HYDRAGEL HEMOGLOBIN(E) K20 - Sebia Electrophoresis
HYDRAGEL HEMOGLOBIN(E) K20 - Sebia Electrophoresis
HYDRAGEL HEMOGLOBIN(E) K20 - Sebia Electrophoresis

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong><br />
Ref. 3010<br />
2005/03
UTILISATION<br />
- 1 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Le kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> permet la séparation des hémoglobines normales (A et A 2 ) et la détection des principales hémoglobines<br />
anormales : S ou D et C ou E, par électrophorèse sur gel d’agarose. L’analyse est réalisée sur l’hémolysat de globules rouges lavés. Les hémoglobines<br />
sont séparées en tampon alcalin (pH 8,5), fixées par la chaleur ou en milieu alcool / acide et colorées par une solution d’amidoschwarz. L’excès de<br />
colorant est éliminé en milieu acide.<br />
Le gel est alors prêt pour l’identification des différentes hémoglobines. L’analyse qualitative des hémoglobines normales et anormales peut être<br />
réalisée. La densitométrie donne une quantification relative précise de chaque zone individualisée dont les hémoglobines présentant un intérêt<br />
particulier, telles que l’hémoglobine A 2 pour le diagnostic des ß thalassémies. L’électrophorèse sur gel acide du kit <strong>HYDRAGEL</strong> ACID(E)<br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, permet de confirmer l’identification des variants de l’hémoglobine, en particulier, de différencier l’hémoglobine S de<br />
l’hémoglobine D et l’hémoglobine E de l’hémoglobine C.<br />
Chaque gel d’agarose contenu dans le kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> est prévu pour l’analyse de 7 échantillons.<br />
À usage in vitro exclusivement.<br />
PRINCIPE DU TEST<br />
L’hémoglobine est une molécule complexe composée de quatre chaînes polypeptidiques, identiques deux à deux, chaque chaîne étant liée à l’hème,<br />
noyau tétrapyrrolique (porphyrine) lié à un atome de fer. L’hème est commun à toutes les hémoglobines. La partie protéique responsable du type<br />
d’hémoglobine est appelée globine. On connaît principalement les chaînes polypeptidiques α, ß, δ et γ. Chez l'homme, on peut trouver les<br />
hémoglobines normales suivantes :<br />
• hémoglobine A ................................... = α 2 ß 2<br />
• hémoglobine A 2 .................................. = α 2 δ 2<br />
• hémoglobine fœtale F ........................ = α 2 γ 2<br />
La chaîne α est commune à ces trois hémoglobines.<br />
La structure spatiale de l’hémoglobine (comme celle de toutes les protéines) dépend de la nature et de la séquence des acides aminés constituant<br />
les chaînes. Les liaisons qui se forment entre les différents acides aminés sont responsables de la forme de la molécule, de sa stabilité et de ses<br />
propriétés. Placées dans un champ électrique, les hémoglobines se déplacent en fonction de leur charge, de la taille de la molécule, de la force<br />
ionique, du pH du tampon et de la nature du support. Les variants de l’hémoglobine sont dus à des mutations de certains acides aminés entraînant<br />
des charges de surface différentes et donc des mobilités différentes en électrophorèse.<br />
Les anomalies de l’hémoglobine sont de deux sortes :<br />
• anomalies qualitatives ou de structure constituant le groupe des hémoglobinopathies ;<br />
• anomalies quantitatives ou de régulation constituant le groupe des thalassémies.<br />
RÉACTIFS FOURNIS DANS LE KIT <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong><br />
| COMPOSANTS | RÉF. N° 3010 |<br />
| Gels d’agarose (prêts à l’emploi) | 10 gels |<br />
| Tampon Tris-Barbital (solution concentrée) | 3 fl. de 75 mL |<br />
| Diluant colorant (solution concentrée) | 1 fl. de 60 mL |<br />
| Colorant amidoschwarz (solution concentrée) | 1 fl. de 20 mL |<br />
| Décolorant (solution concentrée) | 1 fl. de 100 mL |<br />
| Solution hémolysante (prête à l’emploi) | 1 fl. de 20 mL |<br />
| Applicateurs 7 dents (prêts à l’emploi) | 1 boîte de 10<br />
|<br />
|<br />
Papiers-filtres fins | 1 sachet de 10 |<br />
POUR DES RÉSULTATS OPTIMUMS<br />
Les éléments d’un même kit doivent être utilisés ensemble et selon les instructions de la notice.<br />
LIRE ATTENTIVEMENT LA NOTICE D’UTILISATION.<br />
1. GELS D’AGAROSE<br />
Préparation<br />
Les gels d’agarose sont prêts à l’emploi. Chaque gel contient : agarose, 8 g/L ; tampon alcalin, pH 8,5 ± 0,1 ; composants sans danger aux<br />
concentrations utilisées, nécessaires pour des performances optimales.<br />
Utilisation<br />
Support pour l’électrophorèse des hémoglobines.<br />
Conservation, stabilité et signes de détérioration<br />
Les gels doivent être conservés à température ambiante (de 15 à 30 °C) ou au réfrigérateur (entre 2 et 8 °C). Ils sont stables jusqu’à la date<br />
d’expiration indiquée sur le kit ou sur le sachet du gel. Les gels doivent être conservés horizontalement dans leur sachet de protection (la flèche sur<br />
le devant du kit doit être pointée vers le haut). Ne pas stocker les gels à proximité d’une fenêtre ou d’une source de chaleur. Éviter toute variation<br />
brutale de température.<br />
NE PAS CONGELER.<br />
Éliminer le gel dans les cas suivants :<br />
(i) apparition de cristaux, de précipité en surface du gel ou texture du gel très molle (indiquant que le gel a gelé) ;<br />
(ii) apparition de bactéries ou de moisissures ;<br />
(iii) présence anormale de liquide dans la boîte du gel (indiquant une exsudation du gel liée à de mauvaises conditions de conservation).<br />
NOTICE D’UTILISATION SEBIA - Français
- 2 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
2. TAMPON TRIS-BARBITAL<br />
Préparation<br />
Chaque flacon de tampon concentré doit être complété à 1 litre avec de l’eau distillée ou déminéralisée.<br />
Après dilution, la solution contient : tampon tris-barbital, pH 9,2 ± 0,3 ; azoture de sodium.<br />
ATTENTION : Le tampon concentré contient 2,45 % de barbital, 13,73 % de barbital sodé et 0,13 % d’azoture de sodium. Ne pas avaler ! En cas<br />
d’ingestion, consulter immédiatement un médecin ! L’azoture de sodium peut former des complexes explosifs ou toxiques en cas de contact<br />
avec des acides, du plomb ou du cuivre. Au moment de l’élimination des solutions, laver abondamment avec une grande quantité d’eau.<br />
Utilisation<br />
Tampon d’électrophorèse.<br />
Conservation, stabilité et signes de détérioration<br />
Le tampon concentré peut être conservé à température ambiante ou au réfrigérateur. Il est stable pendant plusieurs années et au minimum jusqu’à<br />
la date d’expiration indiquée sur le kit ou sur l’étiquette du flacon de tampon.<br />
Le tampon dilué est stable pendant un an à température ambiante en flacon fermé.<br />
Éliminer le tampon dilué s’il y a un changement d’aspect ou apparition d’un trouble dû à une contamination microbienne.<br />
3. DILUANT COLORANT<br />
Préparation<br />
Le diluant colorant concentré doit être utilisé comme décrit dans le paragrahe " COLORANT AMIDOSCHWARZ ". Il contient une solution acide.<br />
Utilisation<br />
Pour la préparation du colorant amidoschwarz.<br />
Conservation, stabilité et signes de détérioration<br />
Le diluant colorant concentré peut être conservé à température ambiante ou au réfrigérateur. Il est stable jusqu’à la date d’expiration indiquée sur le<br />
kit ou sur l’étiquette du flacon de diluant. NE PAS CONGELER.<br />
Ne pas ajouter d’azoture de sodium.<br />
4. COLORANT AMIDOSCHWARZ<br />
