RESidENcy PROGRAM Scholarly and Community Medicine Projects
RESidENcy PROGRAM Scholarly and Community Medicine Projects
RESidENcy PROGRAM Scholarly and Community Medicine Projects

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Does Micropractice Lead to Macrosatisfaction?<br />
Meaghan Combs, MD, MPH; Elizabeth Paddock, MD; Melissa Stiles, MD, Ron Prince, MS<br />
University of Wisconsin, Department of Family <strong>Medicine</strong>, Madison, WI<br />
ABSTRACT RESULTS RESULTS OUTCOMES: SATISFACTION<br />
Physician quality of work life is a well recognized<br />
key factor in career choice <strong>and</strong> retention. No<br />
comparison exists between traditional practices <strong>and</strong><br />
p y p y p y<br />
by the University of Wisconsin Department of<br />
Family <strong>Medicine</strong> in community <strong>and</strong> residency<br />
clinics <strong>and</strong> physicians working in micropractice<br />
clinics across the USA. Micropractice clinics are<br />
defined as those which are independent, with low<br />
overhead, <strong>and</strong> extended visit time with patients.<br />
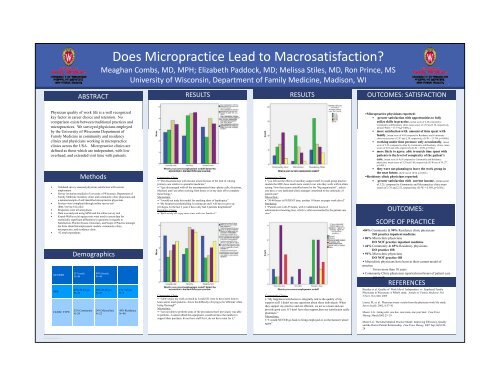
•Micropractice physicians reported:<br />
• greater satisfaction with opportunities to fully<br />
utilize skills in practice, (mean score of 4.38 compared to<br />
<strong>Community</strong> <strong>and</strong> Residency clinic mean scores of 3.55 <strong>and</strong> 3.58, respectively,<br />
(Krusal-Wallis = 13.779, p=0.001).)<br />
• more satisfaction with amount of time spent with<br />
family, (mean score of 4.09 compared to Residency <strong>and</strong> <strong>Community</strong><br />
clinic mean scores of 2.97 <strong>and</strong> 2.30, respectively, (K-W = 25.794, p=0.000).)<br />
• working under time pressure only occasionally, (mean<br />
score of 2.50, compared to often by <strong>Community</strong> <strong>and</strong> Residency clinics, mean<br />
scores of 4.07 <strong>and</strong> 4.08, respectively (K-W = 4.839, p=0.00).)<br />
• more likely to agree: able to match time spent with<br />
patients to the level of complexity of the patient’s<br />
care, (mean score of 4.63 compared to <strong>Community</strong> <strong>and</strong> Residency<br />
physicians, mean scores of 3.29 <strong>and</strong> 3.00, respectively (K-W test of 39.277,<br />
p=0.00).)<br />
• they were not planning to leave the work group in<br />
the h near ffuture,<br />
(K-W test of 10.94, p=0.004.)<br />
•Residency clinic physicians reported:<br />
• greater satisfaction with current income, (mean score<br />
of 3.25, compared to <strong>Community</strong> <strong>and</strong> Micropractice clinic mean<br />
scores of 2.76 <strong>and</strong> 2.32, respectively. (K-W = 6.549, p=0.38).)<br />
micropractices. We surveyed physicians employed ( ,p ))<br />
Methods <strong>Community</strong> Clinic:<br />
• “The dissatisfaction with income arises because of the lack of valuing<br />
• Validated survey assessed physician satisfaction with current<br />
employment<br />
• Survey invitation emailed to University of Wisconsin, Department of<br />
Family <strong>Medicine</strong> residency clinic <strong>and</strong> community clinic physicians <strong>and</strong><br />
a national sample of self-identified micropractice physicians<br />
• Surveys were completed through online survey tool<br />
(http.//survey.wisc.edu)<br />
• Responses were all anonymous<br />
• Data was analyzed y using gSPSS <strong>and</strong> the online survey y tool<br />
• Krusal-Wallis or chi-square tests were used to assess data for<br />
statistically significant differences to questions in regards to<br />
Satisfaction, Practice Issues, Outcomes, <strong>and</strong> Scope of Practice amongst<br />
the three identified employment models: community clinic,<br />
micropractice, <strong>and</strong> residency clinic.<br />
• 92 total respondents<br />
GENDER<br />
