Volume 3, Issue 5 - Midwest Orthopaedics at Rush
Volume 3, Issue 5 - Midwest Orthopaedics at Rush
Volume 3, Issue 5 - Midwest Orthopaedics at Rush

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
6<br />
12<br />
20<br />
Cover Story<br />
Beyond Bumps and Bruises<br />
MOR enhances pedi<strong>at</strong>ric orthopaedic offerings ..............................................................6<br />
Sports Medicine<br />
Twisting and Turning<br />
Ankle sprains are the most common sports injury ......................................................10<br />
Staying in the Game<br />
Winter sports leave knees vulnerable ...........................................................................12<br />
Reality Check for Young Athletes<br />
Long-term effects of overuse injuries are a serious concern ........................................16<br />
Diagnostics and Tre<strong>at</strong>ment<br />
Making Strides<br />
Controversy surrounds the tre<strong>at</strong>ment of idiop<strong>at</strong>hic toe walking ..................................20<br />
ITW Defined<br />
Distinctive characteristics help pinpoint tiptoe gait .....................................................24<br />
Technology Insights<br />
Dict<strong>at</strong>ion Goes Digital<br />
Online pl<strong>at</strong>form makes cassette tapes obsolete ...........................................................26<br />
Smart Tools in Practice<br />
Technology allows physicians to focus on the p<strong>at</strong>ient ..................................................30<br />
In Every <strong>Issue</strong><br />
<strong>Volume</strong> 3 • <strong>Issue</strong> 5<br />
President’s Letter ....................................................................................................4<br />
Chairman’s Letter .....................................................................................................5<br />
Physician Listing .......................................................................................................5<br />
Directory.....................................................................................................................33<br />
Orthopaedic Excellence is published by QuestCorp Media Group, Inc., 885 E. Collins Blvd., Ste. 102, Richardson,<br />
TX 75081. Phone (972) 447-0910 or (888) 860-2442, fax (972) 447-0911, www.qcmedia.com. QuestCorp specializes<br />
in cre<strong>at</strong>ing and publishing corpor<strong>at</strong>e magazines for businesses. Inquiries: Victor Horne, vhorne@qcmedia.<br />
com. Editorial comments: Darren Nielsen, dnielsen@qcmedia.com. Please call or fax for a new subscription,<br />
change of address, or single copy. Single copies: $5.95. This public<strong>at</strong>ion may not be reproduced in part or in whole<br />
without the express written permission of QuestCorp Media Group, Inc. To advertise in an upcoming issue of this<br />
public<strong>at</strong>ion, please contact us <strong>at</strong> (888) 860-2442 or visit us on the Web <strong>at</strong> www.qcmedia.com. March 2007<br />
Orthopaedic Excellence
President’s Letter<br />
I<br />
hope 2006 was as good a year for all of you as it was for <strong>Midwest</strong> <strong>Orthopaedics</strong><br />
<strong>at</strong> <strong>Rush</strong> (MOR). We were proud to see the <strong>Rush</strong> University Medical<br />
Center (<strong>Rush</strong>) Orthopaedic Program continue its move up in the ranks in<br />
U.S.News & World Report’s “America’s Best Hospitals.” In three years we have<br />
moved from 10th to sixth in the n<strong>at</strong>ion, and we expect to keep this positive<br />
momentum going.<br />
We also continued to grow and expand our organiz<strong>at</strong>ion and service lines during 2006 by<br />
adding a number of new physicians and subspecialties. First, we filled the pedi<strong>at</strong>ric ortho-<br />
paedic surgeon void by signing Monica Kogan, MD, who comes to MOR from Children’s<br />
Hospital in Oakland, California. Dr. Kogan started with MOR in October and has been a<br />
fantastic addition to our organiz<strong>at</strong>ion. We feel very fortun<strong>at</strong>e to have Dr. Kogan as a part<br />
of our team and are pleased to be able to provide these much-needed services.<br />
Our Pedi<strong>at</strong>ric Program was further strengthened with the addition of Jeffrey Mjaanes, MD,<br />
a primary care sports medicine physician. In August, Dr. Mjaanes joined us part-time after<br />
completing his primary care sports medicine fellowship <strong>at</strong> Advoc<strong>at</strong>e Lutheran General.<br />
Dr. Mjaanes primarily practices <strong>at</strong> the Winfield office and supports our Athletic Training<br />
Outreach Program. Two days a week he also continues as a practicing pedi<strong>at</strong>rician with<br />
<strong>Rush</strong>’s pedi<strong>at</strong>ric department.<br />
Another new addition in 2006 was Johnny Lin, MD, a foot and ankle specialist. Dr. Lin is<br />
st<strong>at</strong>ioned primarily <strong>at</strong> our Winfield office, but he also sees p<strong>at</strong>ients <strong>at</strong> <strong>Rush</strong> and Oak Park<br />
Hospitals. MOR was well-acquainted with Dr. Lin because he completed his orthopaedic<br />
residency <strong>at</strong> <strong>Rush</strong> before his fellowship training <strong>at</strong> the renowned Campbell Clinic in Nashville.<br />
We believe th<strong>at</strong> Dr. Lin, as the third physician member of the foot and ankle team, will provide<br />
the critical mass the program needs to take off, both clinically and academically.<br />
In January, longtime, highly regarded spinal deformity surgeons Christopher DeWald, MD, and<br />
K.W. Hammerberg, MD, joined our team. The addition of Drs. DeWald and Hammerberg consolid<strong>at</strong>es<br />
most of the <strong>Rush</strong> Orthopaedic Program under the MOR banner. It also immedi<strong>at</strong>ely<br />
established MOR as one of the leading spinal deformity practices in the n<strong>at</strong>ion.<br />
Adding world-renowned physicians and surgeons was not the only thing MOR was up to in<br />
2006. We also added a new loc<strong>at</strong>ion. The Westchester p<strong>at</strong>ient office opened in November and<br />
is providing a wide range of orthopaedic services in a convenient loc<strong>at</strong>ion. In addition, the st<strong>at</strong>eof-the-art<br />
orthopaedic ambul<strong>at</strong>ory building on <strong>Rush</strong>’s campus is expected to open in 2009.<br />
Lastly, we are proud and excited to continue our team rel<strong>at</strong>ionships with the Bulls, White Sox,<br />
World Champion Chicago <strong>Rush</strong>, Chicago Bandits, and other sports teams and cultural arts<br />
programs. If there is anything we can do to improve your experience with our organiz<strong>at</strong>ion,<br />
please contact me or MOR’s CEO, Dennis Viellieu, <strong>at</strong> (708) 236-2611.<br />
Here’s to good health and a gre<strong>at</strong> year for all!<br />
Charles A. Bush-Joseph, MD<br />
Managing Member, <strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong>, LLC<br />
cbj@rushortho.com<br />
Orthopaedic Excellence<br />
A public<strong>at</strong>ion from<br />
<strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong><br />
www.rushortho.com<br />
Central DuPage Hospital<br />
25 North Winfield Rd.<br />
Winfield, IL 60190<br />
Toll free: (877) MD-BONES<br />
Phone: (630) 682-5653<br />
Fax: (630) 682-8946<br />
Chicago — South Loop/River City<br />
800 South Wells, Ste. M30<br />
Chicago, IL 60607<br />
Toll free: (877) MD-BONES<br />
Phone: (312) 431-3400<br />
Fax: (312) 427-6116<br />
Prairie Medical Center of Westchester<br />
2450 South Wolf Rd., Ste. F<br />
Westchester, IL 60154<br />
Toll free: (877) MD-BONES<br />
Phone: (708) 236-2750<br />
Fax: (708) 562-6875<br />
Oak Park Hospital<br />
Medical Office Building<br />
610 South Maple Ave., Ste. 1400<br />
Oak Park, IL 60304<br />
Toll free: (877) MD-BONES<br />
Phone: (312) 243-4244<br />
Fax: (312) 942-1517<br />
RUSH University Medical Center<br />
1725 West Harrison St., Ste. 1063<br />
Chicago, IL 60612<br />
Toll free: (877) MD-BONES<br />
Phone: (312) 243-4244<br />
Fax: (312) 942-1517
Physician Listing<br />
Howard An, MD<br />
Spine, Back, and Neck<br />
Gunnar Andersson, MD<br />
Spine, Back, and Neck<br />
Bernard Bach Jr., MD<br />
Sports Medicine<br />
Richard Berger, MD<br />
Joint Reconstruction<br />
Charles Bush-Joseph, MD<br />
Sports Medicine, Knee, Shoulder,<br />
and Hip<br />
Mark Cohen, MD<br />
Hand, Wrist, and Elbow<br />
Brian Cole, MD<br />
Sports Medicine, Cartilage Restor<strong>at</strong>ion<br />
Craig Della Valle, MD<br />
Joint Reconstruction<br />
Christopher DeWald, MD<br />
Spine, Back, and Neck<br />
John Fernandez, MD<br />
Hand, Wrist, and Elbow<br />
April Fetzer, DO<br />
Physical Medicine/<br />
Pain Management<br />
Jorge Galante, MD<br />
Joint Reconstruction<br />
Steven Gitelis, MD<br />
Orthopaedic Oncology/<br />
Joint Reconstruction<br />
Edward Goldberg, MD<br />
Spine, Back, and Neck<br />
K.W. Hammerberg, MD<br />
Spinal Surgery<br />
George Holmes Jr., MD<br />
Foot and Ankle<br />
Joshua Jacobs, MD<br />
Joint Reconstruction<br />
Monica Kogan, MD<br />
Pedi<strong>at</strong>ric <strong>Orthopaedics</strong><br />
Simon Lee, MD<br />
Foot and Ankle<br />
Johnny Lin, MD<br />
Foot and Ankle<br />
Jeffrey Mjaanes, MD<br />
Sports Medicine and<br />
Pedi<strong>at</strong>ric Sports Medicine<br />
Gregory Nicholson, MD<br />
Shoulder and Elbow, Sports Medicine,<br />
and Knee<br />
Trish Palmer, MD<br />
Sports Medicine and<br />
Women’s Sports Medicine<br />
Wayne Paprosky, MD<br />
Hip and Knee Joint Reconstruction<br />
Frank Phillips, MD<br />
Spine, Back, and Neck<br />
Anthony Romeo, MD<br />
Sports Medicine, Elbow,<br />
and Shoulder<br />
Aaron Rosenberg, MD<br />
Joint Reconstruction<br />
Mitchell Sheinkop, MD<br />
Joint Reconstruction<br />
Kern Singh, MD<br />
Spine, Back, and Neck<br />
Scott Sporer, MD<br />
Hip and Knee Joint Reconstruction<br />
Nikhil Verma, MD<br />
Sports Medicine, Knee, Elbow,<br />
and Shoulder<br />
Walter Virkus, MD<br />
Orthopaedic Oncology/Trauma<br />
K<strong>at</strong>hleen Weber, MD<br />
Sports Medicine and<br />
Women’s Sports Medicine<br />
The <strong>Rush</strong> University Medical Center (<strong>Rush</strong>)<br />
Orthopaedic Program continues to climb in the<br />
U.S.News & World Report’s rankings, moving up<br />
to sixth in the n<strong>at</strong>ion in 2006. This continued improvement<br />
in the annual rankings valid<strong>at</strong>es the commitment<br />
and excellence of our physicians, researchers, and staff, as well as<br />
wh<strong>at</strong> we already knew: We are one of the best orthopaedic departments<br />
in the country.<br />
I’m pleased to announce further consolid<strong>at</strong>ion on the part of the<br />
practicing physicians <strong>at</strong> <strong>Rush</strong>. Drs. DeWald and Hammerberg have<br />
decided to merge with <strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong> (MOR),<br />
adding two n<strong>at</strong>ionally renowned deformity surgeons to our already<br />
highly successful spine practice. Consolid<strong>at</strong>ion is key as we move<br />
forward into new and better space.<br />