Préparation<br />
Le colorant amidoschwarz concentré est une solution visqueuse qui peut éventuellement gélifier, ce qui n’affecte absolument pas la qualité de la<br />
solution finale et son pouvoir de coloration.<br />
Dans tous les cas, pour obtenir une parfaite reconstitution du colorant, il faut respecter le protocole suivant :<br />
1. Ajouter environ 15 mL de diluant colorant au flacon d’amidoschwarz concentré.<br />
2. Refermer soigneusement le flacon.<br />
3. Agiter très vigoureusement le flacon pendant au minimum 5 secondes.<br />
4. Verser la solution obtenue dans le récipient de préparation de la solution de coloration.<br />
5. Renouveler cette opération deux fois, trois fois, si nécessaire.<br />
6. Verser le reste du diluant dans le récipient de préparation de la solution de coloration.<br />
7. Compléter à 300 mL avec de l’eau distillée ou déminéralisée.<br />
8. Agiter parfaitement cette solution pendant 5 à 10 minutes.<br />
Le colorant est prêt à l’emploi.<br />
Après dilution, la solution colorante contient : solution acide pH ≈ 2 ; amidoschwarz, 4 g/L ; éthylène-glycol, 6,7 % ; composants sans danger aux<br />
concentrations utilisées, nécessaires pour des performances optimales.<br />
ATTENTION : Nocif en cas d’ingestion.<br />
Utilisation<br />
Pour la coloration des gels après séparation électrophorétique des protéines.<br />
IMPORTANT : Le colorant est uniquement destiné à la coloration de 10 gels. Renouveler le colorant après 10 utilisations.<br />
Conservation, stabilité et signes de détérioration<br />
Les solutions de colorant concentrée et diluée peuvent être conservées à température ambiante ou au réfrigérateur en flacons fermés pour éviter<br />
l’évaporation. La solution concentrée est stable jusqu’à la date d’expiration indiquée sur le kit ou sur l’étiquette du flacon de colorant.<br />
La solution diluée est stable pendant 1 mois.<br />
Ne pas stocker la solution de colorant diluée à proximité d’une source de chaleur.<br />
5. DÉCOLORANT<br />
Préparation<br />
Le flacon de décolorant concentré doit être dilué au 1/1000 avec de l’eau distillée ou déminéralisée, il permet d'obtenir 100 litres de solution<br />
décolorante.<br />
Prélever par quantité de 1 mL et compléter à 1 litre avec de l’eau distillée ou déminéralisée.<br />
Après dilution, la solution décolorante contient : acide citrique, 0,5 g/L.<br />
Utilisation<br />
Pour la décoloration, c’est-à-dire l’élimination de l’excès de colorant après coloration du gel.<br />
Conservation, stabilité et signes de détérioration<br />
Le décolorant concentré peut être conservé à température ambiante ou au réfrigérateur. Il est stable jusqu’à la date d’expiration indiquée sur le kit ou<br />
sur l’étiquette du flacon de décolorant.<br />
Le décolorant dilué est stable pendant 1 semaine à température ambiante, en flacon fermé.<br />
Éliminer le décolorant dilué s’il y a un changement d’aspect ou apparition d’un trouble dû à une contamination microbienne.<br />
Ne pas ajouter d'azoture de sodium.<br />
En cas de conservation prolongée (au delà d’une semaine) de la solution diluée, ajouter 50 µL/L de ProClin 300 pour prévenir toute prolifération<br />
microbienne.<br />
Le décolorant dilué contenant du ProClin est stable en flacon fermé à température ambiante ou au réfrigérateur jusqu’à la date d’expiration indiquée<br />
sur le kit ou sur l’étiquette du flacon de décolorant.
6. SOLUTION HÉMOLYSANTE<br />
- 3 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Préparation<br />
La solution hémolysante est prête à l’emploi. C’est un tampon avec des composants sans danger aux concentrations utilisées, nécessaires pour des<br />
performances optimales.<br />
Utilisation<br />
Pour l’hémolyse des globules rouges.<br />
Conservation, stabilité et signes de détérioration<br />
La solution hémolysante peut être conservée à température ambiante ou au réfrigérateur. Elle est stable jusqu’à la date d’expiration indiquée sur le<br />
kit ou sur l’étiquette du flacon de solution hémolysante.<br />
Éliminer la solution hémolysante s’il y a un changement d’aspect ou apparition d’un trouble dû à une contamination microbienne.<br />
7. APPLICATEURS<br />
Utilisation<br />
Applicateurs prédécoupés, à usage unique pour le dépôt des échantillons.<br />
Conservation<br />
Les applicateurs doivent être conservés dans un endroit sec à température ambiante ou au réfrigérateur.<br />
8. PAPIERS-FILTRES FINS<br />
Utilisation<br />
Feuilles de papier-filtre, à usage unique pour l’absorption de l’excès de liquide à la surface du gel avant l’application des échantillons.<br />
Conservation<br />
Les papiers-filtres fins doivent être conservés dans un endroit sec à température ambiante ou au réfrigérateur.<br />
RÉACTIFS NÉCESSAIRES NON FOURNIS<br />
1. EAU PHYSIOLOGIQUE<br />
Préparation<br />
Solution de NaCl 0,15 M (9 g/L) dans l’eau distillée ou déminéralisée.<br />
Utilisation<br />
Pour le lavage des globules rouges.<br />
Conservation, stabilité et signes de détérioration<br />
La solution d’eau physiologique peut être conservée à température ambiante ou au réfrigérateur.<br />
Éliminer la solution après 3 mois ou s’il y a un changement d’aspect ou apparition d’un trouble dû à une contamination microbienne. Pour une<br />
conservation prolongée, ajouter 1 g/L d’azoture de sodium.<br />
2. SOLUTION DE FIXATION (facultatif)<br />
Préparation<br />
Au minimum 15 minutes avant l’utilisation, préparer une solution contenant (vol./vol.) : 60 % d’éthanol, 10 % d’acide acétique et 30 % d’eau distillée<br />
ou déminéralisée. Bien mélanger.<br />
Utilisation<br />
Pour la fixation des hémoglobines séparées par électrophorèse en gel d’agarose.<br />
Conservation, stabilité et signes de détérioration<br />
La solution de fixation doit être conservée à température ambiante dans un récipient hermétiquement fermé pour éviter l’évaporation. Éliminer la<br />
solution après 3 mois.<br />
Ne pas fixer plus de 4 gels dans 150 mL de solution de fixation.<br />
ÉQUIPEMENT ET ACCESSOIRES NÉCESSAIRES<br />
1. Générateur de courant : GD 61 D SEBIA, référence N° 1300 ; GD 251 D SEBIA, référence N° 1301 ; MG 300 SEBIA, référence N° 1302 ou<br />
MG 500 SEBIA, référence N° 1303.<br />
2. APPLICATEUR <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA, référence N° 1409, contenant le porte-applicateur <strong>HYDRAGEL</strong> <strong>K20</strong>.<br />
3. Chambre humide, référence N° 1270.<br />
4. Cuve d’électrophorèse : <strong>K20</strong> SEBIA, référence N° 1400.<br />
5. Bacs et portoirs pour le traitement des demi-gels : kit accessoires <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA, référence N° 1420.<br />
6. Pipettes de 5 µL, 10 µL et 200 µL.<br />
7. Incubateur-sécheur : IS 80 SEBIA, référence N° 1430.<br />
8. Densitomètre / scanner capable de lire un film de 82 x 51 mm à 570 nm (filtre jaune) : HYRYS SEBIA, DVSE SEBIA ou scanner équipé du logiciel<br />
PHORESIS SEBIA. Se reporter aux instructions de chaque appareil pour son utilisation et sa calibration.<br />
ÉCHANTILLONS À ANALYSER<br />
Prélèvement et conservation des échantillons<br />
L’analyse se fait sur sangs frais, prélevés sur anticoagulant (EDTA, citrate ou héparine). Éviter les anticoagulants contenant de l'iodoacétate. Les<br />
sangs doivent être prélevés selon la procédure utilisée pour tout test de laboratoire d’analyses cliniques.<br />
Les sangs peuvent être conservés moins de cinq jours au réfrigérateur (entre 2 et 8 °C).
