Descarga
Descarga
Descarga

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
FUNDAP | ex - IAEPD 55<br />
| PERSONA<br />
factor (genetically based impulsivity, for example) is present, because of the need for<br />
a complementary pharmacological treatment.<br />
In a similar way, some patients from the bipolar or schizophrenic end of the spectrum<br />
are misdiagnosed as borderline when the clinical features look like they meet<br />
BPD criteria. But in the majority of the BPD spectrum of cases, trauma, attachment and<br />
biological factors will interact in a complex way that will manifest differently in each<br />
patient. What is essential is the need to understand the relative contribution of each of<br />
these factors to a specific problem in a patient, because many aspects of treatment,<br />
such as pharmacological interventions or EMDR therapy, would need to have more<br />
weight depending on this evaluation. We think that it is important not to consider<br />
these factors as contradictory with each other, but rather complementary and interactive.<br />
Thus, to draw environmental and biological factors as extremes of a spectrum, as<br />
we did, is not entirely adequate, because these factors are not mutually exclusive and<br />
it is possible to find cases with high weights of both biological and environmental factors.<br />
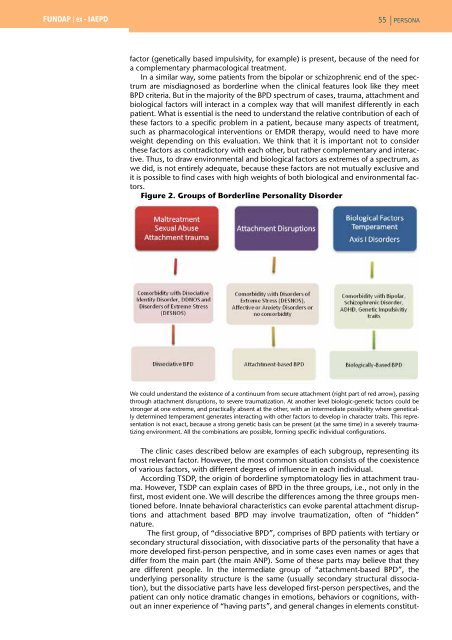
Figure 2. Groups of Borderline Personality Disorder<br />
We could understand the existence of a continuum from secure attachment (right part of red arrow), passing<br />
through attachment disruptions, to severe traumatization. At another level biologic-genetic factors could be<br />
stronger at one extreme, and practically absent at the other, with an intermediate possibility where genetically<br />
determined temperament generates interacting with other factors to develop in character traits. This representation<br />
is not exact, because a strong genetic basis can be present (at the same time) in a severely traumatizing<br />
environment. All the combinations are possible, forming specific individual configurations.<br />
The clinic cases described below are examples of each subgroup, representing its<br />
most relevant factor. However, the most common situation consists of the coexistence<br />
of various factors, with different degrees of influence in each individual.<br />
According TSDP, the origin of borderline symptomatology lies in attachment trauma.<br />
However, TSDP can explain cases of BPD in the three groups, i.e., not only in the<br />
first, most evident one. We will describe the differences among the three groups mentioned<br />
before. Innate behavioral characteristics can evoke parental attachment disruptions<br />
and attachment based BPD may involve traumatization, often of “hidden”<br />
nature.<br />
The first group, of “dissociative BPD”, comprises of BPD patients with tertiary or<br />
secondary structural dissociation, with dissociative parts of the personality that have a<br />
more developed first-person perspective, and in some cases even names or ages that<br />
differ from the main part (the main ANP). Some of these parts may believe that they<br />
are different people. In the intermediate group of “attachment-based BPD”, the<br />
underlying personality structure is the same (usually secondary structural dissociation),<br />
but the dissociative parts have less developed first-person perspectives, and the<br />
patient can only notice dramatic changes in emotions, behaviors or cognitions, without<br />
an inner experience of “having parts”, and general changes in elements constitut-