Regarding the orthopaedic ambul<strong>at</strong>ory building project, we continue<br />
to make gre<strong>at</strong> progress. Eventually, this project will allow us to consolid<strong>at</strong>e<br />
all of our <strong>Rush</strong> and downtown practice facilities and provide<br />
complete diagnostic and outp<strong>at</strong>ient tre<strong>at</strong>ment for p<strong>at</strong>ients with all<br />
types of musculoskeletal injuries and diseases.<br />
In addition to the ambul<strong>at</strong>ory building project, we are expanding<br />
our diagnostic facilities to include the l<strong>at</strong>est technology and developing<br />
a large physical therapy facility capable of accommod<strong>at</strong>ing our<br />
everyday p<strong>at</strong>ients as well as world-class professional <strong>at</strong>hletes. I’d also<br />
like to mention the learning center we are planning, where we will<br />
dissemin<strong>at</strong>e our knowledge and inventions to other physicians and<br />
the l<strong>at</strong>est products will be brought in for the benefit of our residents<br />
and fellows.<br />
All in all, 2006 was a tremendous year for MOR. We experienced<br />
continued clinical growth and were awarded large research grants from<br />
federal and industry sources. As we continue to grow, I am confident<br />
we will continue to provide efficient, high-quality, and compassion<strong>at</strong>e<br />
services to our p<strong>at</strong>ients.<br />
Best regards,<br />
Gunnar Andersson, MD, PhD<br />
Chairman, Department of Orthopaedic Surgery<br />
<strong>Rush</strong> University Medical Center<br />
Chairman’s Letter<br />
Orthopaedic Excellence
Need Kicker<br />
Orthopaedic Excellence<br />
Beyond<br />
Bumps and<br />
Bruises<br />
MOR enhances pedi<strong>at</strong>ric<br />
orthopaedic offerings<br />
By Paul Strandquist
<strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong><br />
(MOR) has long had a gap in its<br />
service line, but it has not been<br />
alone. During the last five years, the hardest<br />
subspecialty to fill by far has been pedi<strong>at</strong>ric<br />
orthopaedics. With some recent additions<br />
to the team, MOR has filled th<strong>at</strong> hole and<br />
then some.<br />
In August, MOR added Jeffrey Mjaanes, MD,<br />
a primary care sports medicine specialist and<br />
pedi<strong>at</strong>rician. In October, the group added<br />
Monica Kogan, MD, a pedi<strong>at</strong>ric orthopaedic<br />
surgeon. Further strengthening the team,<br />
longtime, highly regarded, n<strong>at</strong>ionally recognized<br />
<strong>Rush</strong> University Medical Center<br />
(<strong>Rush</strong>) spinal deformity surgeons Christopher<br />
DeWald, MD, and K.W. Hammerberg,<br />
MD, came on board in January.<br />
These additions help s<strong>at</strong>isfy the demands<br />
of referral sources and p<strong>at</strong>ients clamoring<br />
for pedi<strong>at</strong>ric orthopaedic services. Parents,<br />
referring physicians, therapists, <strong>at</strong>hletic<br />
trainers, and coaches can turn to MOR for<br />
complete, comprehensive pedi<strong>at</strong>ric orthopaedic<br />
care for all injuries and pedi<strong>at</strong>ric<br />
orthopaedic conditions.<br />
“The addition of these physicians and pedi<strong>at</strong>ric<br />
services will help us in providing the<br />
best, broadest, and most convenient menu<br />
of orthopaedic services possible for our<br />
p<strong>at</strong>ients,” says Charles A. Bush-Joseph, MD,<br />
Managing Member <strong>at</strong> MOR.<br />
About Monica Kogan, MD<br />
Dr. Kogan is a medical gradu<strong>at</strong>e from the<br />
University of Illinois College of Medicine<br />
in Chicago. She completed a residency <strong>at</strong><br />
Northwestern Memorial Hospital and a<br />
fellowship <strong>at</strong> Primary Children’s Medical<br />
Center, a renowned pedi<strong>at</strong>ric center in Salt<br />
Lake City, Utah, th<strong>at</strong> serves five st<strong>at</strong>es in the<br />
intermountain region.<br />
Before joining MOR, Dr. Kogan spent the<br />
previous five years <strong>at</strong> Children’s Hospital<br />
and Research Center in Oakland, California.<br />
Dr. Kogan is proud to bring her educ<strong>at</strong>ion<br />
and experience to MOR in the tre<strong>at</strong>ment of<br />
children’s broken bones and other orthopaedic<br />
problems unique to pedi<strong>at</strong>ric p<strong>at</strong>ients.<br />
Dr. Kogan will tre<strong>at</strong> trauma, birth defects,<br />
developmental dysplasia, clubfoot, genetic<br />
anomalies, neurologic dysfunction, scoliosis,<br />
and walking disorders.<br />
“I am excited to be a part of a multispecialty<br />
practice like MOR. We now have a complete<br />
team of fellowship-trained subspecialty<br />
“The addition of these<br />
physicians and pedi<strong>at</strong>ric<br />
services will help us<br />
in providing the best,<br />
broadest, and most<br />
convenient menu of<br />
orthopaedic services<br />
possible for our p<strong>at</strong>ients.”<br />
physicians th<strong>at</strong> can diagnose and tre<strong>at</strong> any<br />
type of orthopaedic injury or disorder,” she<br />
says. And the feeling is mutual. Everyone <strong>at</strong><br />
MOR is pleased to have a pedi<strong>at</strong>ric orthopaedic<br />
surgeon on the team — especially one as<br />
skilled as Dr. Kogan.<br />
About Jeffrey Mjaanes, MD<br />
– Charles A. Bush-Joseph, MD<br />
Children’s sports have certainly changed<br />
since the days of baseball on the prairie,<br />
pickup hockey games in the alley, and tag in<br />
the neighborhood until the street lights came<br />
on. Now there are youth sports programs,<br />
clubs, and elite training facilities open yearround.<br />
Youth soccer, gymnastics, baseball,<br />
and wrestling schedules domin<strong>at</strong>e parents’<br />
calendars and travel schedules. This is where<br />
Dr. Mjaanes comes in.<br />
Dr. Mjaanes has a unique background in<br />
pedi<strong>at</strong>ric medicine and offers a wide range of<br />
services to MOR p<strong>at</strong>ients. “I am trained in<br />
primary care sports medicine and therefore<br />
can tre<strong>at</strong> all sports injuries and problems<br />
experienced by all ages. But I am also a pedi<strong>at</strong>rician<br />
and have an interest and specialize<br />
in preventing and tre<strong>at</strong>ing pedi<strong>at</strong>ric sports<br />
injuries,” says Dr. Mjaanes.<br />
He is a gradu<strong>at</strong>e of the University of Wisconsin<br />
School of Medicine in Madison,<br />
and he completed a residency in pedi<strong>at</strong>rics<br />
<strong>at</strong> <strong>Rush</strong> University Medical Center in<br />
Chicago. He then completed a fellowship<br />
in primary care sports medicine <strong>at</strong> Advoc<strong>at</strong>e<br />
Lutheran General Hospital in Park<br />
Ridge, Illinois.<br />
With his training in sports medicine,<br />
Dr. Mjaanes’ goal is to get child <strong>at</strong>hletes<br />
on the road to recovery as soon as possible.<br />
His training also gives him the skills<br />
to tre<strong>at</strong> nonorthopaedic sports injuries<br />
and problems, including he<strong>at</strong> illness, he<strong>at</strong><br />
stroke, concussion, and wrestling rashes.<br />
He also performs pre-particip<strong>at</strong>ion physicals<br />
for school <strong>at</strong>hletic programs and sports<br />
teams. Both Dr. Mjaanes and Dr. Kogan are<br />
fluent in Spanish.<br />
About Christopher DeWald, MD<br />
Cover Story<br />
Dr. DeWald <strong>at</strong>tended <strong>Rush</strong> Medical College<br />
in Chicago. He completed a residency <strong>at</strong> the<br />
Orthopaedic Excellence
Cover Story<br />
University of Illinois Hospital and Clinics<br />
and <strong>at</strong> Shriners Hospital for Crippled<br />
Children, both in Chicago. He then<br />
completed his training with a fellowship<br />
<strong>at</strong> <strong>Rush</strong> University Medical Center, also<br />
in Chicago, and <strong>at</strong> Shriners Hospital for<br />
Crippled Children.<br />
Since joining MOR, Dr. DeWald and his<br />
staff continue their focus on research and<br />
corrective surgery of spinal deformities,<br />
including scoliosis, kyphosis, and spondylolisthesis.<br />
Dr. DeWald says he is very interested<br />
in research on disorders of the spine,<br />
particularly adult and pedi<strong>at</strong>ric scoliosis.<br />
About K.W. Hammerberg, MD<br />
For the past 22 years, Dr. Hammerberg has<br />
devoted his time and expertise to Shriners<br />
Hospital for Crippled Children as the Chief<br />
Spine Surgeon. Dr. Hammerberg and his<br />
medical team specialize in a nonfusion surgical<br />
technique for pedi<strong>at</strong>ric spinal deformities.<br />
A cum laude gradu<strong>at</strong>e from Yale University<br />
in New Haven, Connecticut, Dr. Hammerberg<br />
completed his medical degree <strong>at</strong><br />
the University of Illinois, Abraham Lincoln<br />
Orthopaedic Excellence<br />
School of Medicine in Chicago in 1977. He<br />
completed a residency and an internship<br />
<strong>at</strong> <strong>Rush</strong> University Medical Center and a<br />
spine fellowship <strong>at</strong> <strong>Rush</strong> — the University<br />
of Illinois and <strong>at</strong> Shriners Hospital for<br />
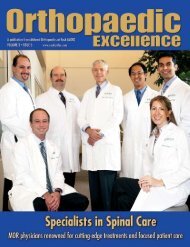
(left to right) K.W. Hammerberg, MD, Jeffrey Mjaanes, MD, Monica Kogan, MD, and Christopher DeWald, MD<br />
Crippled Children. MOR is fortun<strong>at</strong>e to<br />
have a physician with his experience and<br />
expertise on its medical team.<br />
Drs. DeWald and Hammerberg have an excellent<br />
clinical staff th<strong>at</strong> is part of the MOR<br />
team, including Mary Faut Rodts, MS, MSA,<br />
CNP, ONC, FAAN, and Dorothy Pietrowski,<br />
RN, BSN, ONC. The physicians and their<br />
clinical team play a vital role in the pedi<strong>at</strong>ric<br />
orthopaedic subspecialty and for MOR in<br />
the tre<strong>at</strong>ment of spinal deformities, using<br />
the l<strong>at</strong>est techniques in nonoper<strong>at</strong>ive and<br />
advanced surgical approaches. For example,<br />
they use bracing and nonfusion scoliosis<br />
surgery as a conserv<strong>at</strong>ive tre<strong>at</strong>ment for both<br />
pedi<strong>at</strong>ric and adolescent spinal deformity.<br />
The addition of these highly trained, talented<br />
subspecialty physicians and their services<br />
to MOR’s Pedi<strong>at</strong>ric Program helps further<br />
MOR’s mission to provide the best, most<br />
comprehensive, and convenient list of<br />
orthopaedic services to its p<strong>at</strong>ients.<br />
Paul Strandquist, Director of Marketing<br />
<strong>at</strong> <strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong> (MOR),<br />
has been in customer service and marketing<br />
with MOR for 20 years. He enjoys<br />
coaching baseball and is currently the<br />
President of the St. Laurence High School<br />
F<strong>at</strong>her’s Club in Burbank, Illinois.<br />
(left to right) Christopher DeWald, MD, Jeffrey Mjaanes, MD, Monica Kogan, MD, and K.W. Hammerberg, MD
Orthopaedic Excellence
Sports Medicine<br />
