d maryland declaración del impuesto sobre el ingreso de residentes
d maryland declaración del impuesto sobre el ingreso de residentes
d maryland declaración del impuesto sobre el ingreso de residentes

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
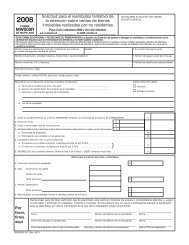
Escriba utilizando sólo tinta azul o negra.<br />
FORMA<br />
503<br />
Marque solamente una casilla<br />
Coloque <strong>el</strong> CHEQUE o <strong>el</strong> GIRO POSTAL<br />
<strong>sobre</strong> sus comprobantes <strong>de</strong> salarios e<br />
<strong>impuesto</strong>s, y adjúnt<strong>el</strong>os aquí con UNA grapa.<br />
MARYLAND<br />
DECLARACIÓN DEL IMPUESTO SOBRE EL<br />
INGRESO DE RESIDENTES<br />
N.º DE SEGURO SOCIAL N.º DE SEGURO SOCIAL DEL CÓNYUGE<br />
Su nombre Inicial Ap<strong>el</strong>lido<br />
Su nombre Inicial Ap<strong>el</strong>lido<br />
DIRECCIÓN ACTUAL (Nro. y calle)<br />
Ciudad Estado Código postal<br />
Nombre <strong>d<strong>el</strong></strong> condado y ciudad incorporada, localidad o área<br />
<strong>de</strong> <strong>impuesto</strong> especial en la que estuvo residiendo <strong>el</strong> último día<br />
<strong>d<strong>el</strong></strong> período tributable. (Vea la Instrucción 6)<br />
ESTADO CIVIL PARA EFECTOS DE LA DECLARACIÓN:<br />
Vea la Instrucción 1 para <strong>de</strong>terminar si <strong>de</strong>be realizar la presentación.<br />
1. Soltero/a (Si pue<strong>de</strong> estar incluido/a en la <strong><strong>de</strong>claración</strong> <strong>de</strong> <strong>impuesto</strong>s <strong>de</strong> otra persona, use <strong>el</strong> estado 6).<br />
2. Casado/a que presenta <strong><strong>de</strong>claración</strong> conjunta o cónyuge que no tuvo <strong>ingreso</strong>s<br />
3. Casado/a que presenta <strong><strong>de</strong>claración</strong> por separado<br />
NÚMERO DE SEGURO SOCIAL DEL CÓNYUGE<br />
EXENCIONES: Vea la Instrucción 10<br />
(A) Propia Cónyuge <br />
Condado <strong>de</strong> Ciudad o área <strong>de</strong> <strong>impuesto</strong><br />
Maryland<br />
Marque aquí si usted es: Su cónyuge tiene:<br />
(B) <br />
<br />
65 o mayor Ciego/a 65 o mayor Ciego/a<br />
(1) Primer nombre Ap<strong>el</strong>lido<br />
Cantidad <strong>de</strong> la exención<br />
4. Cabeza <strong>de</strong> familia<br />
5. Viudo/a que reúne los requisitos con hijo <strong>de</strong>pendiente<br />
6. Contribuyente <strong>de</strong>pendiente (Anote 0 en la Casilla <strong>de</strong> exenciones (A):<br />
Vea la instrucción 7)<br />
(A) Anote <strong>el</strong> n.º marcado . . . . $3,200 $ ____________<br />
(B) Anote <strong>el</strong> n.º marcado . . . . . $1,000 $ ____________<br />
(C) Anote <strong>el</strong> n.º marcado<br />
en las columnas 6 y 7 . . . .<br />
(D) Anote <strong>el</strong> total <strong>de</strong> las exenciones<br />
(Sume A, B, y C) . . . . .<br />
$3,200 $ ____________<br />
1. Ingreso bruto ajustado <strong>de</strong> su <strong><strong>de</strong>claración</strong> fe<strong>de</strong>ral (Vea la Instrucción 11) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .<br />
(Si <strong>el</strong> monto es $100,000 o más, <strong>de</strong>téngase y utilice la Forma 502) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .<br />
. .<br />
1<br />
1a.<br />
2.<br />
Salarios, su<strong>el</strong>dos y propinas (Vea la Instrucción 11) . . . . . . . . . . . . . . . . . . . . . . .<br />
. . . 1a.<br />
Deducción estándar (Vea la Instrucción 16) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .<br />
. . 2<br />
3. Ingreso neto (Reste la línea 2 <strong>de</strong> la línea 1) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3<br />
4. Cantidad <strong>de</strong> la exención como se calculó anteriormente . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4<br />
5. Ingreso neto tributable (Reste la línea 4 <strong>de</strong> la línea 3. VAYA A LA TABLA DE IMPUESTO, página 18). . . . . . . . . . . . . . . . . . . . . . . . . . 5<br />
