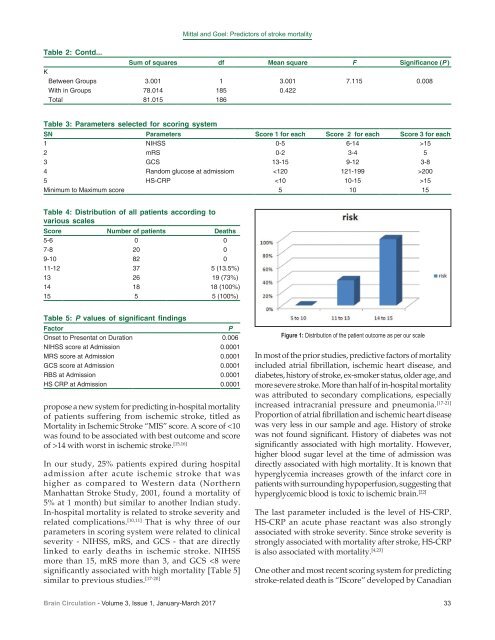
Mittal and Goel: Predictors of <strong>stroke</strong> mortality Table 2: Contd... Sum of squares df Mean square F Significance (P ) K Between Groups 3.001 1 3.001 7.115 0.008 With <strong>in</strong> Groups 78.014 185 0.422 Total 81.015 186 Table 3: Parameters selected for scor<strong>in</strong>g system SN Parameters Score 1 for each Score 2 for each Score 3 for each 1 NIHSS 0-5 6-14 >15 2 mRS 0-2 3-4 5 3 GCS 13-15 9-12 3-8 4 Random glucose at admissiom 200 5 HS-CRP 15 M<strong>in</strong>imum to Maximum <strong>score</strong> 5 10 15 Table 4: Distribution of all patients accord<strong>in</strong>g to various scales Score Number of patients Deaths 5-6 0 0 7-8 20 0 9-10 82 0 11-12 37 5 (13.5%) 13 26 19 (73%) 14 18 18 (100%) 15 5 5 (100%) Table 5: P values of significant f<strong>in</strong>d<strong>in</strong>gs Factor P Onset to Presentat on Duration 0.006 NIHSS <strong>score</strong> at Admission 0.0001 MRS <strong>score</strong> at Admission 0.0001 GCS <strong>score</strong> at Admission 0.0001 RBS at Admission 0.0001 HS CRP at Admission 0.0001 propose a new system for predict<strong>in</strong>g <strong>in</strong>-hospital mortality of patients suffer<strong>in</strong>g from <strong>ischemic</strong> <strong>stroke</strong>, titled as <strong>Mortality</strong> <strong>in</strong> Ischemic Stroke “MIS” <strong>score</strong>. A <strong>score</strong> of 14 with worst <strong>in</strong> <strong>ischemic</strong> <strong>stroke</strong>. [15,16] In our study, 25% patients expired dur<strong>in</strong>g hospital admission after acute <strong>ischemic</strong> <strong>stroke</strong> that was higher as compared to Western data (Northern Manhattan Stroke Study, 2001, found a mortality of 5% at 1 month) but similar to another Indian study. In‐hospital mortality is related to <strong>stroke</strong> severity and related complications. [10,11] That is why three of our parameters <strong>in</strong> scor<strong>in</strong>g system were related to cl<strong>in</strong>ical severity ‐ NIHSS, mRS, and GCS ‐ that are directly l<strong>in</strong>ked to early deaths <strong>in</strong> <strong>ischemic</strong> <strong>stroke</strong>. NIHSS more than 15, mRS more than 3, and GCS
Mittal and Goel: Predictors of <strong>stroke</strong> mortality <strong>stroke</strong> society. Multivariable predictors of 30‐day and 1‐year mortality <strong>in</strong>cluded older age, male sex, severe <strong>stroke</strong>, nonlacunar <strong>stroke</strong> subtype, glucose ≥7.5 mmol/L (135 mg/dL), history of atrial fibrillation, coronary artery disease, congestive heart failure, cancer, dementia, kidney disease on dialysis, and dependency before the <strong>stroke</strong>. Based on these factors, a risk <strong>score</strong> <strong>in</strong>dex stratified the risk of death at 30 days and 1 year and identified low‐ and high‐risk <strong>in</strong>dividuals. [24] This system <strong>in</strong>cludes all parameters for short as well as long‐term mortality, so it is more extensive and therefore little lengthy for bedside utility and is more useful for long‐term mortality. The mortality <strong>in</strong> <strong>ischemic</strong> <strong>stroke</strong> <strong>score</strong> (MISS) system is applicable for prediction of <strong>in</strong>‐hospital mortality <strong>in</strong> <strong>stroke</strong> patients at presentation. It is short, simple, and easy to apply as it uses bedside cl<strong>in</strong>ical scales and simple <strong>in</strong>vestigations whose results are quickly