Twisting and Turning<br />
Ankle sprains are the most common<br />
sports injury<br />
By Johnny Lin, MD<br />
Ankle sprains are the most common<br />
<strong>at</strong>hletic injury, with more than 27,000<br />
sprains reported every day. Th<strong>at</strong><br />
equ<strong>at</strong>es to approxim<strong>at</strong>ely 6% to 10% of all<br />
emergency room visits, costing more than<br />
$3.65 billion per year.<br />
Ankle sprains are caused by injuring the<br />
ligament th<strong>at</strong> stabilizes the ankle. They can<br />
happen during sports, but they also can occur<br />
when people land wrong on an uneven<br />
surface, such as a curb. The fibers in the<br />
ankle ligaments are able to stretch; however,<br />
severe sprains can actually cause the ligaments<br />
to tear. Some people report hearing<br />
a pop when the injury occurs, and the pain<br />
can be delayed or immedi<strong>at</strong>e.<br />
10 Orthopaedic Excellence<br />
Diagnosis<br />
Symptoms of an ankle sprain include pain<br />
and swelling. The grade of a sprain is<br />
determined by the force of the injury. Grade<br />
one injuries cause minimal disability. Putting<br />
weight on the ankle is possible, and swelling<br />
is localized and minimal. The fibers of the<br />
ligament are stretched but not ruptured.<br />
Grade two sprains cause moder<strong>at</strong>e disability.<br />
Putting weight on the ankle is more difficult,<br />
and swelling is more severe over the area of<br />
injury. Only one of the three ankle ligaments<br />
is completely torn.<br />
The most debilit<strong>at</strong>ing sprains are those classified<br />
as grade three. Many times it is not<br />
possible to put weight on the leg, and severe<br />
swelling is present over the whole<br />
ankle and foot. In these cases,<br />
two or three ligaments<br />
are completely torn.<br />
Noticeable instability<br />
is apparent<br />
when a physician<br />
pushes or rot<strong>at</strong>es<br />
the ankle.<br />
Depending on the<br />
severity of the sprain,<br />
a physician may order<br />
an x-ray or magnetic<br />
resonance imaging (MRI)<br />
scan to determine the grade.<br />
In severe cases, the surface of<br />
the ankle joint is also damaged.<br />
It is important to get medical tre<strong>at</strong>ment<br />
for proper diagnosis because a<br />
broken bone may have similar symptoms as<br />
a grade three sprain.<br />
There are several risk factors for sprained<br />
ankles. Particip<strong>at</strong>ing in sports such as<br />
basketball, soccer, and football increases<br />
the risk. Also, those who suffered a previous<br />
ankle sprain or who are overweight are <strong>at</strong><br />
increased risk of a severe sprain. Perhaps the<br />
worst st<strong>at</strong>istic is th<strong>at</strong> approxim<strong>at</strong>ely 40% of<br />
ankle sprains can lead to chronic problems<br />
if not tre<strong>at</strong>ed correctly.<br />
Tre<strong>at</strong>ment<br />
Proper tre<strong>at</strong>ment should start with PRICE<br />
(protection, rest, ice, compression, and<br />
elev<strong>at</strong>ion). Through this approach, a person<br />
with a grade one sprain should be able to<br />
walk without a limp within a week and<br />
return to normal activities in one to two<br />
weeks. Swelling should be minimal <strong>at</strong> this<br />
point, and in some cases, anti-inflamm<strong>at</strong>ory<br />
medic<strong>at</strong>ions are used to control pain<br />
and swelling. Conversely, if noticeable<br />
improvement is not seen by this time, it is<br />
important to see an orthopaedic foot and<br />
ankle physician who can check for a more<br />
serious injury.<br />
If no other serious injury is present, the physician<br />
may recommend muscle-strengthening<br />
and range-of-motion exercises, followed<br />
by activity-specific rehabilit<strong>at</strong>ion training,<br />
which allows for a faster and safer recovery<br />
and has been shown to minimize chances<br />
for reinjury.<br />
Rehabilit<strong>at</strong>ion may include electric stimul<strong>at</strong>ion<br />
to ease pain and swelling and/or<br />
w<strong>at</strong>er exercises, which can be a less painful<br />
altern<strong>at</strong>ive. Rehabilit<strong>at</strong>ion typically involves<br />
three phases:<br />
1. Rest and protection (to decrease<br />
swelling)<br />
2. Strengthening and flexing the muscles<br />
and tendons
The Physiology of the Ankle<br />
Classific<strong>at</strong>ion of Ankle Sprains<br />
Severity Physical Exam Impairment P<strong>at</strong>hophysiology Typical<br />
Findings<br />
Tre<strong>at</strong>ment*<br />
Grade 1<br />
Grade 2<br />
Grade<br />
Minimal tenderness<br />
and swelling<br />
Moder<strong>at</strong>e tenderness<br />
and swelling<br />
Significant swelling ,<br />
tenderness, and<br />
instability<br />
Dorsal view of the ankle joint bones showing the calcaneus,<br />
cuneiforms, met<strong>at</strong>arsals, and phalanges<br />
L<strong>at</strong>eral view of the ankle joint bones showing the calcaneus, cuneiforms, met<strong>at</strong>arsals, and phalanges<br />
Minimal<br />
Moder<strong>at</strong>e<br />
Moder<strong>at</strong>e<br />
Severe<br />
Microscopic tearing of<br />
collagen fibers<br />
Complete tears of<br />
some but not all<br />
collagen fibers in the<br />
ligament<br />
Complete tear/<br />
rupture of the<br />
ligament<br />
Weight bearing<br />
as toler<strong>at</strong>ed; no<br />
splinting/casting;<br />
isometric exercises;<br />
and full range-of-<br />
motion and stretching/strengthening<br />
exercises as toler<strong>at</strong>ed<br />
Immobiliz<strong>at</strong>ion<br />
with air splint and<br />
physical therapy with<br />
range-of-motion and<br />
stretching/strengthening<br />
exercises<br />
Immobiliz<strong>at</strong>ion;<br />
physical therapy<br />
similar to th<strong>at</strong> for<br />
Grade 2 sprains but<br />
over a longer period;<br />
and possible surgical<br />
reconstruction<br />
* P<strong>at</strong>ients must receive tre<strong>at</strong>ment th<strong>at</strong> is tailored to their individual needs. This table outlines common tre<strong>at</strong>ment protocols.<br />
RepROduCed WIth peRMISSIOn fROM BeRnSteIn J (ed): MusculoskeleTal Medicine. ROSeMOnt, IL, AMeRICAn ACAdeMy Of ORthOpAedIC SuRGeOnS, 200 , p 2 2.<br />
3. Gradually returning to normal activity<br />
(This process varies significantly depending<br />
on the grade of the injury and can<br />
range from weeks to months.)<br />
Surgery for a sprain is rare, unless the ligament<br />
fails to heal correctly or the p<strong>at</strong>ient has<br />
recurrent sprains due to a “loose ankle.”<br />
Prevention<br />
Recurring sprains or chronic ankle pain can<br />
be easily prevented with rehabilit<strong>at</strong>ion and<br />
proper healing time. It is important th<strong>at</strong> the<br />
ligament heals completely before returning to<br />
activities th<strong>at</strong> may aggrav<strong>at</strong>e the injury.<br />
Risk can be reduced with braces, but be<br />
careful. Ankle braces can increase strain<br />
on the knee joint. Once an ankle has been<br />
sprained, strengthening exercises should<br />
never cease, even if a brace is worn. Quitting<br />
exercises can lead to a recurrence of the<br />
injury, particularly if they are stopped too<br />
early. Abnormal mechanics of the ankle-joint<br />
complex also can be a contributing factor to<br />
ankle sprains, so the use of orthotics may<br />
help prevent injury.<br />
Prevention is up to the individual. Wearing<br />
sensible, proper-fitting shoes is as important<br />
as staying fit enough to keep muscles strong<br />
and supportive. P<strong>at</strong>ients should w<strong>at</strong>ch for<br />
uneven surfaces when exercising and heed<br />
the body’s warning signs if pain or f<strong>at</strong>igue<br />
occurs during physical activity.<br />
Source: orthoinfo.aaos.org<br />
Johnny L. Lin, MD, is a foot<br />
and ankle specialist <strong>at</strong> <strong>Midwest</strong><br />
<strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong>. A medical<br />
gradu<strong>at</strong>e from the University<br />
of Illinois College of Medicine<br />
<strong>at</strong> Rockford, Dr. Lin completed<br />
a residency in orthopaedic surgery <strong>at</strong> <strong>Rush</strong><br />
University Medical Center. His fellowship was<br />
completed <strong>at</strong> the world-renowned University<br />
of Tennessee-Campbell Clinic Department of<br />
Orthopaedic Surgery.<br />
Orthopaedic Excellence<br />
11
Need Kicker<br />
Winter sports leave<br />
knees vulnerable<br />
Staying in<br />
the Game<br />
12<br />
By Jeff Mjaanes, MD, FAAP<br />
Orthopaedic Excellence<br />
Winter has arrived, and so have<br />
winter sports such as basketball,<br />
volleyball, and indoor soccer.<br />
The constant running and jumping associ<strong>at</strong>ed<br />
with these sports are ideal for improving<br />
cardiovascular fitness. However, these<br />
activities can also increase pressure on<br />
structures in the anterior knee, especially<br />
in young <strong>at</strong>hletes.<br />
Chronic anterior knee pain is one of the<br />
most common problems encountered by<br />
primary care physicians. The most likely<br />
causes for anterior knee pain in young<br />
<strong>at</strong>hletes are Osgood-Schl<strong>at</strong>ter disease,<br />
p<strong>at</strong>ellofemoral stress syndrome, and p<strong>at</strong>ellar<br />
tendinop<strong>at</strong>hies. All three conditions<br />
represent overuse injuries to the extensor<br />
mechanism of the knee.<br />
Osgood-Schl<strong>at</strong>ter Disease<br />
Accessory growth pl<strong>at</strong>es, or apophyses,<br />
are sites where tendons <strong>at</strong>tach to bones<br />
in growing children. There are two apophyses<br />
loc<strong>at</strong>ed <strong>at</strong> each end of the p<strong>at</strong>ellar<br />
tendon in the knee. Repe<strong>at</strong>ed quadriceps<br />
contraction, such as th<strong>at</strong> associ<strong>at</strong>ed with<br />
running and jumping, leads to significant<br />
traction <strong>at</strong> these apophyses.<br />
Pain <strong>at</strong> the proximal tendon insertion<br />
on the inferior pole of the p<strong>at</strong>ella occurs<br />
mainly in pre-adolescents and is termed<br />
Sinding-Larsen-Johansson disease. In<br />
Osgood-Schl<strong>at</strong>ter disease, adolescent<br />
<strong>at</strong>hletes present with pain and swelling<br />
<strong>at</strong> the tibial tuberosity.<br />
In both conditions, physical exam findings<br />
of point tenderness and/or swelling <strong>at</strong> the<br />
respective apophysis are usually sufficient<br />
to make the diagnosis. If l<strong>at</strong>eral x-rays are<br />
obtained, fragment<strong>at</strong>ion of the apophysis
with mild swelling in the overlying soft<br />
tissue is typical. L<strong>at</strong>eral imaging is imper<strong>at</strong>ive<br />
to rule out an avulsion fracture if the<br />
p<strong>at</strong>ient has sudden, severe pain <strong>at</strong> the<br />
apophysis and gait disturbance.<br />
P<strong>at</strong>ellofemoral Stress Syndrome<br />
Anterior knee pain origin<strong>at</strong>ing from increased<br />
pressure between the p<strong>at</strong>ella and the femoral<br />