6. Impuesto <strong>de</strong> Maryland <strong>de</strong> la Tabla <strong>de</strong> <strong>impuesto</strong> . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6<br />
7. Crédito por <strong>ingreso</strong> <strong>d<strong>el</strong></strong> trabajo 7a Crédito por niv<strong>el</strong> <strong>de</strong> pobreza 7b<br />
(Vea la Instrucción 18) Total 7<br />
8. Impuesto <strong>de</strong> Maryland <strong>de</strong>spués <strong>de</strong> los créditos (Reste la línea 7 <strong>de</strong> la línea 6). Si <strong>el</strong> resultado es menor que 0, anote 0.<br />
8<br />
9. Impuesto local (Vea la Instrucción 19 para obtener las tasas <strong>de</strong> <strong>impuesto</strong> y la hoja <strong>de</strong> cómputo). Multiplique la línea 5 por su tasa <strong>de</strong> <strong>impuesto</strong> local.___ 0 ___ ___ ___ 9<br />
10. Local: Crédito por <strong>ingreso</strong> <strong>d<strong>el</strong></strong> trabajo 10a<br />
Crédito por niv<strong>el</strong> <strong>de</strong> pobreza 10b<br />
(Vea la Instrucción 19) Total 10<br />
11. Impuesto local <strong>de</strong>spués <strong>de</strong> los créditos (Reste la línea 10 <strong>de</strong> la línea 9). Si <strong>el</strong> resultado es menor que 0, anote 0.<br />
11<br />
12. Total <strong>de</strong> <strong>impuesto</strong> <strong>de</strong> Maryland y local (Sume las líneas 8 y 11) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12<br />
13. Donaciones a Chesapeake Bay y a Endangered Species Fund . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .<br />
. . 13<br />
14. Donaciones a Fair Campaign Financing Fund . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .<br />
. . 14<br />
15. Donaciones a Maryland Cancer Fund . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .<br />
. . 15<br />
16. Total <strong>d<strong>el</strong></strong> <strong>impuesto</strong> <strong>sobre</strong> <strong>el</strong> <strong>ingreso</strong> <strong>de</strong> Maryland, <strong>d<strong>el</strong></strong> <strong>impuesto</strong> <strong>sobre</strong> <strong>el</strong> <strong>ingreso</strong> local y <strong>de</strong> donaciones (Sume las líneas 12 a la 15) 16<br />
17. Total <strong>d<strong>el</strong></strong> <strong>impuesto</strong> <strong>de</strong> Maryland y local retenido (anote <strong>el</strong> total <strong>de</strong> sus formas W-2 y 1099, y adjúnt<strong>el</strong>as si <strong>el</strong> <strong>impuesto</strong> <strong>de</strong> MD es retenido) 17<br />
18. Crédito por <strong>ingreso</strong> <strong>d<strong>el</strong></strong> trabajo reembolsable (<strong>de</strong> la hoja <strong>de</strong> cómputo en la Instrucción 21) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .<br />
. . 18<br />
19. Total <strong>de</strong> pagos y crédito (Sume las líneas 17 y 18) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19<br />
20. Saldo a pagar (si la línea 16 es mayor que la línea 19, reste la línea 19 <strong>de</strong> la línea 16) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .<br />
. . 20<br />
21. Pago en exceso (si la línea 16 es menor que la línea 19, reste la línea 16 <strong>de</strong> la línea 19). Vea la línea 24 Éste es su Reembolso 21<br />
22. Cargos por intereses <strong>de</strong> la Forma 502UP o por presentación fuera <strong>de</strong> plazo (Vea la Instrucción 22) Total . . .<br />
. . 22<br />
23. MONTO TOTAL A PAGAR (Sume las líneas 20 y 22) SI EL RESULTADO ES $1 O MÁS, PAGUE LA TOTALIDAD CON ESTA DECLARACIÓN 23<br />
Para pago <strong>el</strong>ectrónico o con tarjeta <strong>de</strong> crédito marque aquí y vea la Instrucción 24.<br />
DEPÓSITO DIRECTO DE REEMBOLSO (Vea la Instrucción 22). Verifique que la información <strong>sobre</strong> la cuenta sea correcta.<br />
24. Para s<strong>el</strong>eccionar la opción <strong>de</strong> <strong>de</strong>pósito directo, complete la siguiente información: 24a. Tipo <strong>de</strong> cuenta: Cuenta <strong>de</strong> cheque Cuenta <strong>de</strong> ahorros<br />
