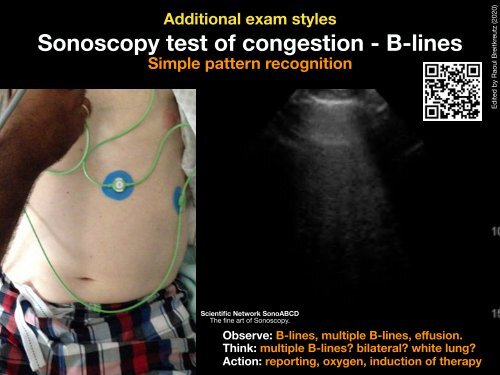
Additional exam styles Sonoscopy test of congestion - B-lines Simple pattern recognition Edited by Raoul Breitkreutz (2020) Scientific Network SonoABCD The fine art of Sonoscopy. Observe: B-lines, multiple B-lines, effusion. Think: multiple B-lines? bilateral? white lung? Action: reporting, oxygen, induction of therapy
Review article nt, especially in its specificity value. Different settings, operperience, Ultrasonography and timing of the for ultrasound confirmation can cause of a endotracheal small but was tube used placement: in ten studies. 9,11,12,14–20 The sensitivity and spe mon ultrasound technique to detect esophageal intubatio nificant A influence on the diagnostic accuracy. Ultrasonogran be a useful tool for confirmation of tracheal intubation. real-time sonographic imaging during intubation has higher are both high in cadaveric models, ORs, and EDs. In ge systematic review and meta-analysis er, Eric the use H. Chou of ultrasonography a,1 , Eitan Dickmanor a , any Po-Yang method Tsouas b , Mark the sole Tessarotivity a , Yang-Ming for detection Tsai c , of esophageal Additional intubation information than post-intu Matthew Huei-Ming Ma d , Chien-Chang Lee c,d,∗ , John Marshall a a Department of Emergency Medicine, Maimonides Medical Center, Brooklyn, NY, USA b College of Medicine, National Yang-Ming University, Taipei, Taiwan c Department of Emergency Medicine, National Taiwan University Hospital Yunlin Branch, Douliou, Taiwan d Department of Emergency Medicine, National Taiwan University Hospital, Taipei, Taiwan <strong>Resuscitation</strong> 90 (2015) 97–103 a r t i c l e i n f o Article history: Received 19 November 2014 Received in revised form 11 February 2015 Accepted 12 February 2015 Keywords: Intubation Airway management Ultrasonography <strong>Resuscitation</strong> Meta-analysis Critical care a b s t r a c t Objective: This study aimed to undertake a systematic review and meta-analysis to summarize evidence on the diagnostic value of ultrasonography for the assessment of endotracheal tube placement in adult patients. Methods: The major databases, PubMed, EMBASE, and the Cochrane Library, were searched for studies published from inception to June 2014. We selected studies that used ultrasonography to confirm endotracheal tube placement. The search was limited to human studies, and had no publication date or country restrictions. Exclusion criteria included case reports, comments, reviews, guidelines and animal studies. Two reviewers extracted and verified the data independently. We summarized test performance characteristics with the use of forest plots, hierarchical summary receiver operating characteristic (HSROC) curves, and bivariate random effect models. Meta-regression analysis was performed to explore the source of heterogeneity. The methodological quality of individual studies was evaluated using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool. Results: A total of 12 eligible studies involving adult patients and cadaveric models were identified from 1488 references. For detection of esophageal intubation, the pooled sensitivity was 0.93 (95%CI: 0.86–0.96) and the specificity was 0.97 (95%CI: 0.95–0.98). The area under the summary ROC curve was 0.97 (95%CI: 0.95–0.98). The positive and negative likelihood ratios were 26.98 (95%CI: 19.32–37.66) and 0.08 (95%CI: 0.04–0.15), respectively. Conclusions: Current evidence supports that ultrasonography has high diagnostic value for identifying esophageal intubation. With optimal sensitivity and specificity, ultrasonography can be a valuable adjunct in this aspect of airway assessment, especially in situations where capnography may be unreliable. © 2015 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Tracheal intubation serves as definite airway control when resuscitating critically ill patients. Confirmation of proper tube placement should be completed in all patients at the time of initial intubation. Unrecognized misplacement of the endotracheal tube may lead to avoidable morbidity including neurological damage, and death, with a reported incidence of 6–16%. 1,2 Thus, immediate post-intubation airway assessment is an essential clinical skill for every physician in emergency medicine (EM), anesthesia and critical care medicine. There are multiple options for confirming tracheal intubation and all methods have unique limitations. 3–5 According to the 2010 American Heart Association (AHA) guideline,
- Page 1 and 2: ALS-conformed Resuscitation Ultraso
- Page 3 and 4: Sonoscopy of trachea in emergencies
- Page 5 and 6: Distinct clinical emergency scenari
- Page 7 and 8: Team H.K. Stanis, M.D., M. Negele,
- Page 9 and 10: Team H.K. Stanis, M.D., M. Negele,
- Page 11 and 12: Distinct clinical emergency scenari
- Page 13 and 14: Sonoscopy of trachea during intubat
- Page 15 and 16: Team K. Stanis, M.D., M. Negele, Ba
- Page 17 and 18: Sonoscopy of lung post-intubation C
- Page 19 and 20: Team Markus Geuting, M.D., M. Negel
- Page 21 and 22: Team Markus Geuting, M.D., M. Negel
- Page 23 and 24: Airway Ultrasound Exam Limitations
- Page 25 and 26: Sonoscopy of lung post-intubation C
- Page 27 and 28: Additional information Airway Ultra
- Page 29 and 30: Additional information Types of air
- Page 31 and 32: Additional exam styles Sonoscopy of
- Page 33: Additional exam styles Sonoscopy te
- Page 37 and 38: Sonoscopy of lung post-intubation C
- Page 39 and 40: 30% VF only >60% PEA / asystole
- Page 41 and 42: The solution is 1) With training AL
- Page 43 and 44: 2015
- Page 45 and 46: 2016 1. Cardiac activity on ultraso
- Page 48 and 49: Is Resuscitation Ultrasound = „Em
- Page 50 and 51: low-cost, available at www.SonoABCD
- Page 52 and 53: During CPR subcostal window Edited
- Page 54 and 55: asystole, after cessation no flow s
- Page 56 and 57: Pseudo - EMD parasternal, LAX Court
- Page 58 and 59: Tamponade subcostal window paraster
- Page 60 and 61: Signs of acute right heart pressure
- Page 62 and 63: Signs of hypovolemia IVC, SAX, tran
- Page 64: IVC , eye-balling, B-Mode Edited by
- Page 67 and 68: VCI, LAX - Pitfall false Diameter (
- Page 69 and 70: Therapy: Puncture/Aspiration, Lysis
- Page 71 and 72: Urgent (specialist / cardiologist w
- Page 73 and 74: ALS-conformed Resuscitation Ultraso