condyles is known as p<strong>at</strong>ellofemoral stress<br />
(pain) syndrome (PFSS). P<strong>at</strong>ients present<br />
with insidious onset of dull, achy perip<strong>at</strong>ellar<br />
or retrop<strong>at</strong>ellar pain th<strong>at</strong> increases when<br />
negoti<strong>at</strong>ing stairs or sitting for prolonged<br />
periods (“the<strong>at</strong>er sign”). P<strong>at</strong>ellar tracking<br />
problems and quadriceps weakness are major<br />
risk factors for PFSS, which affects more<br />
females than males.<br />
During physical examin<strong>at</strong>ion, quadriceps<br />
<strong>at</strong>rophy or asymmetry and p<strong>at</strong>ellar hypermobility<br />
can be observed. Compression of the<br />
p<strong>at</strong>ella often produces pain (“positive grind<br />
test”), as does isometric quadriceps contraction.<br />
Tilting the p<strong>at</strong>ella and palp<strong>at</strong>ing the<br />
facets (articular surfaces) under the medial<br />
and l<strong>at</strong>eral edges commonly elicit pain in<br />
PFSS sufferers.<br />
P<strong>at</strong>ellar Tendinosis<br />
Adolescent <strong>at</strong>hletes in jumping sports,<br />
such as basketball or volleyball, who present<br />
with chronic pain below the kneecap,<br />
often have p<strong>at</strong>ellar tendinosis, or “jumper’s<br />
knee.” Examin<strong>at</strong>ion elicits point tenderness<br />
on the body of the tendon itself<br />
or, more commonly, <strong>at</strong> the inferior pole<br />
of the p<strong>at</strong>ella (similar to Sinding-Larsen-<br />
Johansson disease). Occasionally, p<strong>at</strong>ients<br />
experience tenderness <strong>at</strong> the superior<br />
pole of the p<strong>at</strong>ella, indic<strong>at</strong>ive of quadriceps<br />
tendonitis.<br />
Disease Management<br />
Management of Osgood-Schl<strong>at</strong>ter disease,<br />
PFSS, and p<strong>at</strong>ellar tendonitis involves controlling<br />
pain and correcting biomechanical<br />
defects in knee extension. Activity<br />
modific<strong>at</strong>ion along with rest, ice, compression<br />
(such as an ACE ® bandage wrap or<br />
open-p<strong>at</strong>ella neoprene knee sleeve), and<br />
elev<strong>at</strong>ion (“RICE”) are useful for controlling<br />
symptoms, as are nonsteroidal antiinflamm<strong>at</strong>ory<br />
medic<strong>at</strong>ions.<br />
Therapeutic exercises to strengthen the<br />
quadriceps muscle, particularly the medial<br />
component (the vastus medialis oblique),<br />
and to stretch the hamstring and calf muscles<br />
work to improve p<strong>at</strong>ellar tracking and<br />
decrease pain over time. In elite <strong>at</strong>hletes,<br />
The Physiology of the Knee<br />
Quadriceps<br />
(thigh muscle)<br />
P<strong>at</strong>ella<br />
(kneecap)<br />
P<strong>at</strong>ellar<br />
Tendon<br />
Tibial<br />
Tuberosity<br />
Tibia<br />
(shinbone)<br />
a formal physical therapy consult<strong>at</strong>ion is<br />
often helpful to reinforce strengthening<br />
and stretching exercises, to use modalities<br />
such as electrical stimul<strong>at</strong>ion, and to<br />
perform a gait analysis for detecting and<br />
correcting other predisposing biomechanical<br />
factors.<br />
There are key points to ensuring th<strong>at</strong><br />
p<strong>at</strong>ients receive proper care. Keep in mind<br />
th<strong>at</strong> any young p<strong>at</strong>ient with knee pain but<br />
a normal knee exam requires a detailed<br />
evalu<strong>at</strong>ion of the hip joint, including internal<br />
rot<strong>at</strong>ion, to rule out a referred source<br />
of pain. Also, any <strong>at</strong>hlete with more than<br />
four weeks of knee pain or recurrent joint<br />
swelling should have x-rays performed<br />
(five views, including l<strong>at</strong>eral, sunrise,<br />
bil<strong>at</strong>eral anteroposterior, bil<strong>at</strong>eral skier’s,<br />
Quadriceps<br />
(thigh muscle)<br />
P<strong>at</strong>ella<br />
(kneecap)<br />
P<strong>at</strong>ellar<br />
Tendon<br />
Tibial<br />
Tuberosity<br />
Tibia<br />
(shinbone)<br />
Anterior View Medial View<br />
Sports Medicine<br />
Orthopaedic Excellence<br />
1
Sports Medicine<br />
and tunnel) to rule out growth pl<strong>at</strong>e<br />
disturbances, osteochondral lesions, or<br />
p<strong>at</strong>ellar abnormalities.<br />
Lastly, physicians should be aware th<strong>at</strong> other<br />
entities, such as p<strong>at</strong>ellar sublux<strong>at</strong>ion/disloc<strong>at</strong>ion<br />
and synovial impingement, commonly<br />
lead to chronic anterior knee pain. Therefore,<br />
Any <strong>at</strong>hlete with more<br />
than four weeks of<br />
knee pain or recurrent<br />
joint swelling should<br />
have x-rays performed<br />
to rule out growth<br />
pl<strong>at</strong>e disturbances,<br />
osteochondral lesions, or<br />
p<strong>at</strong>ellar abnormalities.<br />
any p<strong>at</strong>ient who is not improving with conserv<strong>at</strong>ive<br />
tre<strong>at</strong>ment should be referred to a<br />
primary care or orthopaedic sports medicine<br />
specialist for further management.<br />
Jeffrey M. Mjaanes, MD, is<br />
a medical gradu<strong>at</strong>e from the<br />
University of Wisconsin School<br />
of Medicine in Madison. Dr.<br />
Mjaanes completed a residency<br />
in pedi<strong>at</strong>rics <strong>at</strong> <strong>Rush</strong> University<br />
Medical Center. During the residency, he<br />
was awarded the Aesculapius Award for his<br />
work in resident teaching and p<strong>at</strong>ient care. Dr.<br />
Mjaanes is Assistant Professor of Pedi<strong>at</strong>rics <strong>at</strong><br />
<strong>Rush</strong> University Medical Center. Through his<br />
affili<strong>at</strong>ion with <strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong>,<br />
he looks to advance his research in pedi<strong>at</strong>ric<br />
sports medicine, including studies on anterior<br />
knee pain in children and throwing injuries in<br />
young <strong>at</strong>hletes.<br />
Bibliography<br />
LaBella, C. p<strong>at</strong>ellofemoral pain syndrome: evalu<strong>at</strong>ion and<br />
tre<strong>at</strong>ment. Primary care clinics in office Practice. 200 ;Vol 1.<br />
Shea, K, et al. Idiop<strong>at</strong>hic anterior knee pain in adolescents.<br />
orthop clin north am. 200 ; Vol .<br />
Smith, A, tao, S. Knee Injuries in young Athletes. clin sports<br />
Med. 1 ;Vol 1 , no .<br />
1 Orthopaedic Excellence
Orthopaedic Excellence<br />
1
Sports Medicine<br />
Reality Check for<br />
Young Athletes<br />
Long-term effects of overuse injuries<br />
are a serious concern<br />
By Dennis Viellieu<br />
Over a year ago, <strong>Midwest</strong> <strong>Orthopaedics</strong><br />
<strong>at</strong> <strong>Rush</strong> (MOR) decided to<br />
experiment with promoting sports<br />
safety in a vulnerable popul<strong>at</strong>ion — children.<br />
This decision was precipit<strong>at</strong>ed by the continuing<br />
trend for <strong>at</strong>hletes to select a sport of<br />
choice <strong>at</strong> younger and younger ages. They<br />
compete, train, and particip<strong>at</strong>e in these sports<br />
year-round, increasing the probability of overuse<br />
injuries and the chance for sustaining an<br />
injury th<strong>at</strong> will affect them for a lifetime.<br />
MOR started a program to provide children<br />
and their coaches with sports safety<br />
Tammy Sciortino (far right) teaches sports safety to <strong>at</strong>hletes<br />
and their coaches with the goal of reducing overuse injuries<br />
through MOR’s <strong>at</strong>hletic training outreach program.<br />
1 Orthopaedic Excellence<br />
inform<strong>at</strong>ion, clinical coverage for tournaments<br />
and games, and medical advice<br />
or tre<strong>at</strong>ment.<br />
To lead the effort, MOR<br />
turned to Tammy Sciortino,<br />
an experienced <strong>at</strong>hletic<br />
trainer familiar with young<br />
<strong>at</strong>hletes in year-round<br />
programs. Before coming to<br />
MOR, Sciortino was the president and CEO<br />
of her own sports performance company,<br />
Sports Sciorts. In addition, she had <strong>at</strong>hletic<br />
training, strength training, and massage experience<br />
working with organiz<strong>at</strong>ions<br />
like the Chicago Fire Soccer Team,<br />
AVP Pro Beach Volleyball Tour, and<br />
Illinois Gymnastics Institute.<br />
Working with physical and <strong>at</strong>hletic<br />
training company partners of MOR,<br />
Sciortino had the program up and<br />
running quickly. In one year, there<br />
are more than 7,000 <strong>at</strong>hletes particip<strong>at</strong>ing<br />
in clubs affili<strong>at</strong>ed with the<br />
MOR outreach program.<br />
Sciortino and MOR offer sports safety<br />
classes and seminars to help make<br />
coaches and trainers aware of overuse<br />
injuries as well as other safety concerns.<br />
MOR also plans to offer first<br />
aid and CPR programs to the clubs<br />
to ensure th<strong>at</strong> coaches and trainers<br />
are prepared for medical issues th<strong>at</strong><br />
might arise.<br />
The Truth Hurts<br />
According to SAfe KIdS uSA:<br />
· More than . million children ages 1 and<br />
under receive medical tre<strong>at</strong>ment for sports<br />
injuries each year.<br />
· Injuries associ<strong>at</strong>ed with particip<strong>at</strong>ion in<br />
sports and recre<strong>at</strong>ional activities account for<br />
21% of all traum<strong>at</strong>ic brain injuries among<br />
children in the united St<strong>at</strong>es.<br />
· Overuse injuries, which occur over time from<br />
repe<strong>at</strong>ed motion, are responsible for nearly<br />
half of all sports injuries to middle- and<br />
high-school students. Imm<strong>at</strong>ure bones,<br />
insufficient rest after an injury, and poor<br />
training or conditioning contribute to overuse<br />
injuries among children.<br />
· Most organized sports-rel<strong>at</strong>ed injuries ( 2%)<br />
occur during practices r<strong>at</strong>her than games.<br />
despite this fact, a third of parents often<br />
do not take the same safety precautions<br />
during their child’s practices as they would<br />
for a game.<br />
· A recent survey found th<strong>at</strong> among <strong>at</strong>hletes<br />
ages to 1 , 1 % of basketball players, 2 %<br />
of football players, 22% of soccer players,<br />
2 % of baseball players, and 12% percent<br />
of softball players have been injured while<br />
playing their respective sports.<br />
source: sportssafety.org<br />
In 2007, Sciortino and MOR plan to roll<br />
out a sports safety program th<strong>at</strong> is being<br />
developed in-house with the various sports<br />
medicine physicians. Anyone interested<br />
in either of these programs should call<br />
Sciortino directly <strong>at</strong> (708) 236-2624 (office)<br />
or (630) 272-2501 (cell).<br />
Dennis Viellieu is Chief Executive Officer of<br />
<strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong> and has served<br />
in this position for five years. He enjoys golf,<br />
basketball, and mountain biking.
