- Page 1 and 2:
D. Richard Laws · William O'Donohu
- Page 4 and 5:
D. Richard Laws • William O’Don
- Page 6 and 7:
Pref ace It can be wise for a field
- Page 8 and 9:
Contents 1 Problems in the Classifi
- Page 10 and 11:
Contributors Adam J. Carter , Ph.D.
- Page 12 and 13:
Chapter 1 Problems in the Classific
- Page 14 and 15:
1 Problems in the Classification an
- Page 16 and 17:
1 Problems in the Classification an
- Page 18 and 19:
1 Problems in the Classification an
- Page 20 and 21:
1 Problems in the Classification an
- Page 22 and 23:
1 Problems in the Classification an
- Page 24 and 25:
1 Problems in the Classification an
- Page 26 and 27:
1 Problems in the Classification an
- Page 28 and 29:
1 Problems in the Classification an
- Page 30 and 31:
20 L.A. Craig and M. Rettenberger O
- Page 32 and 33:
Table 2.1 Glueck and Glueck’s ( 1
- Page 34 and 35:
24 L.A. Craig and M. Rettenberger w
- Page 36 and 37:
26 L.A. Craig and M. Rettenberger L
- Page 38 and 39:
28 L.A. Craig and M. Rettenberger T
- Page 40 and 41:
30 L.A. Craig and M. Rettenberger T
- Page 42 and 43:
32 L.A. Craig and M. Rettenberger b
- Page 44 and 45:
34 L.A. Craig and M. Rettenberger (
- Page 46 and 47:
36 L.A. Craig and M. Rettenberger r
- Page 48 and 49:
38 L.A. Craig and M. Rettenberger v
- Page 50 and 51:
40 L.A. Craig and M. Rettenberger C
- Page 52 and 53:
42 L.A. Craig and M. Rettenberger H
- Page 54 and 55:
44 L.A. Craig and M. Rettenberger T
- Page 56 and 57:
46 R.J.B. Lehmann et al. at reducin
- Page 58 and 59:
48 R.J.B. Lehmann et al. Certain pa
- Page 60 and 61:
50 R.J.B. Lehmann et al. these cons
- Page 62 and 63:
52 R.J.B. Lehmann et al. to other m
- Page 64 and 65:
54 R.J.B. Lehmann et al. Developing
- Page 66 and 67:
56 R.J.B. Lehmann et al. ( d = 0.67
- Page 68 and 69:
58 R.J.B. Lehmann et al. justified
- Page 70 and 71:
60 R.J.B. Lehmann et al. (any convi
- Page 72 and 73:
62 R.J.B. Lehmann et al. press ) fo
- Page 74 and 75:
64 R.J.B. Lehmann et al. Importantl
- Page 76 and 77:
66 R.J.B. Lehmann et al. United Sta
- Page 78 and 79:
68 R.J.B. Lehmann et al. offenders
- Page 80 and 81:
70 R.J.B. Lehmann et al. A good def
- Page 82 and 83:
72 R.J.B. Lehmann et al. Conclusion
- Page 84 and 85:
74 R.J.B. Lehmann et al. Babchishin
- Page 86 and 87:
76 R.J.B. Lehmann et al. Grove, W.
- Page 88 and 89:
78 R.J.B. Lehmann et al. Hilton, N.
- Page 90 and 91:
80 R.J.B. Lehmann et al. Pedneault,
- Page 92 and 93:
Chapter 4 Risk Formulation: The New
- Page 94 and 95:
4 Risk Formulation: The New Frontie
- Page 96 and 97:
4 Risk Formulation: The New Frontie
- Page 98 and 99:
4 Risk Formulation: The New Frontie
- Page 100 and 101:
4 Risk Formulation: The New Frontie
- Page 102 and 103:
4 Risk Formulation: The New Frontie
- Page 104 and 105:
4 Risk Formulation: The New Frontie
- Page 106 and 107:
4 Risk Formulation: The New Frontie
- Page 108 and 109:
4 Risk Formulation: The New Frontie
- Page 110 and 111:
4 Risk Formulation: The New Frontie
- Page 112 and 113:
4 Risk Formulation: The New Frontie
- Page 114 and 115:
4 Risk Formulation: The New Frontie
- Page 116 and 117:
108 R.J. Wilson and M.H. Miner Conv
- Page 118 and 119:
110 R.J. Wilson and M.H. Miner Circ
- Page 120 and 121: 112 R.J. Wilson and M.H. Miner Visu
- Page 122 and 123: 114 R.J. Wilson and M.H. Miner gyne
- Page 124 and 125: 116 R.J. Wilson and M.H. Miner View
- Page 126 and 127: 118 R.J. Wilson and M.H. Miner comp
- Page 128 and 129: 120 R.J. Wilson and M.H. Miner stim
- Page 130 and 131: 122 R.J. Wilson and M.H. Miner sign
- Page 132 and 133: 124 R.J. Wilson and M.H. Miner In t
- Page 134 and 135: 126 R.J. Wilson and M.H. Miner sexu
- Page 136 and 137: 128 R.J. Wilson and M.H. Miner Babc
- Page 138 and 139: 130 R.J. Wilson and M.H. Miner King
- Page 140 and 141: Chapter 6 Polygraph Testing of Sex
- Page 142 and 143: 6 Polygraph Testing of Sex Offender
- Page 144 and 145: 6 Polygraph Testing of Sex Offender
- Page 146 and 147: 6 Polygraph Testing of Sex Offender
- Page 148 and 149: 6 Polygraph Testing of Sex Offender
- Page 150 and 151: 6 Polygraph Testing of Sex Offender
- Page 152 and 153: 6 Polygraph Testing of Sex Offender
- Page 154 and 155: 6 Polygraph Testing of Sex Offender
- Page 156 and 157: 6 Polygraph Testing of Sex Offender
- Page 158 and 159: 6 Polygraph Testing of Sex Offender
- Page 160 and 161: 6 Polygraph Testing of Sex Offender
- Page 162 and 163: 6 Polygraph Testing of Sex Offender
- Page 164 and 165: Chapter 7 The Strengths of Treatmen
- Page 166 and 167: 7 The Strengths of Treatment for Se
- Page 168 and 169: 7 The Strengths of Treatment for Se
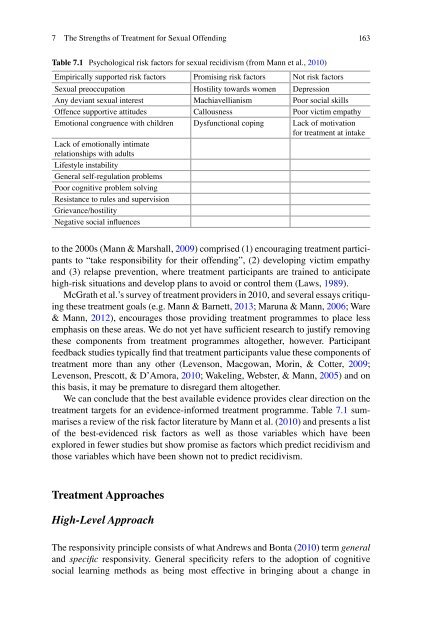
- Page 172 and 173: 7 The Strengths of Treatment for Se
- Page 174 and 175: 7 The Strengths of Treatment for Se
- Page 176 and 177: 7 The Strengths of Treatment for Se
- Page 178 and 179: 7 The Strengths of Treatment for Se
- Page 180 and 181: 7 The Strengths of Treatment for Se
- Page 182 and 183: Chapter 8 Responsivity Dynamic Risk
- Page 184 and 185: 8 Responsivity Dynamic Risk Factors
- Page 186 and 187: 8 Responsivity Dynamic Risk Factors
- Page 188 and 189: 8 Responsivity Dynamic Risk Factors
- Page 190 and 191: 8 Responsivity Dynamic Risk Factors
- Page 192 and 193: 8 Responsivity Dynamic Risk Factors
- Page 194 and 195: 8 Responsivity Dynamic Risk Factors
- Page 196 and 197: 8 Responsivity Dynamic Risk Factors
- Page 198 and 199: Chapter 9 Early Detection and Inter
- Page 200 and 201: 9 Early Detection and Intervention
- Page 202 and 203: 9 Early Detection and Intervention
- Page 204 and 205: 9 Early Detection and Intervention
- Page 206 and 207: 9 Early Detection and Intervention
- Page 208 and 209: 9 Early Detection and Intervention
- Page 210 and 211: 9 Early Detection and Intervention
- Page 212 and 213: 9 Early Detection and Intervention
- Page 214 and 215: 9 Early Detection and Intervention
- Page 216 and 217: 9 Early Detection and Intervention
- Page 218 and 219: 9 Early Detection and Intervention
- Page 220 and 221:
9 Early Detection and Intervention
