SOLO Member Guidebook

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
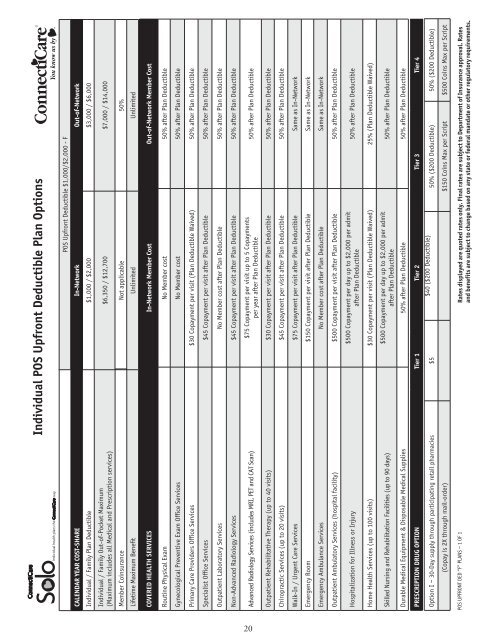
Individual POS Upfront Deductible Plan Options<br />
CALENDAR YEAR COST-SHARE<br />
Individual / Family Plan Deductible<br />
Individual / Family Out-of-Pocket Maximum<br />
(Maximum includes all Medical and Prescription services)<br />
<strong>Member</strong> Coinsurance<br />
Lifetime Maximum Benefit<br />
POS Upfront Deductible $1,000/$2,000 - F<br />
In-Network Out-of-Network<br />
$1,000 / $2,000 $3,000 / $6,000<br />
$6,350 / $12,700 $7,000 / $14,000<br />
Not applicable 50%<br />
Unlimited Unlimited<br />
COVERED HEALTH SERVICES In-Network <strong>Member</strong> Cost Out-of-Network <strong>Member</strong> Cost<br />
Routine Physical Exam No <strong>Member</strong> cost 50% after Plan Deductible<br />
Gynecological Preventive Exam Office Services No <strong>Member</strong> cost 50% after Plan Deductible<br />
Primary Care Providers Office Services $30 Copayment per visit (Plan Deductible Waived) 50% after Plan Deductible<br />
Specialist Office Services $45 Copayment per visit after Plan Deductible 50% after Plan Deductible<br />
Outpatient Laboratory Services No <strong>Member</strong> cost after Plan Deductible 50% after Plan Deductible<br />
Non-Advanced Radiology Services $45 Copayment per visit after Plan Deductible 50% after Plan Deductible<br />
Advanced Radiology Services (includes MRI, PET and CAT Scan)<br />
$75 Copayment per visit up to 5 Copayments<br />
per year after Plan Deductible<br />
50% after Plan Deductible<br />
Outpatient Rehabilitative Therapy (up to 40 visits) $30 Copayment per visit after Plan Deductible 50% after Plan Deductible<br />
Chiropractic Services (up to 20 visits) $45 Copayment per visit after Plan Deductible 50% after Plan Deductible<br />
Walk-In / Urgent Care Services $75 Copayment per visit after Plan Deductible Same as In-Network<br />
Emergency Room $150 Copayment per visit after Plan Deductible Same as In-Network<br />
Emergency Ambulance Services No <strong>Member</strong> cost after Plan Deductible Same as In-Network<br />
Outpatient Ambulatory Services (hospital facility) $500 Copayment per visit after Plan Deductible 50% after Plan Deductible<br />
Hospitalization for Illness or Injury<br />
$500 Copayment per day up to $2,000 per admit<br />
after Plan Deductible<br />
50% after Plan Deductible<br />
Home Health Services (up to 100 visits) $30 Copayment per visit (Plan Deductible Waived) 25% (Plan Deductible Waived)<br />
Skilled Nursing and Rehabilitation Facilities (up to 90 days)<br />
$500 Copayment per day up to $2,000 per admit<br />
after Plan Deductible<br />
50% after Plan Deductible<br />
Durable Medical Equipment & Disposable Medical Supplies 50% after Plan Deductible 50% after Plan Deductible<br />
PRESCRIPTION DRUG OPTION Tier 1 Tier 2 Tier 3 Tier 4<br />
Option I – 30-Day supply through participating retail pharmacies $5<br />
$40 ($200 Deductible)<br />
50% ($200 Deductible) 50% ($200 Deductible)<br />
(Copay is 2X through mail-order) $150 Coins Max per Script $500 Coins Max per Script<br />
POS UPFRONT DED “F” PLANS – 1 OF 1<br />
Rates displayed are quoted rates only. Final rates are subject to Department of Insurance approval. Rates<br />
and benefits are subject to change based on any state or federal mandate or other regulatory requirements.<br />
20