Pseudo ECG-gating in fetal cardiac MRI
Pseudo ECG-gating in fetal cardiac MRI
Pseudo ECG-gating in fetal cardiac MRI
- TAGS
- pseudo
- fetal
- cardiac
- www.ohsu.edu

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
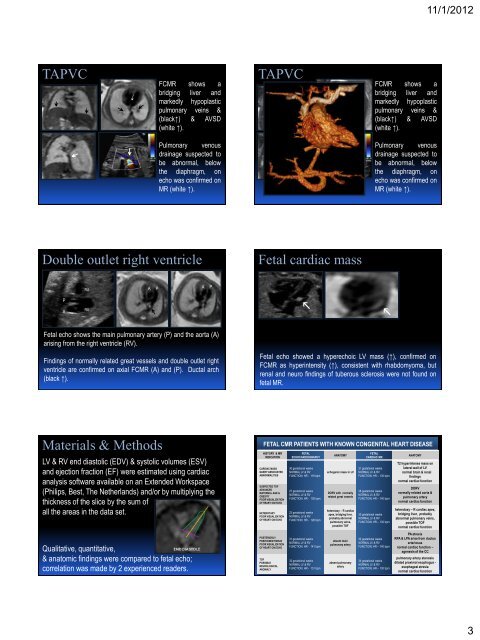
TAPVC<br />
FCMR shows a<br />
bridg<strong>in</strong>g liver and<br />
markedly hypoplastic<br />
pulmonary ve<strong>in</strong>s &<br />
(black↑) & AVSD<br />
(white ↑).<br />
Pulmonary venous<br />
dra<strong>in</strong>age suspected to<br />
be abnormal, below<br />
the diaphragm, on<br />
echo was confirmed on<br />
MR (white ↑).<br />
Double outlet right ventricle<br />
P<br />
A<br />
RA<br />
RV<br />
A P<br />
Fetal echo shows the ma<strong>in</strong> pulmonary artery (P) and the aorta (A)<br />
aris<strong>in</strong>g from the right ventricle (RV).<br />
F<strong>in</strong>d<strong>in</strong>gs of normally related great vessels and double outlet right<br />
ventricle are confirmed on axial FCMR (A) and (P). Ductal arch<br />
(black ↑).<br />
TAPVC<br />
Materials & Methods Results<br />
A P<br />
LV & RV end diastolic (EDV) & systolic volumes (ESV)<br />
and ejection fraction (EF) were estimated us<strong>in</strong>g <strong>cardiac</strong><br />
analysis software available on an Extended Workspace<br />
(Philips, Best, The Netherlands) and/or by multiply<strong>in</strong>g the<br />
thickness of the slice by the sum of<br />
all the areas <strong>in</strong> the data set.<br />
Qualitative, quantitative,<br />
& anatomic f<strong>in</strong>d<strong>in</strong>gs were compared to <strong>fetal</strong> echo;<br />
correlation was made by 2 experienced readers.<br />
Fetal <strong>cardiac</strong> mass<br />
FCMR shows a<br />
bridg<strong>in</strong>g liver and<br />
markedly hypoplastic<br />
pulmonary ve<strong>in</strong>s &<br />
(black↑) & AVSD<br />
(white ↑).<br />
Pulmonary venous<br />
dra<strong>in</strong>age suspected to<br />
be abnormal, below<br />
the diaphragm, on<br />
echo was confirmed on<br />
MR (white ↑).<br />
Fetal echo showed a hyperechoic LV mass (↑), confirmed on<br />
FCMR as hyper<strong>in</strong>tensity (↑), consistent with rhabdomyoma, but<br />
renal and neuro f<strong>in</strong>d<strong>in</strong>gs of tuberous sclerosis were not found on<br />
<strong>fetal</strong> MR.<br />
FETAL CMR PATIENTS WITH KNOWN CONGENITAL HEART DISEASE<br />
HISTORY & MR<br />
INDICATION<br />
CARDIAC MASS<br />
QUERY ASSOCIATED<br />
ABNORMALITIES<br />
SUSPECTED TOF<br />
ADVANCED<br />
MATERNAL AGE &<br />
OBESITY<br />
POOR VISUALIZATION<br />
OF HEART ON ECHO<br />
HETEROTAXY<br />
POOR VISUALIZATION<br />
OF HEART ON ECHO<br />
POSTERIORLY<br />
POSITIONED TWIN B<br />
POOR VISUALIZATION<br />
OF HEART ON ECHO<br />
TOF<br />
POSSIBLE<br />
NEUROLOGICAL<br />
ANOMALY<br />
FETAL<br />
ECHOCARDIOGRAPHY<br />
30 gestational weeks<br />
NORMAL LV & RV<br />
FUNCTION; HR - 119 bpm<br />
27 gestational weeks<br />
NORMAL LV & RV<br />
FUNCTION; HR - 136 bpm<br />
23 gestational weeks<br />
NORMAL LV & RV<br />
FUNCTION; HR - 126 bpm<br />
31 gestational weeks<br />
NORMAL LV & RV<br />
FUNCTION; HR - 141 bpm<br />
32 gestational weeks<br />
NORMAL LV & RV<br />
FUNCTION; HR - 131 bpm<br />
ANATOMY<br />
echogenic mass <strong>in</strong> LV<br />
DORV with normally<br />
related great vessels<br />
heterotaxy – R <strong>cardiac</strong><br />
apex, bridg<strong>in</strong>g liver,<br />
probably abnormal<br />
pulmonary ve<strong>in</strong>s,<br />
possible TOF<br />
absent ma<strong>in</strong><br />
pulmonary artery<br />
absent pulmonary<br />
artery<br />
FETAL<br />
CARDIAC MR<br />
31 gestational weeks<br />
NORMAL LV & RV<br />
FUNCTION; HR – 130 bpm<br />
28 gestational weeks<br />
NORMAL LV & RV<br />
FUNCTION; HR – 140 bpm<br />
30 gestational weeks<br />
NORMAL LV & RV<br />
FUNCTION; HR – 130 bpm<br />
32 gestational weeks<br />
NORMAL LV & RV<br />
FUNCTION; HR – 140 bpm<br />
34 gestational weeks<br />
NORMAL LV & RV<br />
FUNCTION; HR – 130 bpm<br />
ANATOMY<br />
T2 hyper<strong>in</strong>tense mass on<br />
lateral wall of LV<br />
normal bra<strong>in</strong> & renal<br />
f<strong>in</strong>d<strong>in</strong>gs<br />
normal <strong>cardiac</strong> function<br />
DORV<br />
normally related aorta &<br />
pulmonary artery<br />
normal <strong>cardiac</strong> function<br />
heterotaxy – R <strong>cardiac</strong> apex,<br />
bridg<strong>in</strong>g liver, probably<br />
abnormal pulmonary ve<strong>in</strong>s,<br />
possible TOF<br />
normal <strong>cardiac</strong> function<br />
PA atresia<br />
RPA & LPA arise from ductus<br />
arteriosus<br />
normal <strong>cardiac</strong> function –<br />
agenesis of the CC<br />
pulmonary artery stenosis<br />
dilated proximal esophagus -<br />
esophageal atresia<br />
normal <strong>cardiac</strong> function<br />
11/1/2012<br />
3