- Page 222 and 223:
9 Early Detection and Intervention
- Page 224 and 225:
9 Early Detection and Intervention
- Page 226 and 227:
9 Early Detection and Intervention
- Page 228 and 229:
9 Early Detection and Intervention
- Page 230 and 231:
Chapter 10 Community Control of Sex
- Page 232 and 233:
10 Community Control of Sex Offende
- Page 234 and 235:
10 Community Control of Sex Offende
- Page 236 and 237:
10 Community Control of Sex Offende
- Page 238 and 239:
10 Community Control of Sex Offende
- Page 240 and 241:
10 Community Control of Sex Offende
- Page 242 and 243:
10 Community Control of Sex Offende
- Page 244 and 245:
10 Community Control of Sex Offende
- Page 246 and 247:
10 Community Control of Sex Offende
- Page 248 and 249:
10 Community Control of Sex Offende
- Page 250 and 251:
244 K.N. Daly SVP laws were passed
- Page 252 and 253:
246 K.N. Daly 750. 338 b. The condu
- Page 254 and 255:
248 K.N. Daly had largely been a re
- Page 256 and 257:
250 K.N. Daly By contrast successfu
- Page 258 and 259:
252 K.N. Daly In reaching his concu
- Page 260 and 261:
254 K.N. Daly with no accompanying
- Page 262 and 263:
256 K.N. Daly legal significance of
- Page 264 and 265:
258 K.N. Daly law which has caused
- Page 266 and 267:
Chapter 12 The Shortcomings of Sexu
- Page 268 and 269:
12 The Shortcomings of Sexual Offen
- Page 270 and 271:
12 The Shortcomings of Sexual Offen
- Page 272 and 273:
12 The Shortcomings of Sexual Offen
- Page 274 and 275:
12 The Shortcomings of Sexual Offen
- Page 276 and 277:
12 The Shortcomings of Sexual Offen
- Page 278 and 279:
12 The Shortcomings of Sexual Offen
- Page 280 and 281:
12 The Shortcomings of Sexual Offen
- Page 282 and 283:
12 The Shortcomings of Sexual Offen
- Page 284 and 285:
12 The Shortcomings of Sexual Offen
- Page 286 and 287:
282 P. Lussier practitioners have r
- Page 288 and 289:
284 P. Lussier refers to someone vo
- Page 290 and 291:
286 P. Lussier Morton, & Harris, 20
- Page 292 and 293:
288 P. Lussier The authors compared
- Page 294 and 295:
290 P. Lussier relatively stable ch
- Page 296 and 297:
292 P. Lussier Offending Trajectori
- Page 298 and 299:
294 P. Lussier impact or a limited
- Page 300 and 301:
296 P. Lussier especially those han
- Page 302 and 303:
298 P. Lussier the role of social f
- Page 304 and 305:
300 P. Lussier Mulvey, 2009 ). In f
- Page 306 and 307:
302 P. Lussier opportunities and re
- Page 308 and 309:
304 P. Lussier Peer Influence While
- Page 310 and 311:
306 P. Lussier of offending. For ex
- Page 312 and 313:
308 P. Lussier Aging, self-identity
- Page 314 and 315:
310 P. Lussier & Rice, 2007 ; Lussi
- Page 316 and 317:
312 P. Lussier Individual and Socia
- Page 318 and 319:
314 P. Lussier als subject to incre
- Page 320 and 321:
316 P. Lussier opportunities extent
- Page 322 and 323:
318 P. Lussier Corrado, R. R., Cohe
- Page 324 and 325:
320 P. Lussier Lussier, P., & Blokl
- Page 326 and 327:
322 P. Lussier Stouthamer-Loeber, M
- Page 328 and 329:
324 J. Tabachnick et al. community
- Page 330 and 331:
326 J. Tabachnick et al. Fig. 14.1
- Page 332 and 333:
328 J. Tabachnick et al. The Need f
- Page 334 and 335:
330 J. Tabachnick et al. The CDC de
- Page 336 and 337:
332 J. Tabachnick et al. Practical
- Page 338 and 339:
334 J. Tabachnick et al. (e.g., tru
- Page 340 and 341:
336 J. Tabachnick et al. Unfortunat
- Page 342 and 343:
338 J. Tabachnick et al. Banyard, V
- Page 344 and 345:
340 J. Tabachnick et al. Humphries,
- Page 346 and 347:
342 J. Tabachnick et al. Tharp, A.
- Page 348 and 349:
344 Index Adolescent sexually abusi
- Page 350 and 351:
346 Index Offense-supportive attitu
- Page 352:
348 Index Structured assessment of