available. The selected parameters for MISS are related to cl<strong>in</strong>ical severity of <strong>stroke</strong> and are helpful for early prediction of MIS. The radiological assessment of bra<strong>in</strong> parenchyma <strong>in</strong>volvement is not relied upon s<strong>in</strong>ce different recoveries with similar parenchyma <strong>in</strong>volvement have been noted. Besides size of the <strong>in</strong>farct may not accurately def<strong>in</strong>e, the severity as a small‐sized <strong>in</strong>farct <strong>in</strong> a crucial area may do more harm than a large <strong>in</strong>farct <strong>in</strong> a relatively less critical area. Conclusion Our MIS system can effectively predict the mortality <strong>in</strong> patients with <strong>ischemic</strong> <strong>stroke</strong> at the time of presentation and thereby help physicians and neurologists predict the outcome of patients at the presentation to the hospital. F<strong>in</strong>ancial support and sponsorship Nil. Conflicts of <strong>in</strong>terest There are no conflicts of <strong>in</strong>terest. References 1. Jencks SF, Daley J, Draper D, Thomas N, Lenhart G, Walker J. Interpret<strong>in</strong>g hospital mortality data. The role of cl<strong>in</strong>ical risk adjustment. JAMA 1988;260:3611‐6. 2. Vemmos KN, Bots ML, Tsibouris PK, Zis VP, Takis CE, Grobbee DE, et al. Prognosis of <strong>stroke</strong> <strong>in</strong> the South of Greece: 1 year mortality, functional outcome and its determ<strong>in</strong>ants: The Arcadia Stroke Registry. J Neurol Neurosurg Psychiatry 2000;69:595‐600. 3. Matz K, Keresztes K, Tatschl C, Nowotny M, Dachenhausen A, Bra<strong>in</strong><strong>in</strong> M, et al. Disorders of glucose metabolism <strong>in</strong> acute <strong>stroke</strong> patients: An underrecognized problem. Diabetes Care 2006;29:792‐7. 4. Fuentes B, Castillo J, San José B, Leira R, Serena J, Vivancos J, et al. The prognostic value of capillary glucose levels <strong>in</strong> acute <strong>stroke</strong>: The GLycemia <strong>in</strong> acute <strong>stroke</strong> (GLIAS) study. Stroke 2009;40:562‐8. 5. Capes SE, Hunt D, Malmberg K, Pathak P, Gerste<strong>in</strong> HC. Stress hyperglycemia and prognosis of <strong>stroke</strong> <strong>in</strong> nondiabetic and diabetic patients: A systematic overview. Stroke 2001;32:2426‐32. 6. Elk<strong>in</strong>d MS, Tai W, Coates K, Paik MC, Sacco RL. High‐sensitivity C‐reactive prote<strong>in</strong>, lipoprote<strong>in</strong>‐associated phospholipase A2, and outcome after <strong>ischemic</strong> <strong>stroke</strong>. Arch Intern Med 2006;166:2073‐80. 7. Smith WS, English JD, Claiborne Johnston S. Cerebrovascular diseases. In: Fauci Anthony S, Eugene B, Kasper Dennis L, Hauser Stephen L, Longo Dan L, Larry JJ, et al., editors. Harrison’s Pr<strong>in</strong>ciples of Internal Medic<strong>in</strong>e. 17 th ed. New York: The McGraw‐Hill Companies, Inc.; 2008. p. 2513‐36. 8. Kaul S, Bandaru VC, Suvarna A, Boddu DB. Stroke burden and risk factors <strong>in</strong> develop<strong>in</strong>g countries with special reference to India. J Indian Med Assoc 2009;107:358, 367‐70. 9. Ll<strong>in</strong>as Rafael H. Overview of the approach to the <strong>stroke</strong> patient. In: Wityk Robert J, Ll<strong>in</strong>as Rafael H, editors. Stroke. Mumbai: Aramuc India Ltd.; 2007. p. 1‐4. 10. Towfighi A, Saver JL. Stroke decl<strong>in</strong>es from third to fourth lead<strong>in</strong>g cause of death <strong>in</strong> the United States: Historical perspective and challenges ahead. Stroke 2011;42:2351‐5. 