Images - Department of Radiology & Biomedical Imaging ...
Images - Department of Radiology & Biomedical Imaging ...
Images - Department of Radiology & Biomedical Imaging ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
6<br />
clinical and research news<br />
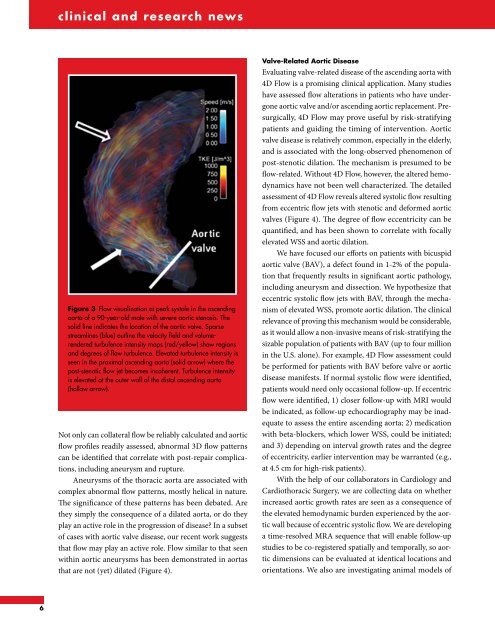
Figure 3 Flow visualization at peak systole in the ascending<br />
aorta <strong>of</strong> a 90-year-old male with severe aortic stenosis. The<br />
solid line indicates the location <strong>of</strong> the aortic valve. Sparse<br />
streamlines (blue) outline the velocity field and volumerendered<br />
turbulence intensity maps (red/yellow) show regions<br />
and degrees <strong>of</strong> flow turbulence. Elevated turbulence intensity is<br />
seen in the proximal ascending aorta (solid arrow) where the<br />
post-stenotic flow jet becomes incoherent. Turbulence intensity<br />
is elevated at the outer wall <strong>of</strong> the distal ascending aorta<br />
(hollow arrow).<br />
Not only can collateral flow be reliably calculated and aortic<br />
flow pr<strong>of</strong>iles readily assessed, abnormal 3D flow patterns<br />
can be identified that correlate with post-repair complications,<br />
including aneurysm and rupture.<br />
Aneurysms <strong>of</strong> the thoracic aorta are associated with<br />
complex abnormal flow patterns, mostly helical in nature.<br />
The significance <strong>of</strong> these patterns has been debated. Are<br />
they simply the consequence <strong>of</strong> a dilated aorta, or do they<br />
play an active role in the progression <strong>of</strong> disease? In a subset<br />
<strong>of</strong> cases with aortic valve disease, our recent work suggests<br />
that flow may play an active role. Flow similar to that seen<br />
within aortic aneurysms has been demonstrated in aortas<br />
that are not (yet) dilated (Figure 4).<br />
Valve-Related Aortic Disease<br />
Evaluating valve-related disease <strong>of</strong> the ascending aorta with<br />
4D Flow is a promising clinical application. Many studies<br />
have assessed flow alterations in patients who have undergone<br />
aortic valve and/or ascending aortic replacement. Presurgically,<br />
4D Flow may prove useful by risk-stratifying<br />
patients and guiding the timing <strong>of</strong> intervention. Aortic<br />
valve disease is relatively common, especially in the elderly,<br />
and is associated with the long-observed phenomenon <strong>of</strong><br />
post-stenotic dilation. The mechanism is presumed to be<br />
flow-related. Without 4D Flow, however, the altered hemodynamics<br />
have not been well characterized. The detailed<br />
assessment <strong>of</strong> 4D Flow reveals altered systolic flow resulting<br />
from eccentric flow jets with stenotic and deformed aortic<br />
valves (Figure 4). The degree <strong>of</strong> flow eccentricity can be<br />
quantified, and has been shown to correlate with focally<br />
elevated WSS and aortic dilation.<br />
We have focused our efforts on patients with bicuspid<br />
aortic valve (BAV), a defect found in 1-2% <strong>of</strong> the population<br />
that frequently results in significant aortic pathology,<br />
including aneurysm and dissection. We hypothesize that<br />
eccentric systolic flow jets with BAV, through the mechanism<br />
<strong>of</strong> elevated WSS, promote aortic dilation. The clinical<br />
relevance <strong>of</strong> proving this mechanism would be considerable,<br />
as it would allow a non-invasive means <strong>of</strong> risk-stratifying the<br />
sizable population <strong>of</strong> patients with BAV (up to four million<br />
in the U.S. alone). For example, 4D Flow assessment could<br />
be performed for patients with BAV before valve or aortic<br />
disease manifests. If normal systolic flow were identified,<br />
patients would need only occasional follow-up. If eccentric<br />
flow were identified, 1) closer follow-up with MRI would<br />
be indicated, as follow-up echocardiography may be inadequate<br />
to assess the entire ascending aorta; 2) medication<br />
with beta-blockers, which lower WSS, could be initiated;<br />
and 3) depending on interval growth rates and the degree<br />
<strong>of</strong> eccentricity, earlier intervention may be warranted (e.g.,<br />
at 4.5 cm for high-risk patients).<br />
With the help <strong>of</strong> our collaborators in Cardiology and<br />
Cardiothoracic Surgery, we are collecting data on whether<br />
increased aortic growth rates are seen as a consequence <strong>of</strong><br />
the elevated hemodynamic burden experienced by the aortic<br />
wall because <strong>of</strong> eccentric systolic flow. We are developing<br />
a time-resolved MRA sequence that will enable follow-up<br />
studies to be co-registered spatially and temporally, so aortic<br />
dimensions can be evaluated at identical locations and<br />
orientations. We also are investigating animal models <strong>of</strong>