- Page 1 and 2: UNIVERSITE SIDI MOHAMMED BEN ABDELL
- Page 3 and 4: PATIENTS & METHODES ...............
- Page 5 and 6: VI-2-3. VOIES D’ABORD ...........
- Page 7 and 8: INTRODUCTION 6
- Page 9 and 10: RAPPELS 8
- Page 11 and 12: I-2. Développement embryonnaire du
- Page 13 and 14: comprend tous les lobes situés en
- Page 15 and 16: Dorsal Latéral Plaque recouvrante
- Page 17 and 18: La fosse cérébrale postérieure c
- Page 19 and 20: II-2. Contenu de la fosse cérébra
- Page 21 and 22: deux pédoncules cérébraux se sit
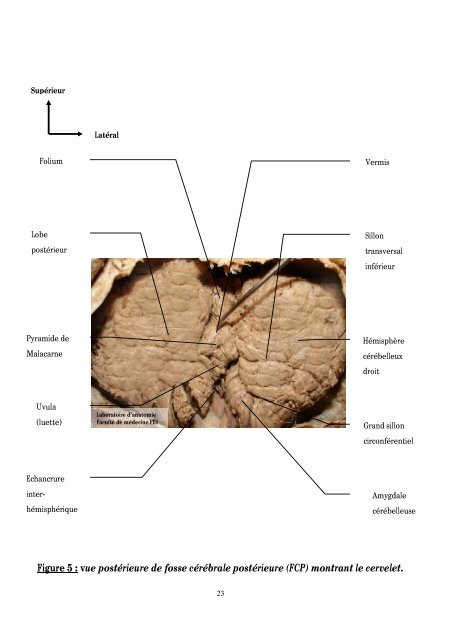
- Page 23: Ses mensurations sont [58] : Diamè
- Page 27 and 28: Antérieur Latéral Plancher du V4
- Page 29 and 30: Supérieur Latéral Arachnoïde Ner
- Page 31 and 32: Supérieur Latéral Artère céréb
- Page 33 and 34: II-2-5. Les vaisseaux : Pour optimi
- Page 35 and 36: II-2-5-2. Les veines : Les veines d
- Page 37 and 38: • La citerne pré-pontique et les
- Page 39 and 40: • la région de l’angle ponto-c
- Page 41 and 42: I. ETUDE : Nous avons revu les obse
- Page 43 and 44: L’œdème périlésionnel n’a p
- Page 45 and 46: (moyenne ± écart type et/ou médi
- Page 47 and 48: I. ANALYSE DESCRIPTIVE DES RESULTAT
- Page 49 and 50: 46,30% Masculin 53,70% Féminin Gra
- Page 51 and 52: Les troubles de conscience étaient
- Page 53 and 54: L’examen ophtalmologique était s
- Page 55 and 56: A B C D E F Figure 14 : IRM en coup
- Page 57 and 58: A B C D E F Figure 16 : TDM en coup
- Page 59 and 60: A B C D E F Figure 19 : TDM céréb
- Page 61 and 62: A B C D E F Figure 21 : TDM en coup
- Page 63 and 64: A B C D E F Figure 23 : Processus e
- Page 65 and 66: A B C D E F Figure 26 : Processus t
- Page 67 and 68: I-3-2. Exploration électro-physiol
- Page 69 and 70: Service de Neurochirurgie CHU Hassa
- Page 71 and 72: Concernant les médulloblastomes de
- Page 73 and 74: I-5. Evolution postopératoire: L
- Page 75 and 76:
CAS 2 → → A B C 24/01/2006 10/0
- Page 77 and 78:
I-6. Histologie : Type Nombre Pourc
- Page 79 and 80:
L’hydrocéphalie a été objectiv
- Page 81 and 82:
Traitement : Dérivation du LCR Ext
- Page 83 and 84:
II-4. Devenir en fonction du type h
- Page 85 and 86:
I. GENERALITES : Les tumeurs de la
- Page 87 and 88:
Cependant, il est de 40-50 ans pour
- Page 89 and 90:
hypoacousie ; ce qui est habituel p
- Page 91 and 92:
ésolution (Quel que soit son mode
- Page 93 and 94:
V-1. Tumeurs intra-axiales : V-1-1.
- Page 95 and 96:
A B Laboratoire d’anatomopatholog
- Page 97 and 98:
L’hémangioblastome est une tumeu
- Page 99 and 100:
L’astrocytome fibrillaire est con
- Page 101 and 102:
V-1-4. Gliome du tronc cérébral :
- Page 103 and 104:
A B C Laboratoire d’anatomopathol
- Page 105 and 106:
Approximativement 5% de schwannomes
- Page 107 and 108:
elativement peu élevée des ménin
- Page 109 and 110:
Microscopie Sa paroi comprend une m
- Page 111 and 112:
cérébelleux. À côté de ce siè
- Page 113 and 114:
VI. PRISE EN CHARGE THERAPEUTIQUE :
- Page 115 and 116:
• le pneumocéphale de tension. P
- Page 117 and 118:
énéficié d’une biopsie alors q
- Page 119 and 120:
dont la grande portion se situe sur
- Page 121 and 122:
VI-2-4-1. mortalité : La mortalit
- Page 123 and 124:
[92]. Dans environ 20 % des cas, un
- Page 125 and 126:
AUTEURS Nombre de cas Syndrome de l
- Page 127 and 128:
• 54 Gy en 30 fractions de 1,8 Gy
- Page 129 and 130:
VII. PRONOSTIC : VII-1. En fonction
- Page 131 and 132:
des techniques chirurgicales de rep
- Page 133 and 134:
CONCLUSION 132
- Page 135 and 136:
RESUME 134
- Page 137 and 138:
SUMMARY Posterior fossa tumors is a
- Page 139 and 140:
TUMEURS DE LA FOSSE CEREBRALE POSTE
- Page 141 and 142:
• Aspect Taille : ……………
- Page 143 and 144:
COMPLICATIONS : .Décès .Coma prol
- Page 145 and 146:
1. ALBERT L. RHOTON, JR. The poster
- Page 147 and 148:
22. ROBERT J. YOUNG, ALLEN K. SILLS
- Page 149 and 150:
43. BOUCHET A, GUILLERET J. Anatomi
- Page 151 and 152:
63. DUE-TONNESSEN B. J., HELSETH E.
- Page 153 and 154:
80. ANDREA JASPERT-GREHL. Cranial n
- Page 155 and 156:
97. PHILIPPE METELLUS, MARYLIN BARR
- Page 157 and 158:
112. X. COMBAZ, N. GIRARD, D. SCAVA
- Page 159:
128. KIRK EA, HOWARD VC, SCOTT CA.