- 4 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Préparation des échantillons<br />
• Agiter le tube primaire avant de prélever le volume de sang total à traiter.<br />
• Centrifuger le sang total, pendant 5 minutes à 5 000 tr/min.<br />
• Éliminer le plasma.<br />
• Laver 2 fois les globules rouges par 10 volumes d’eau physiologique. Les volumes de globules rouges inférieurs à 10 µL doivent être manipulés<br />
avec précaution.<br />
• Éliminer l’excès d’eau physiologique à la surface du culot globulaire lavé, les agiter au vortex avant de prélever les 10 µL à hémolyser.<br />
• Hémolyser 10 µL de globules rouges par 130 µL de solution hémolysante.<br />
• Agiter au vortex pendant 10 secondes puis incuber 5 minutes à température ambiante.<br />
NOTES :<br />
- Pour des sujets anémiés, la quantité de globules rouges hémolysés peut-être augmentée :<br />
- 15 µL pour des sujets moyennement anémiés (environ 0,1 g/mL Hb) ;<br />
- 20 µL pour des sujets fortement anémiés (moins de 0,07 g/mL Hb) ; et 130 µL de solution hémolysante.<br />
L’intensité des fractions sera augmentée sans modifier la proportion de chaque fraction.<br />
- Il n’est pas nécessaire de filtrer ni de centrifuger les hémolysats.<br />
- La solution hémolysante n’affecte pas l’hémoglobine instable Bart.<br />
- En cas de suspicion d’hémoglobine H, il est conseillé de préparer un hémolysat plus concentré, par exemple 10 µL de globules rouges et 30 µL<br />
de solution hémolysante.<br />
TECHNIQUE<br />
I. MIGRATION<br />
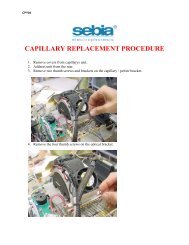
1. Poser le porte-applicateur <strong>HYDRAGEL</strong> <strong>K20</strong> à plat sur la paillasse (Fig. 1) et relever le chariot porte-applicateur.<br />
2. Déposer 120 µL d’eau distillée ou déminéralisée sur le plateau du porte-applicateur dans le tiers inférieur du cadre sérigraphié.<br />
3. Sortir le gel de son emballage.<br />
4. Éliminer rapidement l’excès de liquide en surface, en effleurant le gel avec un papier-filtre fin.<br />
ATTENTION : Ne surtout pas laisser le papier-filtre en contact prolongé avec le gel pour éviter sa déshydratation.<br />
5. Placer le gel (face orientée vers le haut) sur le plateau du porte-applicateur contre la barrette, à l’intérieur du cadre sérigraphié (Fig. 2).<br />
6. Donner une forme concave au gel (Fig. 2) et le dérouler sur le plateau jusqu’au contact de la goutte d’eau qui doit se répartir sur toute la<br />
largeur du gel. Relever légèrement le gel pour éliminer les bulles d’air éventuellement piégées, puis dérouler totalement le gel au contact du<br />
plateau. La goutte d’eau doit s’étaler sous toute la surface du film.<br />
7. Abaisser le chariot porte-applicateur jusqu’en position intermédiaire, la manette située sur le côté du porte-applicateur en position haute.<br />
8. Poser un applicateur à plat sur la paillasse, numérotations (puits) vers le haut (Fig. 3).<br />
9. Déposer 10 µL d’échantillon hémolysé dans chaque puits. Le chargement de l’applicateur ne doit pas excéder 2 minutes.<br />
L’applicateur doit être utilisé immédiatement après le chargement.<br />
Pour un dépôt différé (8 heures maximum), placer l’applicateur dans la chambre humide dents vers le haut (en manipulant l’applicateur par la<br />
protection en plastique), placer la chambre humide au réfrigérateur et ne placer le gel sur le porte-applicateur <strong>HYDRAGEL</strong> <strong>K20</strong> qu’au moment<br />
de l’utilisation.<br />
Voir la notice de la chambre humide pour les instructions d’utilisation.<br />
10. Éliminer la protection des dents de l’applicateur.<br />
11. Placer l'applicateur en position n° 4 sur le porte-applicateur.<br />
IMPORTANT : Les numérotations de l’applicateur sont toujours dirigées vers l'opérateur (Fig. 4).<br />
12. Abaisser le chariot porte-applicateur jusqu’en butée, à l’aide de la manette du porte-applicateur pour amener l’applicateur au contact du gel.<br />
NE PAS FORCER LA DESCENTE DU CHARIOT.<br />
13. Après 1 minute d’application, tourner la manette du porte-applicateur pour relever l’applicateur et le jeter.<br />
14. Placer le gel dans la cuve d’électrophorèse, selon la polarité indiquée sur le gel, bas du gel côté cathodique.<br />
Positionner l’<strong>HYDRAGEL</strong> sur le portoir de la cuve <strong>K20</strong>. La face gel est orientée vers le bas et le gel plonge dans le tampon sur une distance<br />
de 1 cm de chaque côté.<br />
Voir la notice de la cuve <strong>K20</strong> pour les instructions d’utilisation.<br />
15. Brancher la cuve au générateur.<br />
| CONDITIONS DE MIGRATION | SEBIA <strong>K20</strong> |<br />
| Volume de tampon par compartiment | 150 mL |<br />
| Volume total de tampon | 300 mL |<br />
| Temps de migration | 15 minutes |<br />
| Voltage constant | 165 V<br />
|<br />
|<br />
Ampérage de départ (par gel) | 7 ± 2 mA |<br />
16. Après migration, débrancher la cuve et sortir le gel.<br />
II. FIXATION<br />
Elle peut se faire de deux façons : fixation à la chaleur ou à l’aide de la solution de fixation.<br />
Fixation à la chaleur (uniquement avec l’incubateur-sécheur IS 80 SEBIA) :<br />
Sécher le gel sous air chaud à 80 °C dans l’incubateur-sécheur IS 80 jusqu'à séchage complet (pendant 10 minutes minimum).
