Póliza Sobre el Uso de Drogas - West New York School
Póliza Sobre el Uso de Drogas - West New York School
Póliza Sobre el Uso de Drogas - West New York School

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
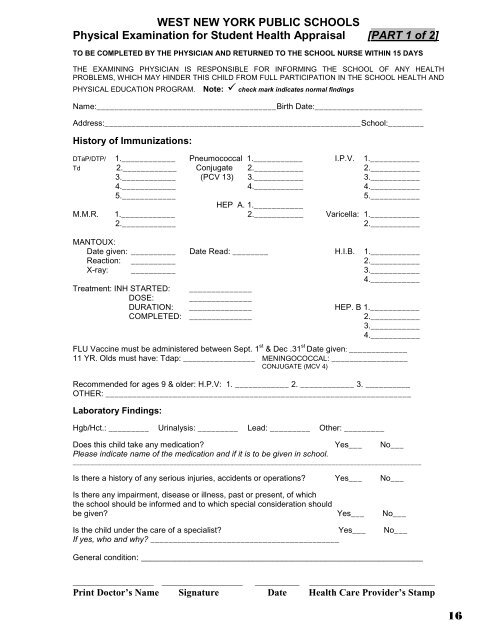
WEST NEW YORK PUBLIC SCHOOLS<br />
Physical Examination for Stu<strong>de</strong>nt Health Appraisal [PART 1 of 2]<br />
TO BE COMPLETED BY THE PHYSICIAN AND RETURNED TO THE SCHOOL NURSE WITHIN 15 DAYS<br />
THE EXAMINING PHYSICIAN IS RESPONSIBLE FOR INFORMING THE SCHOOL OF ANY HEALTH<br />
PROBLEMS, WHICH MAY HINDER THIS CHILD FROM FULL PARTICIPATION IN THE SCHOOL HEALTH AND<br />
PHYSICAL EDUCATION PROGRAM.<br />
Note: check mark indicates normal findings<br />
Name:________________________________________Birth Date:________________________<br />
Address:_________________________________________________________<strong>School</strong>:________<br />
History of Immunizations:<br />
DTaP/DTP/ 1.____________ Pneumococcal 1.___________ I.P.V. 1.___________<br />
Td 2.____________ Conjugate 2.___________ 2.___________<br />
3.____________ (PCV 13) 3.___________ 3.___________<br />
4.____________ 4.___________ 4.___________<br />
5.____________<br />
5.___________<br />
HEP A. 1.___________<br />
M.M.R. 1.____________ 2.___________ Varic<strong>el</strong>la: 1.___________<br />
2.____________<br />
2.___________<br />
MANTOUX:<br />
Date given: __________ Date Read: ________ H.I.B. 1.___________<br />
Reaction: __________ 2.___________<br />
X-ray: __________ 3.___________<br />
4.___________<br />
Treatment: INH STARTED: ______________<br />
DOSE: ______________<br />
DURATION: ______________ HEP. B 1.___________<br />
COMPLETED: ______________<br />
2.___________<br />
3.___________<br />
4.___________<br />
FLU Vaccine must be administered between Sept. 1 st & Dec .31 st Date given: _____________<br />
11 YR. Olds must have: Tdap: ________________ MENINGOCOCCAL: _________________<br />
CONJUGATE (MCV 4)<br />
Recommen<strong>de</strong>d for ages 9 & ol<strong>de</strong>r: H.P.V: 1. ____________ 2. ____________ 3. __________<br />
OTHER: ____________________________________________________________________<br />
Laboratory Findings:<br />
Hgb/Hct.: _________ Urinalysis: _________ Lead: _________ Other: _________<br />
Does this child take any medication? Yes___ No___<br />
Please indicate name of the medication and if it is to be given in school.<br />
_________________________________________________________________________________________________<br />
Is there a history of any serious injuries, acci<strong>de</strong>nts or operations? Yes___ No___<br />
Is there any impairment, disease or illness, past or present, of which<br />
the school should be informed and to which special consi<strong>de</strong>ration should<br />
be given? Yes___ No___<br />
Is the child un<strong>de</strong>r the care of a specialist? Yes___ No___<br />
If yes, who and why? __________________________________________<br />
General condition: __________________________________________________________<br />
____________________ ____________________ ___________ _______________________________<br />
Print Doctor’s Name Signature Date Health Care Provi<strong>de</strong>r’s Stamp<br />
16