygmies <strong>in</strong>Zaire (17) <strong>and</strong> <strong>the</strong> Kalahari bushmen (18). Thefifth was a small mixed group of immigrants exam<strong>in</strong>edby Shaper & Saxton (8). Similar f<strong>in</strong>d<strong>in</strong>gs have beenreported <strong>in</strong> a <strong>rural</strong> <strong>population</strong> <strong>in</strong> <strong>the</strong> Gambia (19),<strong>and</strong> reports from Papua New Gu<strong>in</strong>ea have suggestedan actual fall <strong>in</strong> mean blood <strong>pressure</strong> with age(20, 21).The 2 % prevalence for hypertension <strong>in</strong> this surveyis very low compared with o<strong>the</strong>r surveys <strong>in</strong> Africa,such as 23% <strong>in</strong> <strong>the</strong> Bag<strong>and</strong>a <strong>in</strong> Ug<strong>and</strong>a (8), 34%among persons 45 years old or more <strong>in</strong> Ug<strong>and</strong>a(22), 5 % among tuberculosis outpatients <strong>in</strong> Ethiopia(23) <strong>and</strong> 20-30% <strong>in</strong> <strong>the</strong> <strong>in</strong>habitants of Lagos city,Nigeria (7). In an analysis of <strong>in</strong>patient admissionsreported by all hospitals <strong>in</strong> <strong>the</strong> United Republicof Tanzania for 1966-68, hypertension accountedfor 0.4% of all admissions (not <strong>in</strong>clud<strong>in</strong>g normalchildbirth) <strong>and</strong> for 20% of cardiovascular admissions.One quarter of all admissions for hypertension were<strong>in</strong> fact reported from a region with 7% of <strong>the</strong> total<strong>population</strong> of <strong>the</strong> country plus <strong>the</strong> capital city (4).Similar urban/<strong>rural</strong> differences have been reportedfrom South Africa, where hypertension was foundto be rare <strong>in</strong> <strong>the</strong> <strong>rural</strong> areas <strong>and</strong> considerably morecommon <strong>in</strong> <strong>the</strong> urban <strong>population</strong>s (24, 25). Studies <strong>in</strong>Papua New Gu<strong>in</strong>ea <strong>and</strong> <strong>the</strong> Pacific area have alsorevealed an almost total absence of hypertension <strong>in</strong><strong>the</strong> adult <strong>population</strong> (26, 27) <strong>and</strong> a review of communitieswithout apparent hypertension has recentlybeen published (3).Age has been found to be <strong>the</strong> most importantexplanatory variable <strong>in</strong> large studies employ<strong>in</strong>gmultiple regression analysis of cross-sectional data
BLOOD PRESSURE AND HEART MURMURS95<strong>in</strong> <strong>the</strong> United States of America (28-30), Israel (31),Belgium (32), <strong>and</strong> India (33). In <strong>the</strong> present study,age was found to be an " explanatory " variableonly <strong>in</strong> women. Some measure of body mass, suchas weight or relative weight, was also found to beimportant <strong>in</strong> <strong>the</strong>se studies.Acheson & Florey (28) were able to expla<strong>in</strong> about40% of <strong>the</strong> variance <strong>in</strong> blood <strong>pressure</strong> levels <strong>in</strong> <strong>the</strong>iranalysis of national data from <strong>the</strong> USA, whereas<strong>the</strong> o<strong>the</strong>r studies mentioned above only expla<strong>in</strong>edbetween 10% (32) <strong>and</strong> 23% (29, 30). The presentstudy expla<strong>in</strong>ed less than 10% of <strong>the</strong> variance.The problems of diagnos<strong>in</strong>g mitral valve lesions<strong>in</strong> <strong>the</strong> tropics are common <strong>and</strong> great; Brock<strong>in</strong>gton& Ed<strong>in</strong>gton (34) remarked <strong>in</strong> <strong>the</strong>ir cl<strong>in</strong>icopathologicalstudy of <strong>heart</strong> disease <strong>in</strong> western Nigeria that <strong>the</strong>ywere a "... major source of diagnostic difficulty<strong>in</strong> wards <strong>and</strong> postmortem rooms ". However, <strong>the</strong>persons <strong>in</strong> this survey who were found to have adiastolic murmur most probably had some organicvalvular lesion <strong>and</strong> <strong>the</strong> prevalence rate for mitralvalve disease of 1.45% <strong>in</strong> women aged 25-64 yearsis quite a high but not unlikely rate (moreover, it isbased on only four cases). There was a notableabsence of diastolic <strong>murmurs</strong> <strong>in</strong> men.Systolic <strong>murmurs</strong> present quite a different picture.All <strong>the</strong> persons were exam<strong>in</strong>ed by <strong>the</strong> author <strong>and</strong><strong>the</strong> prevalence figures for <strong>the</strong> presence of <strong>murmurs</strong>might be expla<strong>in</strong>ed by observer error or bias.However, although this might partly account for<strong>the</strong> high prevalence figures, it is unlikely to be <strong>the</strong>entire explanation because <strong>the</strong> figures <strong>the</strong>mselveswere very high, <strong>the</strong> observations were consistentbetween men <strong>and</strong> women, <strong>and</strong> <strong>the</strong> age prevalencerates for apical <strong>murmurs</strong> rema<strong>in</strong>ed constant whereasthose for <strong>murmurs</strong> maximum at <strong>the</strong> left lower borderof <strong>the</strong> sternum fell. Even if Grade 1 <strong>murmurs</strong> areignored, <strong>the</strong> proportion with Grade 2 or more wasstill surpris<strong>in</strong>gly high; men 17 % <strong>and</strong> women 22 %. All<strong>the</strong>se persons were apparently well. This contrastsmarkedly with hospital studies, where patients areusually given a diagnostic category. There are veryfew references <strong>in</strong> <strong>the</strong> literature to such " benign "systolic <strong>murmurs</strong> among hospital patients. However,Parker (35) found <strong>in</strong> Nairobi that <strong>in</strong> 6% of hiscardiac outpatients <strong>the</strong>re was a systolic murmur<strong>and</strong> noth<strong>in</strong>g else abnormal to be found.In community surveys, similar f<strong>in</strong>d<strong>in</strong>gs wereobta<strong>in</strong>ed by Mann et al. (17) <strong>in</strong> Ituri Forest pygmies<strong>in</strong> Zaire, <strong>in</strong> whom 16% of 186 subjects had a Grade 2murmur or higher. Also, a cardiovascular survey <strong>in</strong><strong>the</strong> vic<strong>in</strong>ity of <strong>the</strong> Albert Schweitzer Hospital <strong>in</strong>Gabon revealed that "... a large amount of unexpla<strong>in</strong>edcardiac disease exists, manifested ma<strong>in</strong>lyby " organic" systolic <strong>murmurs</strong>, cardiomegaly orabnormal ECG's" (36).In <strong>the</strong> present survey, <strong>the</strong> prevalence of systolic<strong>murmurs</strong> was similar <strong>in</strong> <strong>the</strong> two sexes, which suggeststhat causal factors are probably environmentalra<strong>the</strong>r than genetic. Anaemia is not common orsevere enough to expla<strong>in</strong> <strong>the</strong> high prevalence. In<strong>the</strong> tropics streptococcal <strong>in</strong>fections are frequent, highASO titres are commonly found, acute rheumaticfever appears to take on cl<strong>in</strong>ically mild forms, <strong>and</strong><strong>the</strong>re is a high prevalence of chronic rheumatic<strong>heart</strong> disease (37, 38). Could <strong>the</strong>se systolic <strong>murmurs</strong>represent <strong>the</strong> subcl<strong>in</strong>ical aftermath of such a pathologicalprocess?Why <strong>the</strong> proportion of LLBS <strong>murmurs</strong> decreased<strong>in</strong> <strong>the</strong> older age groups is not clear. It might beexpla<strong>in</strong>ed by affected persons dy<strong>in</strong>g earlier, <strong>the</strong>'lesion ' (whatever it might be) heal<strong>in</strong>g, or a cohortphenomenon show<strong>in</strong>g itself by ris<strong>in</strong>g prevalence rates<strong>in</strong> younger age groups. There is no way of differentiat<strong>in</strong>gamong <strong>the</strong>se possibilities with <strong>the</strong> presentdata. Some follow-up <strong>in</strong>formation on <strong>the</strong> personssurveyed might reveal <strong>the</strong> significance of such <strong>murmurs</strong><strong>and</strong> also what happens to <strong>the</strong>m with time.ACKNOWLEDGEMENTS1 wish to thank <strong>the</strong> people who lived <strong>in</strong> <strong>the</strong> survey area for <strong>the</strong>ir cooperation, <strong>and</strong> <strong>the</strong> Dean <strong>and</strong> staff of <strong>the</strong>Faculty of Medic<strong>in</strong>e, Dar es Salaam, for a great deal of help. I was greatly supported <strong>and</strong> guided <strong>in</strong> this project byProfessor C. Wood, Dr P. Hamilton, <strong>and</strong> Dr W. Miall. Particular thanks go to Dr Amri, Dr Mlay, Dr Mgone,Dr Malangalila, Dr Parma, <strong>and</strong> Dr Tesha who, as medical students, helped with <strong>the</strong> survey <strong>and</strong> rema<strong>in</strong>ed enthusiasticthroughout. My thanks also go to Professor M. Backett <strong>and</strong> <strong>the</strong> staff <strong>in</strong> <strong>the</strong> Department of Community Health whowere very encourag<strong>in</strong>g <strong>and</strong> helped with <strong>the</strong> analysis of <strong>the</strong> survey data.