24b. Número <strong>de</strong> envío 24c. Número <strong>de</strong> cuenta <br />
<br />
<br />
<br />
Monto total $____________<br />
<br />
<br />
- -<br />
- -<br />
(C) Dependientes:<br />
(2) Número <strong>de</strong> seguro social (3) Parentesco<br />
<br />
<br />
N.° <strong>de</strong> t<strong>el</strong>éfono durante <strong>el</strong> día N.° <strong>de</strong> t<strong>el</strong>éfono particular<br />
CÓDIGO (3 dígitos por casilla)<br />
Declaro bajo pena <strong>de</strong> falso testimonio que he examinado esta <strong><strong>de</strong>claración</strong>, incluyendo los anexos y comprobantes adjuntos, y que, según Hacer los cheques paga<strong>de</strong>ros a: COMPTROLLER OF MARYLAND.<br />
mi leal saber y enten<strong>de</strong>r, es verda<strong>de</strong>ra, correcta y completa. Si la <strong><strong>de</strong>claración</strong> es preparada por otra persona que no sea <strong>el</strong> contribuyente, se Se recomienda que anote su número <strong>de</strong> seguro social en <strong>el</strong> cheque.<br />
<strong>de</strong>be basar en toda la información <strong>de</strong> la que dicho preparador tenga conocimiento. Marque aquí si autoriza a su preparador a discutir<br />
esta <strong><strong>de</strong>claración</strong> con nosotros.<br />
<br />
Envíe por correo a: Comptroller of Maryland, Revenue<br />
Administration Division, Annapolis, Maryland 21411-0001<br />
Su firma Fecha SSN o PTIN <strong>d<strong>el</strong></strong> preparador Firma <strong>d<strong>el</strong></strong> preparador que no sea <strong>el</strong> contribuyente<br />
Firma <strong>d<strong>el</strong></strong> cónyuge Fecha Dirección y número <strong>de</strong> t<strong>el</strong>éfono <strong>d<strong>el</strong></strong> preparador<br />
COM/RAD-020 08-60<br />
060<br />
(4) Marque<br />
si hay hijo<br />
<strong>de</strong>pendiente<br />
(5) Si la casilla Hijo<br />
<strong>de</strong>pendiente está marcada,<br />
¿<strong>el</strong> niño tiene<br />
asistencia médica?<br />
Sí No<br />
2008<br />
$<br />
(6)<br />
Regular<br />
(7)<br />
65 o<br />
mayor
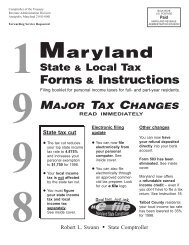
FORMA<br />
503 2007<br />
MARYLAND<br />
DECLARACIÓN DEL IMPUESTO<br />
SOBRE EL INGRESO DE RESIDENTES<br />
NOMBRE ______________________________ SSN ________________________<br />
¿QUIÉN PUEDE USAR ESTA FORMA?<br />
Usted pue<strong>de</strong> usar esta forma (Forma 503) si respon<strong>de</strong> “NO” a TODAS estas preguntas<br />
SÍ NO SÍ NO<br />
1. ¿Su <strong>ingreso</strong> bruto ajustado fe<strong>de</strong>ral es <strong>de</strong> 100,000 o más? 6. ¿Fue usted no resi<strong>de</strong>nte <strong>de</strong> Maryland?<br />
2. ¿Deberá realizar Sumas al <strong>ingreso</strong> o Restas <strong>d<strong>el</strong></strong> <strong>ingreso</strong> en<br />
su <strong><strong>de</strong>claración</strong> <strong>de</strong> Maryland? Si cumple los requisitos para<br />
una <strong>de</strong>ducción, como la exclusión por pensión, la Forma<br />
502 será beneficiosa para usted. Si tiene una cantidad que<br />
paga al estado en su Forma W-2, <strong>de</strong>be usar la Forma 502.<br />
3. ¿Desea <strong>de</strong>tallar las <strong>de</strong>ducciones?<br />
4. ¿Ha realizado pagos estimados en 2008; ha aplicado parte<br />
o todo su reembolso <strong>de</strong> 2007 a su cuenta estimada <strong>de</strong> 2008,<br />
o ha realizado un pago con una solicitud <strong>de</strong> prórroga,<br />
Forma 502E?<br />
5. ¿Está reclamando un crédito tributario con la Forma 500CR<br />
o la Forma 502CR <strong>de</strong> Maryland?<br />
7. ¿Fue usted resi<strong>de</strong>nte durante parte <strong>d<strong>el</strong></strong> año en Maryland?<br />
8. ¿Su <strong><strong>de</strong>claración</strong> abarca un período menor que 12 meses?<br />
9. ¿Fue usted contribuyente <strong>de</strong> un año fiscal?<br />
PAGE 2<br />
10. ¿Desea acreditar parte o todo su reembolso a la cuenta estimada<br />
<strong>d<strong>el</strong></strong> año próximo?