Fixation avec la solution de fixation :<br />
1. Placer le gel dans un portoir (fourni dans le kit accessoires <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA).<br />
2. Remplir un bac (fourni dans le kit accessoires <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA) avec 150 mL de solution de fixation.<br />
3. Immerger le gel dans la solution de fixation pendant 15 minutes.<br />
4. Sortir le gel et le sécher sous air chaud à 80 °C dans l’incubateur-sécheur.<br />
IMPORTANT : Le gel doit être parfaitement sec.<br />
- 5 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
III. COLORATION - DÉCOLORATION<br />
1. Immerger le gel sec et refroidi dans la solution colorante pendant 5 minutes.<br />
2. Décolorer par trois bains successifs minimum de décolorant jusqu’à obtention d’un fond parfaitement clair.<br />
3. Éliminer l’excès de liquide en surface du gel avec un papier ouaté et sécher le gel sous air chaud à 80 °C. Si nécessaire, nettoyer le dos du<br />
gel (support plastique) avec un papier ouaté humide.<br />
IV. LECTURE<br />
Lire au densitomètre / scanner avec un filtre jaune ou à 570 nm : sur les densitomètres HYRYS ou DVSE, positionner la fraction A 2 sur le repère 5 mm<br />
du plateau de lecture de façon à placer le zéro sur le point le plus bas entre la fraction anhydrase carbonique et la fraction A 2 .<br />
NOTE : Afin d’assurer les résultats les plus exacts et cohérents :<br />
- Ajuster la longueur de lecture à 30 mm de façon à inclure le profil électrophorétique entier.<br />
- Positionner les minima de façon à encadrer au plus près la fraction A 2 .<br />
Il est recommandé d’analyser les profils électrophorétiques le plus rapidement possible. Les gels conservés à l’obscurité, dans un endroit sec et à<br />
l’abri de toute source de chaleur peuvent être interprétés qualitativement dans un délai de trois mois.<br />
RÉSULTATS<br />
Contrôle Qualité<br />
Pour chaque série d’analyses, il est recommandé d’inclure un sang de contrôle ou un échantillon de contrôle contenant des hémoglobines A, F, S<br />
et C.<br />
Valeurs<br />
La lecture à 570 nm par densitométrie permet de définir les concentrations relatives (pourcentages) de chaque fraction.<br />
Les valeurs normales (moyennes ± 2 écarts types) pour chaque fraction dans la technique <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, ont été établies à<br />
partir d’une population de 200 adultes (hommes et femmes), en bonne santé :<br />
Hémoglobine A ≥ 96,5 %<br />
Hémoglobine F < 2,0 % (*)<br />
Hémoglobine A2 ≤ 3,5 %<br />
(*) cf Interférences et limites<br />
Il est recommandé à chaque laboratoire d’établir ses propres valeurs normales.<br />
Interprétation<br />
1. Anomalies qualitatives : Hémoglobinopathies<br />
La plupart sont des anomalies de structure, dues au remplacement par mutation d'un acide aminé par un autre sur l'une ou l'autre chaîne. Les<br />
conséquences de la mutation varient suivant la position de l'acide aminé muté et de celui qui le remplace, l'intégrité de certaines parties de la molécule<br />
étant plus particulièrement nécessaire à sa viabilité et à son bon fonctionnement.<br />
Plus de 200 variants de l'hémoglobine adulte sont actuellement définis et décrits. Les premières hémoglobines anormales étudiées, et les plus<br />
nombreuses, sont dues à une modification de la charge électrique globale de la molécule, entraînant une détection facile par électrophorèse.<br />
Quatre hémoglobines anormales principales présentent un intérêt particulier, d'un point de vue anthropologique et médical : S, C, E et D.<br />
Le kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> est destiné à la détection des hémoglobinopathies et des thalassémies. Dès qu’une anomalie est détectée,<br />
il est conseillé de la confirmer à l’aide de tests complémentaires tels que l’électrophorèse sur gel acide.<br />
Hémoglobine S<br />
La plus fréquente, due à une mutation d’un acide glutamique de la chaîne ß (acide aminé acide) par une valine (acide aminé neutre) : la mobilité est<br />
dans ce cas diminuée. Dans la technique <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, en tampon alcalin, l'hémoglobine S migre en position médiane entre<br />
les fractions A et A 2 .<br />
Hémoglobine C<br />
La mutation est due à un acide glutamique de la chaîne ß, remplacé par une Iysine (acide aminé basique), la mobilité est dans ce cas très réduite.<br />
Dans la technique <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, les hémoglobines C et E se trouvent parfaitement superposées à la fraction A 2 . Quand cette<br />
fraction est supérieure à 15 %, la présence d’hémoglobines C et E peut alors être suspectée.<br />
Hémoglobine E<br />
Un acide glutamique de la chaîne ß est remplacé par une Iysine. Dans la technique <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, cette hémoglobine migre<br />
exactement comme l'hémoglobine C. En tampon acide [technique <strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>], elle ne se sépare pas des<br />
hémoglobines A et A 2 , ce qui permet de la différencier de l’hémoglobine C.<br />
Hémoglobine D<br />
Un acide glutamique de la chaîne ß est remplacé par une glutamine. Dans la technique <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, cette hémoglobine migre<br />
exactement comme l'hémoglobine S. En tampon acide [technique <strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>], elle ne se sépare pas des<br />
hémoglobines A et A 2 , ce qui permet de la différencier de l’hémoglobine S.