96 J. P. VAUGHANRtSUMPPRESSION ARTERIELLE ET SOUFFLES CARDIAQUES DANS UNE POPULATION RURALEDE LA REPUBLIQUE-UNIE DE TANZANIEL'hypertension est fr6quemment constatee chez les maladessoign6s dans les h6pitaux tanzaniens, et la plupartdes enquetes sur la pression arterielle men&es au se<strong>in</strong>d'autres <strong>population</strong>s d'Afrique noire confirment que lamoyenne de celle-ci pour les diff6rents groupes d'agene differe pas de celle qui s'6tablit dans des <strong>population</strong>seuropeennes. L'<strong>in</strong>suffisance cardiaque globale et les cardiopathiesvalvulaires sont 6galement couramment diagnostiqueeschez les malades adultes; quant aux soufflescardiaques souvent perqus a l'auscultation, ils pr6sentent,pour la plupart, un caractere ben<strong>in</strong> et il est gen6ralementdifficile de les associer a un trouble organique determ<strong>in</strong>e.La presente 6tude a ete faite pour etablir la prevalencede l'hypertension et des souffles cardiaques dans une<strong>population</strong> <strong>rural</strong>e a 6conomie agricole de subsistance.Elle a port6 sur un echantillon al6atoire de 608 <strong>in</strong>dividusages de 25 a 64 ans qui ont ete exam<strong>in</strong>es en appliquantles methodes habituelles de controle cardio-vasculaire.Chez les femmes, la moyenne de la pression arteriellesystolique s'accroit legerement avec l'age, mais non lapression diastolique; chez les hommes, on n'a pasconstat6 d'6l6vation avec l'Age de la pression soitsystolique, soit diastolique. Deux pour cent des sujetspr6sentaient de l'hypertension (pression 6gale ou superieurea 160/95). L'analyse par r6gression multiple amontr6 que l'age constituait une variable significative ence qui concerne la pression systolique et diastolique chezles femmes, mais non chez les hommes. Elle a aussipermis d'etablir que 1'6paisseur du pli cutane figuraitparmi les variables en relation avec le niveau de la pressionart6rielle chez les <strong>in</strong>dividus des deux sexes. Quoiqu'il en soit, ni l'age ni les mesures anthropometriquesn'ont pu expliquer plus de 10% de la variance chez leshommes ou chez les femmes.Un souffle systolique de degre egal ou superieur a 2a e perqu chez 17% des hommes et 22% des femmes.Son <strong>in</strong>tensite maximale se situait a l'apex et dans laregion mitrale (pour 53% des cas) et dans la partie<strong>in</strong>ferieure du bord gauche du sternum (pour 31 % des cas).La proportion de sujets pr6sentant un souffle apexien n'apas paru varier en fonction du groupe d'age, alors quela perception d'un souffle au bord <strong>in</strong>ferieur gauche dusternum dim<strong>in</strong>uait de maniere appreciable avec l'age.On a constate une forte correlation entre la presence d'unbattement de l'apex contre la cage thoracique et celled'un souffle systolique du degre 2 ou plus, a<strong>in</strong>si quecelle d'un certa<strong>in</strong> d6ficit du taux d'hemoglob<strong>in</strong>e. Unsouffle diastolique a ete perqu chez 4 des 275 femmesexam<strong>in</strong>&es et 4 d'entre elles pr6sentaient une cardiopathiemitrale asymptomatique, le taux de morbidit6 par cettemaladie s'etablissant a<strong>in</strong>si a 15 pour 1000 femmes ag6esde 25 a 64 ans. La cause de la forte prevalence du soufflesystolique n'est pas connue, mais on peut se dem<strong>and</strong>ers'il ne constitue pas souvent une sequelle d'<strong>in</strong>fectionstreptococcique.REFERENCES1. LOWENSTEIN, F. W. <strong>Blood</strong> <strong>pressure</strong> <strong>in</strong> relation toage <strong>and</strong> sex <strong>in</strong> <strong>the</strong> tropics <strong>and</strong> subtropics. Lancet,1: 389-392 (1961).2. HUIZINGA, J. Casual blood <strong>pressure</strong> <strong>in</strong> <strong>population</strong>s.In: Vorster, D. J. M., ed. Human biology of environmentalchange. London, International BiologicalProgramme, 1972, p. 164.3. SHAPER, A. G. Communities without hypertension.In: Shaper, A. G. et al., ed. Cardiovascular disease<strong>in</strong> <strong>the</strong> tropics. London, British Medical Association,1974, p. 77.4. VAUGHAN, J. P. Cardiovascular diseases seen <strong>in</strong>Tanzanian hospitals 1966-68. East African medicaljournal, 54: 373-379 (1977).5. ABRAHAMS, D. G. ET AL. The systemic blood <strong>pressure</strong><strong>in</strong> a <strong>rural</strong> West African community. West Africanmedical journal, 9: 45-58 (1960).6. AKINKUGBE, 0. 0. & Ojo, 0. A. Arterial <strong>pressure</strong>s<strong>in</strong> <strong>rural</strong> <strong>and</strong> urban <strong>population</strong>s <strong>in</strong> Nigeria. Britishmedical journal, 2: 222-224 (1969).7. JOHNSON, 0. T. Arterial blood <strong>pressure</strong>s <strong>and</strong> hypertension<strong>in</strong> an urban African <strong>population</strong> sample.British journal of preventive <strong>and</strong> social medic<strong>in</strong>e,25: 26-33 (1971).8. SHAPER, A. G. & SAXTON, G. A. <strong>Blood</strong> <strong>pressure</strong> <strong>and</strong>body build <strong>in</strong> a <strong>rural</strong> community <strong>in</strong> Ug<strong>and</strong>a. EastAfrican medical journal, 46: 228-245 (1969).9. NHONOLI, A. M. Heart disease <strong>in</strong> Dar es Salaam.East African medical journal, 45: 118-121 (1968).10. SPENCER, S. S. & MAKENE, W. J. Rheumatic <strong>heart</strong>disease <strong>in</strong> Tanzania. East African medical journal,49: 909-920 (1972).11. VAUGHAN, J. P. Brief review of cardiovasculardisease <strong>in</strong> Africa. Transactions of <strong>the</strong> Royal Societyof Tropical Medic<strong>in</strong>e <strong>and</strong> Hygiene, 71: 226-231 (1977).
BLOOD PRESSURE AND HEART MURMURS 9712. NHONOLI, A. M. The <strong>in</strong>cidence of hypertensive <strong>heart</strong>disease <strong>in</strong> Dar es Salaam. East African medicaljournal, 46: 55-57 (1969).13. WRIGHT, B. M. & DORE, C. F. A r<strong>and</strong>om zerosphygmomanometer. Lancet, 1: 337-338 (1970).14. ROSE, G. A. & BLACKBURN, H. Cardiovascularsurvey methods. Geneva, World Health Organization,1968 (Monograph Series, No. 56).15. ROSE, G. A. St<strong>and</strong>ardisation of observers <strong>in</strong> blood<strong>pressure</strong> measurement. Lancet, 1: 673-674 (1965).16. WHO Technical Report Series, No. 168, 1959(Hypertension <strong>and</strong> coronary <strong>heart</strong> disease: classification<strong>and</strong> criteria for epidemiological studies. Firstreport of <strong>the</strong> Expert Committee on CardiovascularDiseases <strong>and</strong> Hypertension).17. MANN, G. V. ET AL. Cardiovascular disease <strong>in</strong>African pygmies. Journal of chronic diseases, 15:341-371 (1962).18. KAMINER, B. & LUTZ, W. P. W. <strong>Blood</strong> <strong>pressure</strong> <strong>in</strong><strong>the</strong> bushmen of <strong>the</strong> Kalahari Desert. Circulation,32: 289-295 (1960).19. REE, G. H. Arterial <strong>pressure</strong>s <strong>in</strong> a West African(Gambian) <strong>rural</strong> <strong>population</strong>. Journal of tropicalmedic<strong>in</strong>e <strong>and</strong> hygiene, 76: 65-70 (1973).20. MADDOCKS, I. & RovIN, L. A New Gu<strong>in</strong>ea <strong>population</strong><strong>in</strong> which blood <strong>pressure</strong> appears to fall as ageadvances. Papua New Gu<strong>in</strong>ea medical journal,8: 17-21 (1965).21. STANHOPE, J. M. Population studies <strong>in</strong> Papua NewGu<strong>in</strong>ea. S<strong>in</strong>gapore medicaljournal, 14: 228-229(1973).22. IKEME, A. C. ET AL. A survey