Orthopaedic Excellence<br />
1
1 Orthopaedic Excellence
The Salvino Investment Team<br />
Customized Portfolio Management<br />
for Individual Investors<br />
Serving doctors and their unique investment<br />
and retirement planning needs<br />
John Salvino<br />
312.364.5360<br />
jsalvino@williamblair.com<br />
Investment Banking Asset Management Equity Research Institutional & Priv<strong>at</strong>e Brokerage Priv<strong>at</strong>e Capital<br />
William Blair & Company, L.L.C. 222 West Adams Street Chicago, Illinois 60606 800.621.0687 www.williamblair.com<br />
CHICAGO HARTFORD LONDON SAN FRANCISCO TOKYO VADUZ ZURICH<br />
Orthopaedic Excellence<br />
1
Need Kicker<br />
Making Strides<br />
Controversy surrounds<br />
the tre<strong>at</strong>ment of<br />
idiop<strong>at</strong>hic toe walking<br />
By Monica Kogan, MD<br />
When children begin walking, a<br />
toe-to-toe gait p<strong>at</strong>tern is considered<br />
part of normal gait develop-<br />
ment. However, a toe-walking gait p<strong>at</strong>tern<br />
th<strong>at</strong> persists past the age of 2 is considered<br />
abnormal, depending on gait velocity 11 .<br />
There are many causes for persistent toe<br />
walking in children, including cerebral palsy,<br />
congenital contractures of the Achilles<br />
tendon, muscular dystrophy, and idiop<strong>at</strong>hic<br />
toe walking (ITW).<br />
Diagnosis<br />
The diagnosis of ITW is one of exclusion<br />
and can be challenging. For example,<br />
children with ITW typically walk on their<br />
toes but are able to fl<strong>at</strong>ten their foot on<br />
request or when concentr<strong>at</strong>ing on their<br />
gait. It may be especially difficult to distinguish<br />
ITW from children with mild spastic<br />
diplegia 7-10 . Children with cerebral palsy<br />
begin walking <strong>at</strong> a l<strong>at</strong>er age, and children<br />
with ITW begin to walk <strong>at</strong> the appropri<strong>at</strong>e<br />
time, 18 months.<br />
The etiology of ITW is not known. Some<br />
authors have suggested th<strong>at</strong> ITW p<strong>at</strong>ients<br />
20 Orthopaedic Excellence<br />
have congenitally short tendo Achilles 6 . Others<br />
have divided p<strong>at</strong>ients into habitual toe<br />
walkers or those with short tendo Achilles 4 .<br />
If left untre<strong>at</strong>ed, the n<strong>at</strong>ural progression of<br />
persistent toe walking places children <strong>at</strong> risk<br />
for falling 2 , developing limit<strong>at</strong>ions in ankle<br />
mobility, and structural abnormalities, such<br />
as persistent outward tibial torsion 3 .<br />
Tre<strong>at</strong>ment<br />
Much controversy exists around the tre<strong>at</strong>ment<br />
of ITW. The goal of any tre<strong>at</strong>ment is to<br />
provide normal function, but also important<br />
is limiting the impact on the child and family.<br />
Heel cord lengthening (either open or<br />
closed), serial casting, and stretching and<br />
physical therapy are tre<strong>at</strong>ment options.<br />
Nonsurgical Solutions<br />
Nonoper<strong>at</strong>ive management, such as serial<br />
casting to stretch the plantar flexors, is<br />
believed by some to be the optimal initial<br />
tre<strong>at</strong>ment 13 . Each week, the child goes to the<br />
physical therapist to have the ankle stretched<br />
and a new cast applied. This process goes<br />
on six weeks or longer.<br />
Brower et. al. 1 showed th<strong>at</strong> children with<br />
ITW along with cerebral palsy who toe walk<br />
and were tre<strong>at</strong>ed with serial casting showed<br />
improvement in dorsiflexion and toe walking.<br />
Griffin et. al. 5 performed a gait analysis<br />
comparing ITW with heel-toe walkers before<br />
and after serial casting; the analysis showed<br />
th<strong>at</strong> serial casting increased the range of<br />
dorsiflexion and also changed the muscle<br />
synergy p<strong>at</strong>tern from abnormal to normal.<br />
Tachdian 13 suggested passive stretching of<br />
the heel cords, gait training, and below-knee<br />
walking casts as the initial tre<strong>at</strong>ment of ITW,<br />
with surgery being reserved for p<strong>at</strong>ients more<br />
than 8 years of age who have failed to respond<br />
to nonoper<strong>at</strong>ive tre<strong>at</strong>ment. Stretching<br />
without casting is an option where the child<br />
undergoes weekly stretching by a physical<br />
therapist, followed by gait training.<br />
Surgical Solutions<br />
The reported failure r<strong>at</strong>e of nonoper<strong>at</strong>ive<br />
tre<strong>at</strong>ment is significant, leading to the<br />
recommend<strong>at</strong>ion by others th<strong>at</strong> surgical<br />
intervention be the primary tre<strong>at</strong>ment. Proponents<br />
argue th<strong>at</strong> oper<strong>at</strong>ive management
of either an open or percutaneous Achilles<br />
lengthening produces more consistent<br />
outcomes, with improved ankle dorsiflexion<br />
and gre<strong>at</strong>er parental s<strong>at</strong>isfaction 11 .<br />
Stricker and Angulo 12 showed th<strong>at</strong> children<br />
tre<strong>at</strong>ed initially with surgical intervention<br />
had better results with respect to restor<strong>at</strong>ion<br />
of ankle dorsiflexion and parental<br />
s<strong>at</strong>isfaction, and th<strong>at</strong> cast and brace tre<strong>at</strong>ment<br />
offered little long-term improvement<br />
compared with untre<strong>at</strong>ed ITW. Hall et. al. 6<br />
performed tendo Achilles lengthenings on<br />
a group of p<strong>at</strong>ients who showed no improvement<br />
after six months to two years<br />
of observ<strong>at</strong>ion. They showed th<strong>at</strong>, when<br />
tre<strong>at</strong>ed surgically, the children exhibited<br />
normal passive and active dorsiflexion<br />
with a heel-toe gait p<strong>at</strong>tern, except for<br />
occasional toe walking in older children.<br />
Both percutaneous and open techniques<br />
have been used for tendo Achilles lengthening.<br />
P<strong>at</strong>ients are placed in below-the-knee<br />
weightbearing casts for four weeks and are<br />
allowed to bear weight immedi<strong>at</strong>ely. During<br />
the four-week period, they particip<strong>at</strong>e in<br />
physical therapy for gait training. Since they<br />
have likely toe walked since ambul<strong>at</strong>ion<br />
began, p<strong>at</strong>ients need to be retrained to walk.<br />
Physical therapy should continue after the<br />
casts are removed, and it is beneficial th<strong>at</strong><br />
Bibliography<br />
1. Brouwer B, davidson LK, Olney SJ. Serial casting in idiop<strong>at</strong>hic<br />
toe-walkers and children with spastic cerebral palsy.<br />
J Pedi<strong>at</strong>r orthop 2000;20:221- .<br />
2. Caselli MA, Rzonca eC, Lue By. habitual toe walking: evalu<strong>at</strong>ion<br />
and approach to tre<strong>at</strong>ment. clin Podi<strong>at</strong>r Med surg<br />
1 ; : - .<br />
. deLuca pA. the musculoskeletal management of children<br />
with cerebral palsy. Pedi<strong>at</strong>r clin north am 1 ; :11 - 0.<br />
. furrer f, deonna t. persistent toe walking in children:<br />
a comprehensive clinical study of 2 cases. Helv Paedi<strong>at</strong>r<br />
acta 1 2; : 01-1 .<br />
. Griffin p, Wheelhouse W, Shiavi R, Bass W. habitual<br />
younger children go to a center th<strong>at</strong> has<br />
pedi<strong>at</strong>ric physical therapists.<br />
Conclusion<br />
ITW is a problem th<strong>at</strong> is seen quite often.<br />
Both oper<strong>at</strong>ive and nonoper<strong>at</strong>ive methods<br />
of tre<strong>at</strong>ment have been recommended,<br />
and each has its pros and cons. Serial<br />
casting is a lengthy process with the child<br />
<strong>at</strong>tending physical therapy once a week<br />
If left untre<strong>at</strong>ed, persistent toe walking can lead<br />
to structural limit<strong>at</strong>ions and abnormalities in the<br />
hips, knees, ankles, and feet. To achieve similar<br />
force and movement levels as those required<br />
during heel-toe walking, toe walkers require<br />
gre<strong>at</strong>er activ<strong>at</strong>ion of less commonly used muscles,<br />
weakening the quadriceps and other muscles and<br />
thre<strong>at</strong>ening joint stability.<br />
toe walkers: a clinical and electromyographic gait analysis. J<br />
Bone Joint surg [Am] 1 ; : -101.<br />
. hall Je, Salter RB, Bhalla SK. Congenital short tendo<br />
calcaneus. J Bone Joint surg [Br] 1 ; : - .<br />
. hicks R, durinick n, Gage JR. differenti<strong>at</strong>ion of<br />
idiop<strong>at</strong>hic toe walking and cerebral palsy. J Pedi<strong>at</strong>r orthop<br />
1 ; :1 0- .<br />
. K<strong>at</strong>z MM, Mubarak SJ. hereditary tendo Achilles contractures.<br />
J Pedi<strong>at</strong>r orthop 1 ; : 11- .<br />
. Rose J, Martin J, torburn L, et al. electromyographic differenti<strong>at</strong>ion<br />
of diplegic cerebral palsy from idiop<strong>at</strong>hic toe<br />
walking: involuntary coactiv<strong>at</strong>ion of the quadriceps and<br />
Diagnostics and Tre<strong>at</strong>ment<br />
for <strong>at</strong> least six weeks, followed by physical<br />
therapy after cast removal. This can be<br />
time consuming for both the p<strong>at</strong>ient and<br />
the parent or caregiver.<br />
Surgery as the initial tre<strong>at</strong>ment may be<br />
seen by some as aggressive, but the results<br />
have been more consistent. Often, parents<br />
or caregivers will try nonoper<strong>at</strong>ive measures<br />
first and opt for surgical intervention<br />
if no improvement is seen. Studies show<br />
th<strong>at</strong> most often children end up requiring<br />
surgery. However, no damage is done<br />
by trying physical therapy first. If nothing<br />
else, parents or caregivers feel secure<br />
knowing th<strong>at</strong> all options were exhausted<br />
before opting for surgery.<br />
Monica Kogan, MD, specializes<br />
in pedi<strong>at</strong>ric orthopaedics<br />
<strong>at</strong> <strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong><br />
<strong>Rush</strong>. A medical gradu<strong>at</strong>e from<br />
the University of Illinois College<br />
of Medicine in Chicago, Dr.<br />
Kogan completed a residency in orthopaedic<br />
surgery <strong>at</strong> Northwestern Memorial Hospital.<br />
A fellowship in pedi<strong>at</strong>ric orthopaedic surgery<br />
was completed <strong>at</strong> the Primary Children’s Medical<br />
Center in Salt Lake City, Utah, a renowned<br />
pedi<strong>at</strong>ric center serving five st<strong>at</strong>es in the<br />
intermountain region.<br />
gastrocnemius. J Pedi<strong>at</strong>r orthop 1 ;1 : - 2.<br />
10. Sala dA, Shulman Lh, Kennedy Rf, et al. Idiop<strong>at</strong>hic toe<br />
walking: a review. dev Med child neuro 1 ; 1: - .<br />