- 6 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
2. Anomalies quantitatives : Thalassémies<br />
Elles constituent un groupe assez hétérogène d'affections génétiques caractérisées par la réduction du taux de synthèse d'une ou de plusieurs<br />
chaînes de l'hémoglobine. Le mécanisme de cette réduction à l'échelon moléculaire est encore mal connu.<br />
Il existe différents syndromes thalassémiques :<br />
Les alpha thalassémies<br />
Caractérisées par la diminution de synthèse des chaînes α, affectant par conséquent la synthèse des 3 hémoglobines physiologiques. L'excès de<br />
synthèse des chaînes ß et γ par rapport aux chaînes α provoque la formation de tétramères sans chaîne α :<br />
• hémoglobine Bart = γ 4,<br />
• hémoglobine H = ß 4.<br />
Les bêta thalassémies<br />
Caractérisées par la diminution de synthèse des chaînes ß. Seule la synthèse de l'hémoglobine A est affectée.<br />
Les pourcentages des hémoglobines F et A 2 sont donc augmentés par rapport à l’hémoglobine A.<br />
3. Profils électrophorétiques<br />
Migration des<br />
hémoglobines normales<br />
point d’application<br />
A0 : fraction non glyquée de l’hémoglobine adulte normale A.<br />
A1 : fraction glyquée de l’hémoglobine adulte normale A.<br />
A(A 0 + A 1 ) A (A 0 + A 1 )<br />
F<br />
S - D<br />
A2 A2 - C - E<br />
anhydrase carbonique anhydrase carbonique<br />
Interférences et limites<br />
• Ne pas utiliser d’échantillon hémolysé.<br />
• Lorsque la présence d’une hémoglobine anormale, présentant une mobilité électrophorétique différente de celle des variants majeurs de<br />
l’hémoglobine S, C, D et E, est détectée, il est recommandé d’utiliser d’autres techniques d’identification (par exemple, électrophorèse des chaînes<br />
de globine) ou de consulter un laboratoire spécialisé.<br />
• La mesure quantitative de l’hémoglobine F (Hb F) ou de toute autre hémoglobine mineure migrant à proximité des fractions majeures, est<br />
approximative quand leur concentration représente moins de 2 à 3 % de l’hémoglobine totale.<br />
• Les échantillons de certains patients ayant une hémoglobine S homozygote et traités à l’Hydrea® (hydroxycarbamide) peuvent présenter une<br />
hémoglobine F dont la synthèse a été induite par ce traitement. Sur quelques cas observés, cette hémoglobine F induite a une mobilité sur les gels<br />
<strong>HYDRAGEL</strong> 7 <strong>HEMOGLOBIN</strong>(E) légèrement différente de celle de l’hémoglobine F native.<br />
• Sur certains échantillons conservés plus de 7 jours, il peut être observé une focalisation de la traînée située derrière la fraction Hb A, cette<br />
focalisation ne doit pas être confondue avec un variant de l’hémoglobine (tel que les hémoglobines H ou Bart).<br />
Assistance technique<br />
Contacter le Service Technique SEBIA en cas de test défectueux.<br />
Les fiches de données de sécurité des différents réactifs du kit ainsi que les informations relatives à l’élimination des déchets sont disponibles auprès<br />
du Service Technique SEBIA.<br />
PERFORMANCES<br />
Migration des hémoglobines<br />
anormales majeures<br />
Toutes les mesures densitométriques ont été effectuées à l’aide du densitomètre HYRYS SEBIA. De plus, les profils électrophorétiques ont été<br />
interprétés qualitativement à l’oeil nu. Les résultats suivants obtenus par analyse quantitative indiquent une très bonne répétabilité et reproductibilité<br />
du kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> pour tous les aspects testés, avec un coefficient de variation moyen de 2,2 %.<br />
Reproductibilté intra-essai<br />
Trois échantillons de sang (un échantillon normal, un échantillon à Hb A2 élevée et un échantillon à Hb C) ont été analysés en répétabilité dans la<br />
technique <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> sur des gels d’un même lot. Les profils électrophorétiques ont été analysés par densitométrie et le<br />
tableau suivant présente les valeurs moyennes (en %), écart-types (ET) et coefficients de variation (CV) obtenus pour chaque fraction de<br />
l’hémoglobine de ces 3 échantillons.<br />
NOTE : Quel que soit l’échantillon, aucune discordance n’a été mise en évidence :<br />
- Échantillon à taux normal en Hb A2 : toutes les valeurs sont normales ;<br />
- Échantillons à taux élevés en Hb A2 et Hb C : toutes les valeurs sont élevées<br />
| FRACTION Hb | MOYENNE | ET | CV (%) |<br />
| Sang normal |<br />
| Hb A | 97,4 | 0,1 | 0,1 |<br />
| Hb A | 2 2,6 | 0,1 | 5,3 |<br />
| Sang à Hb A2 élevée |<br />
| Hb A | 95,2 | 0,2 | 0,2 |<br />
| Hb A | 2 4,8 | 0,2 | 4,4 |<br />
| Sang à Hb C élevée |<br />
| Hb A | 56,7 | 0,4 | 0,8 |<br />
| Hb C | 43,3 | 0,4 | 1,0 |
- 7 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Reproductibilté inter-essais<br />
Des échantillons de sang ont été analysés dans la technique <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> sur 10 gels d’un même lot.<br />
Parmi les échantillons analysés, se trouvaient 7 échantillons avec hémoglobines anormales (Hb S, Hb F ou Hb C), 2 échantillons avec un taux d’Hb A 2<br />
élevé, les autres échantillons étant normaux. Les valeurs moyennes (en %), écart-types (ET) et coefficients de variation (CV) ont été déterminés pour<br />
chaque fraction de l’hémoglobine des échantillons. Le tableau suivant présente les limites des valeurs moyennes, ET et CV, ainsi que le CV moyen<br />
représentant l’ensemble de chaque fraction.<br />
NOTE : Quel que soit l’échantillon, aucune discordance n’a été mise en évidence :<br />
- Échantillons à taux normal en Hb A 2 : toutes les valeurs sont normales ;<br />
- Échantillons à taux élevés en Hb A 2 : toutes les valeurs sont élevées.<br />
| FRACTION Hb | MOYENNE | ET | CV (%) | CV MOYEN (%) |<br />
| Hb A | 18,0 - 97,8 | 0,1 - 1,0 | 0,1 - 4,0 | 0,8 |<br />
| Hb F | 13,3 - 76,3 | 0,5 - 0,6 | 0,7 - 3,4 | 1,8 |<br />
| Hb C | 21,5 - 43,5 | 0,2 - 0,3 | 0,6 - 1,1 | 0,8 |<br />
| Hb S/D | 9,7 - 84,1 | 0,1 - 0,6 | 0,4 - 2,6 | 1,1<br />
| |<br />
Hb A | 2 2,2 - 5,7 | 0,1 - 0,2 | 2,3 - 7,6 | 4,0 |<br />
Exactitude - Détection d’hémoglobines anormales<br />
Soixante trois échantillons de sang ont été analysés dans la technique <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> et sur un autre système en gel d’agarose<br />
disponible dans le commerce. Ces échantillons, accompagnés de leur diagnostic clinique établi par électrophorèses sur gel alcalin et sur gel acide<br />
et/ou par HPLC, ont été fournis par un centre hospitalier. Les résultats obtenus ont montré une parfaite corrélation entre les deux systèmes avec, pour<br />
la détection des hémoglobines anormales, une sensibilité de 100 % et une spécificité de 100 % par rapport à la technique de référence, calculées<br />
selon la méthode recommandée (Wendling, 1986). En effet, toutes les hémoglobines anormales ainsi que les taux anormaux d’hémoglobines<br />
normales ont été détectés dans la technique <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> en accord avec le second système de comparaison sur gel, les<br />
résultats hospitaliers et le diagnostic clinique. Quel que soit l’échantillon, aucune discordance entre les techniques n’a été mise en évidence, telle que<br />
la présence de faux positifs (détection d’une Hb anormale inexistante ou d’une Hb à taux normal détectée à un taux anormal).<br />
Exactitude - Détermination quantitative d’Hb A 2<br />
Cinquante et un échantillons de sang présentant des taux normaux ou élevés d’Hb A 2 ont été analysés en parallèle dans la technique <strong>HYDRAGEL</strong><br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> et sur un autre système en gel d’agarose disponible dans le commerce, avec densitométrie des profils électrophorétiques<br />
obtenus.<br />
La corrélation entre ces deux techniques sur le taux d’Hb A 2 a été déterminée à l’aide d’outils statistiques : moyenne et coefficient de régression<br />