for cardiovasculardisease <strong>in</strong> middle aged Ug<strong>and</strong>ans. Bullet<strong>in</strong> of <strong>the</strong>World Health Organization, 48: 751-753 (1973).23. PARRY, E. H. 0. Ethiopian cardiovascular studies.III: <strong>the</strong> casual blood <strong>pressure</strong> <strong>in</strong> Ethiopian highl<strong>and</strong>ers<strong>in</strong> Addis Ababa. East African medicaljournal, 46: 246-256 (1969).24. SCOTCH, N. A. A prelim<strong>in</strong>ary report on <strong>the</strong> relationof sociocultural factors to hypertension among <strong>the</strong>Zulu. Annals of <strong>the</strong> New York Academy of Sciences,84: 1000-1009 (1960).25. EDGINGTON, M. E. ET AL. Disease patterns <strong>in</strong> a SouthAfrican <strong>rural</strong> Bantu <strong>population</strong>. South Africanmedical journal, 46: 968-976 (1972).26. MADDOCKS, I. Possible absence of essential hypertension<strong>in</strong> two complete Pacific Isl<strong>and</strong> <strong>population</strong>s.Lancet, 2: 396 (1961).27. PRIOR, Epidemiology of cardiovascular diseases <strong>in</strong>Asian-Pacific region. S<strong>in</strong>gapore medical journal,14: 223-227. (1973).28. ACHESON, R. M. & FLOREY, C. DU V. Predict<strong>in</strong>gblood <strong>pressure</strong> from age, physique, blood glucose<strong>and</strong> serum cholesterol <strong>in</strong> a national sample of <strong>the</strong>USA (1960-62). Archives rouma<strong>in</strong>es de pathologieexperimentale et de microbiologie, 28: 131-136 (1969).29. STAMLER, J. ET AL. Multivariate analysis of <strong>the</strong>relationship of six variables to blood <strong>pressure</strong>:f<strong>in</strong>d<strong>in</strong>gs from Chicago community surveys, 1965-71Journal of chronic diseases, 28: 499-525 (1975).30. STAMLER, J. ET AL. Multivariate analysis of <strong>the</strong>relationship of seven variables to blood <strong>pressure</strong>:f<strong>in</strong>d<strong>in</strong>gs of <strong>the</strong> Chicago Heart Association detectionproject <strong>in</strong> <strong>in</strong>dustry, 1967-72. Journal of chronicdiseases, 28: 527-548 (1975).31. SIVE, P. H. ET AL. Distribution <strong>and</strong> multiple regressionanalysis of blood <strong>pressure</strong> <strong>in</strong> 10,000 Israeli men.American journal of epidemiology, 93: 317-327 (1971).32. KESTELOOT, H. & VAN HOUTE, 0. An epidemiologicsurvey of arterial blood <strong>pressure</strong> <strong>in</strong> a large male<strong>population</strong> group. American journal of epidemiology,99: 14-29 (1974).33. BAGCHI, S. C. & INDRAYAN, A. Multivariate analysisof blood <strong>pressure</strong> correlates <strong>in</strong> an Indian urbancommunity. Indian journal of public health, 18:93-104 (1973).34. BROCKINGTON, I. F. & EDINGTON, G. M. Adult<strong>heart</strong> disease <strong>in</strong> western Nigeria: a cl<strong>in</strong>icopathologicalsynopsis. American <strong>heart</strong> journal, 83: 27-40(1972).35. PARKER, A. H. T. Cardiac disorders <strong>in</strong> Nairobi.East African medical journal, 50: 530-536 (1973).36. MILLER, D. C. ET AL. Survey of cardiovasculardisease among Africans <strong>in</strong> <strong>the</strong> vic<strong>in</strong>ity of <strong>the</strong> AlbertSchweitzer Hospital <strong>in</strong> 1960. American journal ofcardiology, 10: 432-446 (1962).37. SHAPER, A. G. Cardiovascular disease <strong>in</strong> <strong>the</strong> tropics.British medical journal, 3: 682-686 (1972).38. STOLLERMAN, G. H. Streptococcus, rheumatic fever<strong>and</strong> rheumatic <strong>heart</strong> disease. In: Shaper, A. G. et al.,ed. Cardiovascular disease <strong>in</strong> <strong>the</strong> tropics. London,British Medical Association, 1974, pp. 7-21.