11. St<strong>at</strong>ham L, Murray Mp. early walking p<strong>at</strong>terns of normal<br />
children. clin orthop 1 1; : -2 .<br />
12. Stricker SJ, Angulo JC. Idiop<strong>at</strong>hic toe walking:<br />
a comparison of tre<strong>at</strong>ment methods.<br />
J Pedi<strong>at</strong>r orthop 1 ;1 :2 - .<br />
1 . tachdjian MO. the foot and leg. In: tachdjian MO,<br />
ed. Pedi<strong>at</strong>ric orthopaedics, vol. 2. philadelphia: Saunders:<br />
1 2:1 - 0.<br />
Orthopaedic Excellence<br />
21
22 Orthopaedic Excellence
Orthopaedic Excellence<br />
2
Diagnostics and Tre<strong>at</strong>ment<br />
ITW Defined<br />
distinctive characteristics help pinpoint<br />
tiptoe gait<br />
By Tina Chase, MPT, PCS<br />
Idiop<strong>at</strong>hic toe walking (ITW) is characterized<br />
by a bil<strong>at</strong>eral tiptoe gait th<strong>at</strong><br />
origin<strong>at</strong>es within several months of<br />
independent ambul<strong>at</strong>ion. In normal development,<br />
a m<strong>at</strong>ure heel-toe gait p<strong>at</strong>tern emerges<br />
and is consistent by 2 years of age. Before<br />
th<strong>at</strong>, intermittent toe walking can occur and<br />
progress to a m<strong>at</strong>ure gait p<strong>at</strong>tern.<br />
For some of these children, however, toe<br />
walking persists without history of prem<strong>at</strong>urity,<br />
difficult delivery, evidence of hypertonicity,<br />
or abnormal reflexes. Standing<br />
and walking on tiptoes throughout toddler<br />
and school-aged years continues despite<br />
rel<strong>at</strong>ively normal development and <strong>at</strong>tainment<br />
of advanced gross motor skills, such<br />
as running and skipping.<br />
Distinguishing Fe<strong>at</strong>ures and Diagnoses<br />
When diagnosing ITW, mild spastic diplegia<br />
cerebral palsy (CP) is considered in<br />
the differential diagnosis. In addition to the<br />
neurological exam, family history, range of<br />
motion (ROM), and gait p<strong>at</strong>tern assist in<br />
confirming ITW.<br />
Unlike CP, ITW is an autosomal dominant<br />
trait. Approxim<strong>at</strong>ely 40% of those affected<br />
by ITW have a family history of tiptoe gait.<br />
Also differing is passive ankle dorsiflexion<br />
ROM with the knee extended, which typically<br />
averages more than 5 degrees in ITW<br />
versus less than 5 degrees with mild CP.<br />
The gait p<strong>at</strong>tern of the two is also slightly<br />
different. In ITW, the knees typically remain<br />
flexed throughout the gait cycle and the feet<br />
2 Orthopaedic Excellence<br />
plantarflexed throughout most of the swing<br />
phase. In CP, the knees flex <strong>at</strong> initial contact,<br />
have no loading response, and extend<br />
through mid or l<strong>at</strong>e stance. The feet dorsiflex<br />
during the swing phase.<br />
L<strong>at</strong>e-onset toe walking implies a well-<br />
established period of heel-toe gait followed<br />
by the emergence of toe walking. This progression<br />
is not characteristic of ITW, and<br />
Serial casting can be an effective technique for<br />
gaining stretch in the Achilles tendon. A belowthe-knee<br />
plaster or fiberglass cast is applied/<br />
changed weekly to progressively increase the<br />
range of dorsiflexion.<br />
neuromuscular abnormality — including<br />
spinal cord anomalies, peripheral neurop<strong>at</strong>hies,<br />
and muscular dystrophies — should<br />
be considered.<br />
The Importance of Range of Motion<br />
Kinem<strong>at</strong>ic studies show th<strong>at</strong> approxim<strong>at</strong>ely<br />
10 degrees of ankle dorsiflexion occurs during<br />
normal gait. A heel-toe gait p<strong>at</strong>tern is<br />
achievable, however, with as little as 0 degrees<br />
of dorsiflexion. Because most ITW p<strong>at</strong>ients<br />
have <strong>at</strong> least 0 degrees of dorsiflexion, they<br />
may stand and walk normally on command.<br />
In deciding the course and effectiveness of<br />
tre<strong>at</strong>ment, the degree of active and passive<br />
dorsiflexion ROM should be considered. If<br />
a child has <strong>at</strong> least 10 degrees of active dorsiflexion<br />
with the knee extended, then focus<br />
can be placed on strengthening the dorsiflexors<br />
and the timing of their activ<strong>at</strong>ion during<br />
gait. If there is significant dynamic tone in<br />
the gastrocnemius and/or soleus muscles,<br />
the Tardieu Scale measures of resistance 1<br />
(R1) and resistance 2 (R2) can be used.<br />
R1 refers to the initial end range or dynamic<br />
range of the muscle. It is the first resistance,<br />
or “first c<strong>at</strong>ch,” appreci<strong>at</strong>ed when<br />
the ankle is quickly, passively dorsiflexed.<br />
R2, or “second c<strong>at</strong>ch,” refers to the maximal<br />
end-range length of the muscle, which<br />
is obtained when the muscle is maximally<br />
stretched with continued pressure into the<br />
elong<strong>at</strong>ed position.<br />
For an ITW p<strong>at</strong>ient, R1 is functionally more<br />
relevant than R2 since most will only use the<br />
ROM up to R1 during gait. This is especially<br />
true when the “thickness” of resistance<br />
between R1 and R2 is gre<strong>at</strong>. When this is<br />
the case, a fixed muscle contracture may be<br />
developing, and ROM gains are expected<br />
to be minimal with stretching alone. Better<br />
ROM gains may be obtained with bracing,<br />
casting, or surgery.<br />
Tre<strong>at</strong>ment<br />
Once ITW is diagnosed, a course of tre<strong>at</strong>ment<br />
can be determined. Conserv<strong>at</strong>ive<br />
approaches to tre<strong>at</strong>ing ITW include physical<br />
therapy by a pedi<strong>at</strong>ric physical therapist for<br />
stretching, strengthening, and gait training.<br />
Night and/or daytime bracing in ankle foot<br />
orthoses (AFOs) or serial casting over several<br />
weeks may be prescribed for children whose<br />
ankles do not easily dorsiflex beyond neutral.<br />
Botox injections to weaken the overactive
gastrocnemius or surgical lengthening of the<br />
Achilles tendons by an orthopaedic surgeon<br />
also are successful tre<strong>at</strong>ment interventions<br />
and may appeal to families when conserv<strong>at</strong>ive<br />
measures fail.<br />
Choosing the appropri<strong>at</strong>e course of tre<strong>at</strong>ment<br />
depends on many factors, including:<br />
• Age, <strong>at</strong>tention, and cognitive abilities of<br />
the child<br />
• Ankle dorsiflexion, ROM, and degree of<br />
toe walking<br />
• Importance of speedy and full recovery<br />
Physical Therapy<br />
Physical therapy for ITW can be most effective<br />
when performed by a pedi<strong>at</strong>ric physical<br />
therapist. Walking on challenging surfaces<br />
such as sand, ramps, or a m<strong>at</strong>tress on the<br />
floor can reinforce heel contact and teach<br />
appropri<strong>at</strong>e timing and coactiv<strong>at</strong>ion of the<br />
foot muscul<strong>at</strong>ure. These str<strong>at</strong>egies can be<br />
taught to caregivers for practicing <strong>at</strong> home.<br />
Bracing<br />
AFOs can be worn <strong>at</strong> night to apply a<br />
long-dur<strong>at</strong>ion, low-intensity stretch to the<br />
heel cords or during the day to promote<br />
a heel-toe gait. They have shown better<br />
Idiop<strong>at</strong>hic Toe Walking<br />
Hip: normal kinem<strong>at</strong>ics<br />
Knee: Remains flexed throughout gait cycle<br />
Maximum extension is <strong>at</strong> ground contact with<br />
the knee averaging 11 degrees of flexion<br />
Ankle: Average passive dorsiflexion is more than<br />
degrees (range is less than 10 degrees to more<br />
than 1 degrees)<br />
Ground contact is in plantar flexion<br />
Swing phase: Ankle initially dorsiflexes but then<br />
plantarflexes mid to l<strong>at</strong>e swing<br />
Walking on challenging surfaces such as an<br />
inclined treadmill can help reinforce heel contact<br />
and teach appropri<strong>at</strong>e timing and coactiv<strong>at</strong>ion of<br />
the foot muscul<strong>at</strong>ure.<br />
outcomes in children who do not gain ROM<br />
with stretching or who consistently toe walk<br />
despite exercises. Although many children<br />
return to toe walking once the AFOs are<br />
removed, the braces allow the heels to be<br />
loaded correctly and the postural muscles to<br />
be used in correct alignment.<br />
Casting<br />
Serial casting involves applying short leg<br />
casts to the lower legs and feet to stretch the<br />
gastrocsoleus muscles. It can be indic<strong>at</strong>ed<br />
if conserv<strong>at</strong>ive stretching fails, if bracing is<br />
not well toler<strong>at</strong>ed by the child, or if tightness<br />
prevents bracing. With casting, the ankle<br />
joint is held in an elong<strong>at</strong>ed position for<br />
several weeks vs. several minutes or hours<br />
as with stretching and bracing. Casts are<br />
changed every one to two weeks between<br />
Mild Diplegia<br />
Hip: normal kinem<strong>at</strong>ics<br />
Knee: flexes <strong>at</strong> ground contact, has no loading<br />
response, and extends through mid and l<strong>at</strong>e stance<br />
Maximum extension is <strong>at</strong> mid to l<strong>at</strong>e stance<br />
Ankle: Average passive dorsiflexion is less than<br />
degrees (range is less than 20 degrees to 0 degrees)<br />
Ground contact is in plantar flexion<br />
Swing phase: Ankle dorsiflexes throughout the<br />
entire phase<br />
three and eight times. With each cast, the<br />
ankles are repositioned into a gre<strong>at</strong>er degree<br />
of ankle dorsiflexion until the desired ROM<br />
is obtained. Serial casting can result in large<br />
gains in ROM and improvements in walking<br />
in a short period of time.<br />
Conclusion<br />
Early detection of ITW is important because<br />
prolonged tiptoe gait can lead to adaptive<br />
shortening of the heel cords, weakness and<br />
poor coordin<strong>at</strong>ion in the knee and ankle<br />
muscul<strong>at</strong>ure, and postural changes in the<br />
trunk. Timely referral to an orthopaedic<br />
surgeon and a pedi<strong>at</strong>ric physical therapist<br />
increases the likelihood of successful tre<strong>at</strong>ment<br />
and, in the long run, may be less<br />
costly and time consuming.<br />
Tina Chase, MPT, PCS,<br />
Clinic Director of The Pedi<strong>at</strong>ric<br />
Place in Naperville, Illinois,<br />
is available to speak with<br />
physicians and/or groups who<br />
would like to learn more about<br />
idiop<strong>at</strong>hic toe walking (ITW). She received her<br />
master’s degree in physical therapy from Gannon<br />
University, where she was honored with<br />
the “Outstanding Service in Physical Therapy<br />
Award.” Chase’s professional certific<strong>at</strong>ions<br />
include pedi<strong>at</strong>ric clinical specialist and neurodevelopmental<br />