11. Balami JS, Chen RL, Grunwald IQ, Buchan AM. Neurological complications of acute ischaemic <strong>stroke</strong>. Lancet Neurol 2011;10:357‐71. 12. Hemphill JC 3 rd , Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH <strong>score</strong>: A simple, reliable grad<strong>in</strong>g scale for <strong>in</strong>tracerebral hemorrhage. Stroke 2001;32:891‐7. 13. Adams HP Jr., Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, et al. Classification of subtype of acute <strong>ischemic</strong> <strong>stroke</strong>. Def<strong>in</strong>itions for use <strong>in</strong> a multicenter cl<strong>in</strong>ical trial. TOAST. Trial of Org 10172 <strong>in</strong> acute <strong>stroke</strong> treatment. Stroke 1993;24:35‐41. 14. Bushnell C. Another <strong>score</strong> to predict <strong>ischemic</strong> <strong>stroke</strong> mortality? Circulation 2011;123:712‐3. 15. Wong KS. Risk factors for early death <strong>in</strong> acute <strong>ischemic</strong> <strong>stroke</strong> and <strong>in</strong>tracerebral hemorrhage: A prospective hospital‐based study <strong>in</strong> Asia. Asian Acute Stroke Advisory Panel. Stroke 1999;30:2326‐30. 16. Heuschmann PU, Kolom<strong>in</strong>sky‐Rabas PL, Misselwitz B, Hermanek P, Leffmann C, Janzen RW, et al. Predictors of <strong>in</strong>‐hospital mortality and attributable risks of death after <strong>ischemic</strong> <strong>stroke</strong>: The German Stroke Registers Study Group. Arch Intern Med 2004;164:1761‐8. 17. Bhatia RS, Garg RK, Gaur SP, Kar AM, Shukla R, Agarwal A, et al. Predictive value of rout<strong>in</strong>e hematological and biochemical parameters on 30‐day fatality <strong>in</strong> acute <strong>stroke</strong>. Neurol India 2004;52:220‐3. 18. Clark Wayne M, Hourhane Maurice J. Cl<strong>in</strong>ical <strong>stroke</strong> scales. In: Herndon Robert M, editor. Handbook of Neurologic Rat<strong>in</strong>g Scales. 2 nd ed. New York: Demos Medical Publish<strong>in</strong>g, Inc.; 2006. p. 261‐84. 19. Yoneda Y, Uehara T, Yamasaki H, Kita Y, Tabuchi M, Mori E. Hospital‐based study of the care and cost of acute <strong>ischemic</strong> <strong>stroke</strong> <strong>in</strong> Japan. Stroke 2003;34:718‐24. 20. Sulter G, Steen C, De Keyser J. Use of the Barthel <strong>in</strong>dex and modified Rank<strong>in</strong> scale <strong>in</strong> acute <strong>stroke</strong> trials. Stroke 1999;30:1538‐41. 21. Hartmann A, Rundek T, Mast H, Paik MC, Boden‐Albala B, Mohr JP, et al. <strong>Mortality</strong> and causes of death after first <strong>ischemic</strong> <strong>stroke</strong>: The Northern Manhattan <strong>stroke</strong> study. Neurology 2001;57:2000‐5. 22. Wong AA, Read SJ. Early changes <strong>in</strong> physiological variables after <strong>stroke</strong>. Ann Indian Acad Neurol 2008;11:207‐20. 23. Idicula TT, Brogger J, Naess H, Waje‐Andreassen U, Thomassen L. Admission C‐reactive prote<strong>in</strong> after acute <strong>ischemic</strong> <strong>stroke</strong> is associated with <strong>stroke</strong> severity and mortality: The ‘Bergen <strong>stroke</strong> study’. BMC Neurol 2009;9:18. 24. Saposnik G, Kapral MK, Liu Y, Hall R, O’Donnell M, Raptis S, et al. IScore: A risk <strong>score</strong> to predict death early after hospitalization for an acute <strong>ischemic</strong> <strong>stroke</strong>. Circulation 2011;123:739‐49. 34 Bra<strong>in</strong> Circulation - Volume 3, Issue 1, January-March 2017