linéaire. Les paramètres de corrélation entre ces 2 systèmes d’analyse (y = <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>) sont présentés dans le tableau cidessous.<br />
| Coefficient de Corrélation | Intersection-y | Pente | Limites des valeurs de % |<br />
| | | | (système SEBIA) |<br />
| 0,973 | -0,344 | 0,963 | 1,5 - 5,7 |<br />
BIBLIOGRAPHIE<br />
1. Fairbanks V.F., ed. (1980) Hemoglobinopathies and thalassemia: Laboratory methods and case studies. Brian C. Decker, New York.<br />
2. Galacteros F. (1986) Thalassémie, drépanocytose et autres hémoglobinopathies. Techniques et Biologie, 3, 174-178.<br />
3. Huisman T.H.J. and. Jonxis J.H.P (1977) The hemoglobinopathies: techniques of identification. Marcel Dekker, New York.<br />
4. Krauss J.S., Drew P.A., Jonah M.H., Trinh M., Shell S., Black L. and Baisden C.R. (1986) Densitometry and microchromatography compared for<br />
determination of the hemoglobin C and A 2 proportions in hemoglobin C and hemoglobin SC disease and in hemoglobin C trait. Clin. Chem. 32, 5,<br />
860-863.<br />
5. Livingstone C. (1986) The hemoglobinopathies. Edit. London.<br />
6. Maier-Redelsberger M., Girot R. (1989) Diagnostic biologique des maladies de l’hémoglobine. Feuillets de biologie, 170.<br />
7. Schneider R.G. (1978) Methods for detection of hemoglobin variants and hemoglobinopathies in the routine clinical laboratory. CRC Crit. Rev. Clin.<br />
Lab. Sci. 9, 243-271.<br />
8. Vovan L., Lara-Russo D., Orsini A. (1985) Diagnostic biologique des hémoglobinoses. Ann. Pédiat. 32, 9, 780-789.<br />
9. Wendling A. Procédures de diagnostic ou de dépistage : Justification et validité d’un test de diagnostic ou de dépistage-sensibilité-spécificité.<br />
Impact-Internat, 1986 ; Sept : 93-97.
INTENDED USE<br />
- 8 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
The <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> kit is designed for separation of the normal hemoglobins (A and A 2 ) and for the detection of the major<br />
hemoglobin variants: S or D and C or E, by electrophoresis on alkaline agarose gels. The resulting electrophoregrams are evaluated visually for pattern<br />
abnormalities. Densitometry can serve as an aid in the interpretation by providing relative concentrations of individual fractions. <strong>Electrophoresis</strong> on<br />
acidic gel, e.g., <strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure, should follow to confirm the identification of hemoglobin variants, in particular,<br />
to differentiate hemoglobins S from D and E from C.<br />
Each agarose gel in the <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> kit is intended to run 7 samples.<br />
For In Vitro Diagnostic Use.<br />
PRINCIPLE OF THE TEST<br />
Hemoglobin is a complex molecule composed of two pairs of polypeptide chains. Each chain is linked to the heme, a tetrapyrrolic nucleus (porphyrin)<br />
which chelates an iron atom. The heme part is common to all hemoglobins and their variants. The type of hemoglobin is determined by the protein<br />
part called globin. Polypeptide chains α, ß, δ and γ constitute the normal human hemoglobins:<br />
• hemoglobin A ..................................... = α 2 ß 2<br />
• hemoglobin A 2 .................................... = α 2 δ 2<br />
• fetal hemoglobin F ............................. = α 2 γ 2<br />
The α-chain is common to these three hemoglobins.<br />
The hemoglobin spatial structure and other molecular properties (as that of all proteins) depend on the nature and the sequence of the amino acids<br />
forming the chains. Substitution of amino acids by mutation is responsible for formation of hemoglobin variants which have different surface charge<br />
and consequently different electrophoretic mobilities, which also depend on the pH and ionic strength of the buffer.<br />
The resulting qualitative (or structural) abnormalities are called hemoglobinopathies. Decreased synthesis of one of the hemoglobin chains leads to<br />
quantitative (or regulation) abnormalities, called thalassemias.<br />
The assay is performed on hemolyzed washed red blood cells. The hemoglobins are separated by electrophoresis on alkaline gels and the fractions<br />
are visualized by staining with amidoblack. The dried gels are ready for interpretation.<br />
REAGENTS AND MATERIALS SUPPLIED IN THE <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> KIT<br />
| ITEMS | PN 3010 |<br />
| Agarose Gels (ready to use) | 10 gels |<br />
| Tris-Barbital Buffer (stock solution) | 3 vials, 75 mL each |<br />
| Staining solution diluent (stock solution) | 1 vial, 60 mL |<br />
| Amidoblack Stain (stock solution) | 1 vial, 20 mL |<br />
| Destaining Solution (stock solution) | 1 vial, 100 mL |<br />
| Hemolysing solution (ready to use) | 1 vial, 20 mL |<br />
| Applicators 7 teeth (ready to use) | 1 pack of 10<br />
| |<br />
Filter Papers -Thin | 1 pack of 10 |<br />
FOR OPTIMAL RESULTS<br />
All reagents from the same kit must be always used together and according to the package insert instructions.<br />
PLEASE READ THE PACKAGE INSERT CAREFULLY.<br />
1. AGAROSE GELS<br />
Preparation<br />
Agarose gels are ready to use. Each gel contains: agarose, 0.8 g/dL ; alkaline buffer pH 8.5 ± 0.1 ; additives, nonhazardous at concentrations used,<br />
necessary for optimum performance.<br />
Use<br />
Support medium for hemoglobin electrophoresis.<br />
Storage, stability and signs of deterioration<br />
Store the gels horizontally in the original protective packaging at room temperature (15 to 30 °C) or refrigerated (2 to 8 °C). (The arrow on the front of<br />
the kit box must be pointing upwards). Avoid obvious temperature fluctuations during storage (e.g., do not store close to a window or a heat source).<br />
The gels are stable until the expiration date indicated on the kit package or the gel package labels.<br />
DO NOT FREEZE.<br />
Discard gel when:<br />
(i) crystals or precipitate form on the gel surface or the gel texture becomes very soft (all these result from freezing the gel),<br />
(ii) bacterial or mold growth is indicated,<br />
(iii) abnormal liquid quantity is present in the gel box (as a result of buffer exudation from the gel due to improper storage conditions).<br />
2. TRIS-BARBITAL BUFFER<br />
Preparation<br />
Each vial of the stock buffer solution to be diluted up to 1 liter with distilled or deionized water.<br />
After dilution, the working solution contains : tris-barbital pH 9.2 ± 0.3 ; sodium azide.<br />
WARNING: Each vial of the stock buffer contains 2.45 % barbital, 13.73 % sodium barbital and 0.13 % sodium azide. Do not ingest ! If<br />
ingested, consult physician immediately ! Prevent contact with acids, lead or copper, as these are known to form explosive or toxic<br />
compounds with sodium azide. Always flush with a large quantity of water when disposing.<br />
SEBIA INSTRUCTIONS - English
- 9 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Use<br />
<strong>Electrophoresis</strong> buffer.<br />
Storage, stability and signs of deterioration<br />
Store stock buffer solution at room temperature or refrigerated. Stock solution is stable for several years, at least until the expiration date indicated on<br />
the kit package or buffer vial labels. Diluted buffer solution is stable for one year at room temperature in a closed bottle.<br />
Discard diluted buffer if it changes its appearance, e.g., becomes cloudy due to microbial contamination.<br />
3. STAINING SOLUTION DILUENT<br />
Preparation<br />
The stock staining solution diluent must be used as described in paragraph " AMIDOBLACK STAIN ".<br />
It contains an acidic solution.<br />
Use<br />
For the preparation of the amidoblack staining solution.<br />
Storage, stability and signs of deterioration<br />