tre<strong>at</strong>ment for the pedi<strong>at</strong>ric<br />
popul<strong>at</strong>ion. She also specializes in lower<br />
extremity biomechanics/serial casting and<br />
has a particular interest in cerebral palsy and<br />
developmental coordin<strong>at</strong>ion disorder (DCD).<br />
The Pedi<strong>at</strong>ric Place is a Stryker Physiotherapy<br />
Associ<strong>at</strong>es company. Stryker currently<br />
has 18 adult and 12 pedi<strong>at</strong>ric facilities in<br />
the Chicago area. Call (312) 944-7595 to<br />
be connected to Tina in Naperville or any<br />
Illinois facility.<br />
Editor’s Note: Tina Chase is not affili<strong>at</strong>ed<br />
with <strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong>. Tre<strong>at</strong>ment<br />
recommend<strong>at</strong>ions presented in this article are<br />
solely the professional opinion of the author.<br />
Orthopaedic Excellence<br />
2
Technology Insights<br />
Dict<strong>at</strong>ion<br />
Goes Digital<br />
Online pl<strong>at</strong>form makes<br />
cassette tapes obsolete By Victoria Chavez<br />
<strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong> (MOR)<br />
has a long history of working with<br />
various medical transcription (MT)<br />
services, including five independent MTs or<br />
MT services. Physicians have developed very<br />
close working rel<strong>at</strong>ionships with their MTs.<br />
These MTs allow for gre<strong>at</strong> productivity and<br />
efficiency because of their familiarity with<br />
the physician’s dict<strong>at</strong>ion style and use of<br />
medical and technical jargon.<br />
MOR needed a system th<strong>at</strong> would help improve<br />
the workflow of its support staff and<br />
turnaround time from its MT services, but<br />
converting all of the physicians to one new<br />
service where a number of different MTs<br />
are used was not an option. MOR decided<br />
to let all of its physicians keep their current<br />
MTs but to transition to one centralized<br />
2 Orthopaedic Excellence<br />
technology pl<strong>at</strong>form to maximize efficiency<br />
while still preserving the quality of service.<br />
MOR found wh<strong>at</strong> it was looking for in Scribe<br />
Healthcare Technologies, Inc., Lake Forest,<br />
Illinois, a company th<strong>at</strong> came highly recommended.<br />
Scribe offered a centralized system<br />
for all areas of transcription th<strong>at</strong> would<br />
consolid<strong>at</strong>e processes, limit paperwork, and<br />
eventually save time and money. In effect,<br />
MOR went from cassette tapes and daily<br />
courier services in December 2003 to using<br />
digital recording devices for digital transmission<br />
of d<strong>at</strong>a in January 2004.<br />
The flexibility of the Scribe system played<br />
a very important role in transitioning the<br />
physicians to a new system quickly, because<br />
the physicians were able to keep the<br />
quality of their transcription service while<br />
improving all other aspects of processing<br />
dict<strong>at</strong>ions. If this were not the case, MOR<br />
might not be where it is today in terms of<br />
transcription. The company values the rel<strong>at</strong>ionships<br />
it has with its transcription services<br />
and the quality of service they provide.<br />
Executing Change<br />
The implement<strong>at</strong>ion consisted of three<br />
steps to transition to 100% digital via the<br />
Scribe system. First, the MTs were trained<br />
on Scribe and brought up to speed with<br />
hands-on training. This undertaking was<br />
challenging for them because moving to<br />
the new Scribe pl<strong>at</strong>form changed so many<br />
of their processes.<br />
The computer systems of the MTs were<br />
upd<strong>at</strong>ed so th<strong>at</strong> they could support the<br />
Scribe online MT pl<strong>at</strong>form. Many, if not<br />
all, of their computers were outd<strong>at</strong>ed, with<br />
some systems as old as DOS. Scribe provided<br />
training sessions with each of the MT<br />
services and assisted with setting up their<br />
new computers. Once each MT service was<br />
comfortable on the system, they proceeded<br />
to implement<strong>at</strong>ion.<br />
Second, the support staff, management<br />
team, and physicians were trained on<br />
Scribe’s online MD pl<strong>at</strong>form, reworking their<br />
processes to handle dict<strong>at</strong>ion efficiently<br />
on the new pl<strong>at</strong>form. Again, Scribe was<br />
there every step of the way, training MOR’s<br />
practice groups. This step also involved<br />
purchasing digital voice recorders for<br />
all clinicians and physicians, installing<br />
software on all computers<br />
for downloading audio files<br />
from the digital recorders, and<br />
training the staff how<br />
to download.<br />
With technology comes the need for<br />
support. Scribe was very familiar with<br />
typical troubleshooting issues and helped<br />
MOR’s IT staff through the transition.
The last step was training the physicians and<br />
clinicians to use the digital voice recorders.<br />
Although using them was not extremely<br />
different from using old devices th<strong>at</strong> stored<br />
inform<strong>at</strong>ion on tapes, the look and feel of the<br />
new devices was slightly different and inform<strong>at</strong>ion<br />
was stored digitally. The MTs, physicians,<br />
and support staff were now working<br />
on one system divided into two pl<strong>at</strong>forms,<br />
one for the MTs and one for the physicians.<br />
L<strong>at</strong>er, Scribe introduced the administr<strong>at</strong>ive<br />
pl<strong>at</strong>form. This pl<strong>at</strong>form allowed for MOR to<br />
support staff internally, and only on rare occasions<br />
do they need to reach out to Scribe<br />
for technical support. Now th<strong>at</strong> the technical<br />
kinks have been worked out from the implement<strong>at</strong>ion<br />
process and the administr<strong>at</strong>ive<br />
pl<strong>at</strong>form has been introduced, MOR only<br />
needs one IT staff member to support its<br />
Scribe system.<br />
Improved Efficiencies<br />
For many reasons, the decision to use<br />
Scribe’s services has surpassed all expect<strong>at</strong>ions.<br />
MOR no longer has to store or<br />
purchase tapes or rely on a courier service<br />
to deliver dict<strong>at</strong>ions to the proper sources.<br />
Now, MOR has a constant flow of files<br />
going out and completed files coming in.<br />
By elimin<strong>at</strong>ing the middleman, MOR avoids<br />
costly intercepts th<strong>at</strong> can result in the<br />
complete loss of audio<br />
files. With its<br />
new system, MOR rarely loses a file, in<br />
which case it is usually <strong>at</strong>tributed to user<br />
error. In addition, the audio files are stored<br />
on the computer and are tracked on the<br />
Scribe system, substantially increasing the<br />
chances of finding missing inform<strong>at</strong>ion.<br />
MOR staff has quickly become accustomed<br />
to transferring audio files to its MT services<br />
in a m<strong>at</strong>ter of minutes. The audio files<br />
can be transmitted electronically from the<br />
physician to the MT service almost instantaneously.<br />
With courier service and tapes, the<br />
standard turnaround time was two weeks;<br />
now it is anywhere from four to 48 hours.<br />
With a practice th<strong>at</strong> is constantly growing,<br />
space is a priority. Now th<strong>at</strong> its files are<br />
stored electronically, it is not necessary for<br />
MOR to physically store everything in charts<br />
in its medical records department. Scribe’s<br />
pl<strong>at</strong>form is completely Web-based, so critical<br />
p<strong>at</strong>ient inform<strong>at</strong>ion is available <strong>at</strong> all times.<br />
Planning Ahead<br />
Since the transition, Scribe has been flexible<br />
in accommod<strong>at</strong>ing MOR’s needs as a<br />
company. For instance, MOR is taking large<br />
strides toward an electronic medical records<br />
system.<br />
A digital voice recorder stores inform<strong>at</strong>ion on an<br />
online pl<strong>at</strong>form r<strong>at</strong>her than on tapes.<br />
MOR Thanks Its MTs<br />
Without our talented Mts, the transition to<br />
Scribe’s pl<strong>at</strong>form would have been a daunting<br />
challenge. We thank you for all you do and for<br />
your dedic<strong>at</strong>ed service to our company.<br />
– Anne Luginbill, independently contracted<br />
for 1 years<br />
– Ct transcription, 1 years<br />
– Accuscript, years<br />
– Keystrokes transcription Service, Inc., years<br />
– Joyce Garst, independently contracted for<br />
over a year<br />
MOR recently launched a Health Level Seven,<br />
Inc. (HL7) interface th<strong>at</strong> exports p<strong>at</strong>ient identific<strong>at</strong>ion<br />
inform<strong>at</strong>ion from its system applic<strong>at</strong>ion<br />
into the Scribe pl<strong>at</strong>form and imports<br />
p<strong>at</strong>ient clinical notes from Scribe into MOR’s<br />
system. The interface <strong>at</strong>taches all notes back<br />
into the p<strong>at</strong>ient’s chart in MOR’s system.<br />
Scribe has always taken into consider<strong>at</strong>ion<br />
any suggestions or needs of MOR to ensure<br />
the system is working <strong>at</strong> its full potential.<br />
So far, MOR has reduced costs and enhanced<br />
work processes on all fronts, and<br />
the company can report with simplicity<br />
for billing purposes and quality assurance.<br />
This transition was a huge step in the right<br />
direction and has opened the door to endless<br />
possibilities. MOR feels th<strong>at</strong> it is vital to move<br />
forward relentlessly in its pursuit of the l<strong>at</strong>est<br />
technology. The 100% digital transcription<br />
system is a testament to th<strong>at</strong>, and MOR’s<br />
staff looks forward to the changes ahead.<br />
Victoria Chavez received her bachelor’s degree<br />
in inform<strong>at</strong>ion and decision sciences from<br />
the University of Illinois <strong>at</strong> Chicago. She has<br />
been with <strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong> for<br />
five years and currently serves as Inform<strong>at</strong>ion<br />
Systems and Marketing Manager. She enjoys<br />
scrapbooking and traveling.<br />
Orthopaedic Excellence<br />
2
2 Orthopaedic Excellence
Orthopaedic Excellence<br />
2
Need Kicker<br />
Smart<br />
Tools in<br />
Practice<br />
technology allows<br />
physicians to focus on<br />
the p<strong>at</strong>ient<br />
By Lora Freeman, <strong>Midwest</strong> Region<br />
Account Manager, and John Weiss,<br />
Vice President of Sales and Marketing,<br />
Scribe Healthcare Technologies, Inc.<br />
Physicians should spend the majority<br />
of their day delivering quality p<strong>at</strong>ient<br />