AGE<br />
CLINIC TYPE<br />
RESEARCH POSTER PRESENTATION DESIGN © 2011<br />
www.PosterPresentations.com<br />
Demographics g p<br />
51% male<br />
N=46<br />
47% 25-45 yrs<br />
N=43<br />
32% <strong>Community</strong><br />
N=29<br />
49% female<br />
N=44<br />
52% 45-65 yrs<br />
N=47<br />
24% Microclinic<br />
N=22<br />
1% >65 yrs<br />
N=1<br />
44% Residency<br />
N=40<br />
primary care relative to specialist medicine.”<br />
• “I get discouraged with all the uncompensated time--phone calls, dictations,<br />
Mychart, <strong>and</strong> I am often working from home or on my days off to complete<br />
these things.”<br />
Microclinic:<br />
• “I would not trade this model for anything short of bankruptcy”<br />
• “My hospital recredentialling is coming up <strong>and</strong> I will have to give up<br />
privileges. In the last 2 years I have only had 2 patients hospitalized”<br />
Residency Clinic:<br />
• “We'd W nearly yall enjoy j y more time with our families!”<br />
<strong>Community</strong> Clinic:<br />
• “I don't enjoy jymy ywork<br />
as much as I could if I were to have more time to<br />
learn <strong>and</strong> to teach patients...this is the difficulty of trying to be 'efficient' while<br />
being 'thorough'”<br />
Microclinic:<br />
• “I am not able to perform some of the procedures that I previously was able<br />
to perform...I cannot afford this equipment, would not have the number to<br />
support their purchase, do not have staff for it, do not have room for it.”<br />
<strong>Community</strong> Clinic:<br />
• “you left out the effects of ancillary support staff. In small group practice<br />
models the MD's have much more control over who they work with in clinic<br />
setting. Now that seems controlled more by the "big organization" , unless<br />
you have a very dedicated clinic manager committed to the continuity of<br />
patient care”<br />
Microclinic:<br />
• “30-40 hours is PATIENT time, another 10 hours on paper work drivel”<br />
Residency:<br />
• “Patient care is 40-55 hours, with 12 additional hours of<br />
administrative/teaching time, which is often encroached by the patient care<br />
time”<br />
<strong>Community</strong> Clinic:<br />
• “My My happiness/satisfaction is integrally tied to the quality of my<br />
support staff. I didn't see any questions about these individuals. When<br />
they support my practice <strong>and</strong> are efficient, we act as a team <strong>and</strong> can<br />
provide good care. If I don't have that support,then my satisfaction really<br />
plummets.”<br />
Microclinic:<br />
• “I would NEVER go back to being employed or on the hamster wheel<br />
again”<br />
OUTCOMES:<br />
SCOPE OF PRACTICE<br />
•84% <strong>Community</strong> & 90% Residency clinic physicians<br />
DO practice inpatient medicine<br />
• 86% Microclinic physicians<br />
DO NOT practice inpatient medicine<br />
• 44% <strong>Community</strong> & 65% Residency physicians<br />
DO practice OB<br />
• 91% Microclinic physicians<br />
DO NOT practice ti OB<br />
• Microclinic physicians have been in their current model of<br />
practice<br />
for no more than 10 years<br />
• <strong>Community</strong> Clinic physicians reported most hours of patient care<br />
per week<br />
REFERENCES<br />
Beasley et. al. Quality of Work life of Independent vs Employed Family<br />
Physicians in Wisconsin: A WReN study. Annals of Family <strong>Medicine</strong>. Vol<br />
3,No 6. Nov/Dec 2005<br />
Linzer, M, et. al. Physician stress: results from the physician work life study.<br />
Stress health. 2002; 8:37-42<br />
Moore LG. Going solo: one doc, one room, one year later. Fam Pract<br />
Manag. March2002:25–29.<br />
Moore LG. The Ideal Medical Practice Model: Improving Efficiency, Quality<br />
<strong>and</strong> the Doctor-Patient Relationship. Fam Pract Manag. 2007 Sep;14(8):20-<br />
24<br />
5/13/2011<br />
1