Store the stock staining solution diluent at room temperature or refrigerated. It is stable until the expiration date indicated on the kit package or staining<br />
solution diluent vial labels. DO NOT FREEZE.<br />
Do not add any sodium azide.<br />
4. AMIDOBLACK STAIN<br />
Preparation<br />
The amidoblack concentrated stain is a visquous solution which may gelify. The integrity of the stock staining solution is not altered by the increase in<br />
viscosity or solidification.<br />
In all cases, to obtain a perfect reconstitution of the stain, we advise you to respect the following procedure:<br />
1. Add 15 mL of stain diluent to the concentrated amidoblack vial.<br />
2. Close carefully the vial.<br />
3. Shake very vigorously the vial during approximately 5 seconds.<br />
4. Pour this solution in the container for staining solution processing.<br />
5. Repeat this step twice, three times if necessary.<br />
6. Pour the remaining diluent in the container and complete the volume to 300 mL with distilled or deionized water.<br />
7. Mix contents of stain cubitainer well for 5 to 10 minutes.<br />
The staining solution is ready to use.<br />
After dilution, the working staining solution contains: acid solution pH ≈ 2 ; amidoblack, 0.4 g/dL ; ethylene-glycol, 6.7 % ; additives, nonhazardous at<br />
concentrations used, necessary for optimum performance.<br />
WARNING: Harmful if swallowed.<br />
Use<br />
For staining gels with electrophoretic protein separations.<br />
IMPORTANT : The staining solution is designed to stain only 10 gels. Change the solution after 10 staining steps.<br />
Storage, stability and signs of deterioration<br />
Store both stock and working staining solutions at room temperature or refrigerated in closed containers to prevent evaporation. Stock staining solution<br />
is stable until the expiration date indicated on the kit package or staining vial labels.<br />
Working staining solution is stable for 1 month.<br />
Do not store the working staining solution close to a heat source.<br />
5. DESTAINING SOLUTION<br />
Preparation<br />
Each vial of stock destaining solution to be diluted up to 100 liters with distilled or deionized water. It is convenient to dilute only 1 mL of the stock<br />
solution to 1 liter. After dilution, the working destaining solution contains: citric acid, 0.05 g/dL.<br />
Use<br />
For destaining, that is removal of excess and background stain from the gels.<br />
Storage, stability and signs of deterioration<br />
Store the stock destaining solution at room temperature or refrigerated. It is stable until the expiration date indicated on the kit package or destaining<br />
solution vial labels. Working destaining solution is stable for one week at room temperature in a closed bottle.<br />
Discard working destaining solution if it changes its appearance, e.g., becomes cloudy due to microbial contamination.<br />
Do not add any sodium azide.<br />
To prevent microbial proliferation in the diluted destaining solution to be stored more than one week, add 5 µL/dL of ProClin 300.<br />
Working destaining solution added with ProClin is stable in a closed bottle at room temperature or refrigerated until the expiration date indicated on<br />
the kit package or destaining solution vial labels.<br />
6. HEMOLYZING SOLUTION<br />
Preparation<br />
Hemolyzing Solution is ready to use. It is a buffer with additives, nonhazardous at the concentration used, necessary for optimum performance.<br />
Use<br />
To hemolyze red blood cells.<br />
Storage, stability and signs of deterioration<br />
Store Hemolyzing Solution at room temperature or refrigerated. It is stable until the expiration date indicated on the kit package or Hemolyzing Solution<br />
vial label.<br />
Discard Hemolyzing Solution if it changes its appearance, e.g., becomes cloudy due to microbial contamination.<br />
7. APPLICATORS<br />
Use<br />
Precut, single use applicators for sample application.
Storage<br />
Store the applicators in a dry place at room temperature or refrigerated.<br />
8. FILTER PAPERS - THIN<br />
Use<br />
Single use, thin absorbent paper pads for blotting excessive moisture off the gel surface before sample application.<br />
Storage<br />
Store the thin filter papers in a dry place at room temperature or refrigerated.<br />
REAGENTS REQUIRED BUT NOT SUPPLIED<br />
- 10 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
1. SALINE<br />
Preparation<br />
Make 0.15 M (0.9 g/dL) NaCl solution in distilled or deionized water.<br />
Use<br />
To wash red blood cells.<br />
Storage, stability and signs of deterioration<br />
Store saline at room temperature or refrigerated. Discard after 3 months or if it changes its appearance, e.g., becomes cloudy due to microbial<br />
contamination. For longer storage periods, add sodium azide, 0.1 g/dL.<br />
2. FIXATIVE SOLUTION (optional)<br />
Preparation<br />
At least 15 minutes before use, prepare a solution containing (vol. / vol.): 60 % ethanol ; 10 % acetic acid and 30 % distilled or deionized water.<br />
Mix well.<br />
Use<br />
To fix electrophoretic hemoglobin separations in agarose gel plates.<br />
Storage, stability and signs of deterioration<br />
Store fixative solution at room temperature tightly capped to prevent evaporation. Discard after 3 months. Do not fix more than 4 gels in each 150 mL<br />
of fixative solution.<br />
EQUIPMENT AND ACCESSORIES REQUIRED BUT NOT SUPPLIED<br />
1. Power supply: GD 61 D SEBIA, PN 1300 ; GD 251 D SEBIA, PN 1301 ; MG 300 SEBIA, PN 1302 or MG 500 SEBIA, PN 1303.<br />
2. <strong>HYDRAGEL</strong> <strong>K20</strong> APPLICATOR SEBIA, PN 1409, containing the <strong>HYDRAGEL</strong> <strong>K20</strong> applicator carrier.<br />
3. Wet Storage Chamber, PN 1270.<br />
4. <strong>Electrophoresis</strong> chamber: <strong>K20</strong> SEBIA, PN 1400.<br />
5. Tanks and Gel Holders for processing of gel plates: <strong>HYDRAGEL</strong> <strong>K20</strong> Accessory Kit SEBIA, PN 1420.<br />
6. Pipettes: 5 µL, 10 µL and 200 µL.<br />
7. Incubator-Dryer: IS 80 SEBIA, PN 1430.<br />
8. Densitometer / flat-bed scanner able to scan 82 x 51 mm gel plates at 570 nm (yellow filter) : HYRYS SEBIA, DVSE SEBIA or PHORESIS software<br />
for flat-bed scanner. Refer to manufacturer’s instructions for operation and calibration procedures.<br />
SAMPLES FOR ANALYSIS<br />
Sample collection and storage<br />
Fresh anticoagulated blood samples are recommended for analysis. Common anticoagulants such as those containing EDTA, citrate or heparin are<br />
acceptable ; avoid those with iodoacetate. Blood must be collected according to established procedures used in clinical laboratory testing. If needed,<br />
store samples at 2 to 8 °C for up to 5 days.<br />
Sample preparation<br />
• Mix the collection tube before taking the blood to prepare.<br />
• Centrifuge anticoagulated blood at 5 000 rpm for 5 minutes.<br />
• Discard the plasma.<br />
• Wash the red blood cells 2 times with 10 volumes of saline ; great care must be taken when processing volumes of red blood cells smaller than<br />
10 µL.<br />
• Discard the excess of saline over the red blood cells pellet and vortex them before taking 10 µL to hemolyze.<br />
• Hemolyze 10 µL packed red cells with 130 µL Hemolyzing Solution.<br />
• Vortex for 10 seconds and incubate 5 minutes at room temperature.<br />
NOTES:<br />
- To prepare hemolysate from subjects, mildly anemic (approximately 10 g/dL Hb) or severely anemic (< 7 g/dL Hb), the volume of packed<br />
RBC may be increased to 15 µL and 20 µL, respectively. The staining intensity will thus increase but relative concentrations of individual<br />
fractions will not change.<br />
- The hemolyzate need not be filtered or centrifuged.<br />
- The SEBIA’s hemolyzing solution does not affect the unstable hemoglobin Bart’s.