care. This is why they have completed<br />
years of study and specializ<strong>at</strong>ion. Most<br />
would probably prefer to focus their time<br />
on improving the quality of life for p<strong>at</strong>ients<br />
r<strong>at</strong>her than dealing with administr<strong>at</strong>ive<br />
issues. The last thing a physician needs<br />
to be inconvenienced by is note dict<strong>at</strong>ion,<br />
including dict<strong>at</strong>ing his or her own notes,<br />
finding transcribed documents, or loc<strong>at</strong>ing<br />
notes from referring physicians.<br />
An Affordable, Convenient Solution<br />
Fortun<strong>at</strong>ely, a new breed of company is<br />
making a difference and enabling physicians<br />
to focus on their number-one priority, the<br />
0 Orthopaedic Excellence<br />
p<strong>at</strong>ient. Companies such as Scribe Healthcare<br />
Technologies, Inc., Lake Forest, Illinois,<br />
and Vianeta Communic<strong>at</strong>ions, Milpitas,<br />
California, offer Web-n<strong>at</strong>ive technologies th<strong>at</strong><br />
are cost-effective to purchase and maintain<br />
compared to other software solutions. These<br />
integr<strong>at</strong>ed Internet technologies work with<br />
the existing hardware and widely used Microsoft<br />
technology th<strong>at</strong> most offices use.<br />
In the short history of transcription technology,<br />
an easy, inexpensive, predictable,<br />
quality product has not always existed. Many<br />
technologies implemented during the last 15<br />
years involved purchasing exorbitantly priced<br />
hardware and/or software or the use of voice-<br />
recognition software th<strong>at</strong> did not provide a<br />
suitable product. While speech recognition<br />
and electronic medical records (EMR) were<br />
once predicted to make transcriptionists<br />
obsolete by the year 2000, the reality is th<strong>at</strong><br />
physicians still dict<strong>at</strong>e, and transcriptionists<br />
still transcribe.<br />
A Personal Touch<br />
There is a bright side. After years of failed<br />
technological implement<strong>at</strong>ions, new<br />
technologies are adapting to the requirements<br />
of the physicians. Technology-based<br />
transcription had to take a close look <strong>at</strong> wh<strong>at</strong><br />
physicians needed, how they did their work,<br />
and wh<strong>at</strong> the end product needed to be.<br />
Both Scribe and Vianeta are companies th<strong>at</strong><br />
have responded to these needs and provided<br />
products th<strong>at</strong> fit easily into a physician’s
existing workflow. In the typical workflow of<br />
a Web-based transcription:<br />
• The physician picks up the phone or handheld<br />
recorder and dict<strong>at</strong>es his or her notes.<br />
• The dict<strong>at</strong>ion is routed to voice-recognition<br />
software or to the medical transcriptionist<br />
(MT). The record is cre<strong>at</strong>ed<br />
in Microsoft Word using the physician’s<br />
preferred form<strong>at</strong>ting and letterhead.<br />
• The document is sent to a physician-<br />
accessed inbox via the Internet. On this<br />
Internet pl<strong>at</strong>form, the physician can edit,<br />
print, fax, e-mail, and store documents<br />
securely. Authorized persons can access<br />
the documents <strong>at</strong> home or in the office.<br />
Back End Support<br />
Wh<strong>at</strong> does a physician need to run these<br />
systems? While many dict<strong>at</strong>ion and transcription<br />
systems cost between tens and<br />
hundreds of thousands of dollars in upfront<br />
expenses, Scribe’s system is Internet-based.<br />
All th<strong>at</strong> is needed is an upd<strong>at</strong>ed PC with<br />
Microsoft Windows and Office programs, a<br />
high-speed Internet connection, and access<br />
to a phone. For a low monthly licensing fee<br />
and a per-line charge for the storage of documents<br />
on Scribe’s pl<strong>at</strong>form, physicians can<br />
use MTs they already work with or choose<br />
from offshore or domestic vendors who type<br />
on the Scribe MT pl<strong>at</strong>form.<br />
Systems like these allow physicians to:<br />
• Perform an advanced search of all documents<br />
on the pl<strong>at</strong>form, meaning they can<br />
search all p<strong>at</strong>ient files by the name of a<br />
drug, diagnosis, or tre<strong>at</strong>ment.<br />
• Listen to all of their audio files, which are<br />
stored electronically.<br />
• Keep an address book of all the referring<br />
physicians with whom they communic<strong>at</strong>e,<br />
which is available online to the MTs.<br />
An Evolving Industry<br />
This new breed of healthcare technology<br />
company has been growing its value proposition.<br />
Scribe has begun to make its move<br />
from dict<strong>at</strong>ion and transcription technology<br />
to offering a complete online repository th<strong>at</strong><br />
looks like an EMR d<strong>at</strong>abase. In 2006, Scribe<br />
announced P<strong>at</strong>ientChart as an “add-on”<br />
module. P<strong>at</strong>ientChart allows a practice to<br />
centralize and store all p<strong>at</strong>ient inform<strong>at</strong>ion,<br />
including transcribed records, images, lab results,<br />
and more. It is flexible, allowing records<br />
to be cre<strong>at</strong>ed through “smart templ<strong>at</strong>es.”<br />
“Scribe focuses on document<strong>at</strong>ion technologies<br />
th<strong>at</strong> complement the way physicians<br />
work. We plan to add a secure communica-<br />
Technology Insights<br />
tion product in 2007 th<strong>at</strong> will allow physicians<br />
to share inform<strong>at</strong>ion with other physicians<br />
or their p<strong>at</strong>ients,” says John Weiss,<br />
Vice President of Sales and Marketing for<br />
Scribe. “As insurance companies begin to<br />
embrace phone and e-mail consult<strong>at</strong>ions,<br />
our new communic<strong>at</strong>ion product will allow<br />
for tracking and reimbursement for these<br />
types of services.”<br />
The University of Chicago Hospitals have<br />
found Scribe’s package to be tremendously<br />
supportive of their dict<strong>at</strong>ion and transcription<br />
process. “The customer service is excellent,”<br />
says Dennis Gray, Assistant Director<br />
of Medical Records <strong>at</strong> University of Chicago<br />
Hospitals. “The training and ownership are<br />
fabulous. They are right in there with the<br />
physicians, training them and helping them<br />
use the system correctly.”<br />
The University of Chicago Hospitals are<br />
implementing an electronic sign<strong>at</strong>ure process,<br />
and Gray says he is looking forward to<br />
experiencing its full benefits soon.<br />
In much the same way th<strong>at</strong> physicians relieve<br />
p<strong>at</strong>ients’ pain and increase their ability<br />
to function in life, technology has evolved<br />
during recent years to ease physicians’ workloads<br />
and improve their ability to function<br />
more efficiently in providing p<strong>at</strong>ient care.<br />
Lora Freeman is the <strong>Midwest</strong> Region Account<br />
Manager for Scribe Healthcare Technologies,<br />
Inc., where <strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong> is<br />
one of her customers. Freeman has been with<br />
Scribe for more than two years. She uses the<br />
dict<strong>at</strong>ion pl<strong>at</strong>form to support her writing when<br />
she cannot access the computer directly.<br />
John Weiss is the Vice President of Sales and<br />
Marketing for Scribe Healthcare Technologies,<br />
Inc. Prior to acquiring Scribe, John was an<br />
early Internet entrepreneur, having founded<br />
several successful dotcoms like Starting Point,<br />
WebPromote, and YesMail. In his free time<br />
John enjoys spending time with family, sailbo<strong>at</strong><br />
racing, and w<strong>at</strong>er skiing.<br />
Orthopaedic Excellence<br />
1
2 Orthopaedic Excellence
<strong>Midwest</strong> <strong>Orthopaedics</strong> <strong>at</strong> <strong>Rush</strong> thanks the following advertisers for helping<br />
make this public<strong>at</strong>ion possible.<br />
Acceler<strong>at</strong>ed Rehabilit<strong>at</strong>ion Centers ... see page 22<br />
AMDC ................................................... see page 18<br />
AthletiCo ................................see inside front cover<br />
ATI Physical Therapy ............ see inside back cover<br />
Benefitdecisions, Inc.<br />
125 S. Wacker Dr., Ste. 2075<br />
Chicago, IL 60606<br />
(312) 606-4800 • (312) 606-8101 Fax<br />
www.benefitdecisions.com<br />
Central DuPage Hospital .................... see page 18<br />
Chicago Bulls ........................................ see page 32<br />
Chicago Magazine .............................. see page 17<br />
Chicago Office Technology Group .... see page 33<br />
Chicago Rehabilit<strong>at</strong>ion Services, Inc. .. see page 15<br />
Chicago <strong>Rush</strong> Arena Football ............. see page 29<br />
Citigroup ..........................................see back cover<br />
DePuy Spine ......................................... see page 18<br />
Gallagher Healthcare<br />
Insurance Services, Inc. .....................see page 23<br />
Girling Health Care, Inc. ..................... see page 32<br />
Harris Priv<strong>at</strong>e Bank .............................. see page 23<br />
H-Wave ................................................. see page 23<br />
Illinois Collection Service, Inc. ............ see page 32<br />
MB Financial Bank ............................... see page 22<br />
McGuireWoods LLP<br />
77 W. Wacker Dr., Ste. 4100<br />
Chicago, IL 60601<br />
(312) 849-8100 • (312) 849-3690 Fax<br />
www.mcguirewoods.com<br />
OccuSport Physical Therapy ............... see page 19<br />
Omnia Marketing & Design ............... see page 32<br />
P<strong>at</strong>ient Care ......................................... see page 29<br />
Perkins + Will ....................................... see page 28<br />
Physiotherapy Associ<strong>at</strong>es ...................... see page 9<br />
<strong>Rush</strong> Oak Park Hospital ……………… see page 23<br />
<strong>Rush</strong> SurgiCenter LP ............................ see page 22<br />
Scheck & Siress ..................................... see page 14<br />
Scribe Healthcare Technologies, Inc. . see page 18<br />
Spada Law Offices, P.C. ....................... see page 15<br />
The Center, Inc.<br />
1853 Bernice Rd.<br />
Lansing, IL 60438<br />
(800) 237-8228 • (708) 730-3324 Fax<br />
Directory<br />
WCS Physical Work Re-Training ......... see page 29<br />
William Blair & Company, L.L.C. ......... see page 19<br />
Wolf Financial Group .......................... see page 33<br />
Orthopaedic Excellence
Orthopaedic Excellence
Need Kicker
Orthopaedic Excellence<br />
One Westbrook Corpor<strong>at</strong>e Center, Ste. 240<br />
Westchester, IL 60154-5701