PROCEDURE<br />
- 11 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
I. MIGRATION STEP<br />
1. Place the <strong>HYDRAGEL</strong> <strong>K20</strong> applicator carrier on a flat surface (Fig. 1) and raise the part of the applicator carrier with the numbered notches.<br />
2. Pool 120 µL distilled or deionized water on the lower third of the frame printed on the <strong>HYDRAGEL</strong> <strong>K20</strong> applicator carrier.<br />
3. Unpack the <strong>HYDRAGEL</strong> agarose gel plate.<br />
4. Roll quickly and uniformly one thin filter paper onto the gel surface to absorb the excess of liquid. Remove the paper immediately.<br />
WARNING: Do not leave the filter paper for a too long contact with the gel to avoid its dehydration.<br />
5. Place the gel plate (the gel side up) with its edge against the stop at the bottom of the printed frame (Fig. 2).<br />
6. Bend the gel and lower it down onto the water pool (Fig. 2). Ensure that no air bubbles are trapped, water is spread underneath the entire gel<br />
plate and the gel is lined up with the printed frame.<br />
7. Lower the applicator carrier with the numbered notches down to the intermediate position with the switch in high position.<br />
8. Place one applicator on a flat surface with the well numbers in the right-side-up position (Fig. 3).<br />
9. Apply 10 µL of hemolyzed sample into the applicator wells. Load the applicator within 2 minutes.<br />
- Use the applicator without any delay.<br />
- For later use (up to 8 hours), place the applicator into the wet storage chamber with the teeth up [handle it by the plastic tooth protection<br />
frame], keep the entire chamber under refrigeration and set-up the gel plate onto the <strong>HYDRAGEL</strong> <strong>K20</strong> applicator carrier just before use.<br />
See wet chamber package insert for further details.<br />
10. Snap off the applicator teeth's protection frame.<br />
11. Place the sample applicator into position No. 4 on the applicator carrier.<br />
IMPORTANT: The numbers printed on the sample applicator must face the operator (Fig. 4).<br />
12. Lower the applicator carrier with the switch so that the applicator contacts the gel surface. DO NOT FORCE THE CARRIERS ALL THE WAY<br />
DOWN.<br />
13. After 1 minute, turn the switch to rise up the applicator, remove the applicator and discard.<br />
14. Put the gel into an appropriate electrophoresis chamber, according to the polarity indicated on the gel, the lower side of the gel on the cathodic<br />
side.<br />
When using SEBIA <strong>K20</strong> chamber, place the <strong>HYDRAGEL</strong> on the bridge with the gel side facing down ; the gel should dip about 1 cm into the<br />
buffer on each side.<br />
See <strong>K20</strong> chamber package insert for further details.<br />
15. Plug the chamber to the power supply.<br />
| MIGRATION CONDITIONS | SEBIA <strong>K20</strong> |<br />
| Volume of buffer per compartment | 150 mL |<br />
| Total buffer volume | 300 mL |<br />
| Migration time | 15 minutes |<br />
| Constant voltage | 165 V<br />
|<br />
|<br />
Initial current (per gel) | 7 ± 2 mA |<br />
16. After migration, unplug the chamber and remove the gel plate.<br />
II. FIXATION<br />
Process gels according to one of the following procedures.<br />
Hot air fixation (recommended only with SEBIA IS 80 Incubator-Dryer) :<br />
Dry the gel completely in the incubator-dryer at 80 °C (for 10 minutes minimum).<br />
Fixation with fixative solution :<br />
1. Place the gel into a gel holder (supplied with SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong> Accessory Kit) for further processing.<br />
2. Fill one tank (supplied with SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong> Accessory Kit) with 150 mL of fixative solution.<br />
3. Immerse the gel in the fixative solution for 15 minutes.<br />
4. Remove the gel and dry it with hot 80 °C air flow in incubator-dryer IS 80.<br />
IMPORTANT : The gel must be perfectly dry.<br />
III. STAINING - DESTAINING<br />
1. Immerse the dried and cooled gel in the staining solution for 5 minutes.<br />
2. Destain in three successive baths of destaining solution until the background is completely colorless and clear.<br />
3. Soak up excess liquid on the gel surface with a tissue paper and dry the gel with hot 80 °C air. If needed, clean the back side (the plastic<br />
support side) of the dry film with a wet tissue paper.<br />
IV. SCANNING<br />
Scan using a densitometer / scanner at 570 nm or with a yellow filter. When using HYRYS or DVSE, densitometers, position the A 2 fraction on the<br />
5 mm mark of the scanning plate: the background zero is made between the A 2 and carbonic anhydrase fractions at the lowest point.<br />
NOTE : To assure the most accurate and consistent results, do the following:<br />
- Adjust the scan length to include the entire electrophoretic pattern (≈ 30 mm).<br />
- Make sure the minima on both sides of A 2 fraction are positioned at the very feet of the A 2 peak.<br />
It is a good practice to read the stained gels without delay. For future reference, they can be stored in a protective cover in a dry, dark place away from<br />
sources of heat and visually interpreted within at least 3 months.
RESULTS<br />
- 12 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Quality Control<br />
It is advised to include an assayed control blood or assayed blood sample containing hemoglobins A, F, C and S into each run of samples.<br />
Values<br />
Densitometer scanning of stained electrophoregrams yields relative concentrations (percentages) of individual hemoglobin zones.<br />
Normal values (mean ± 2 SD) using <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure have been established from a healthy population of 200 adults<br />
(men and women):<br />
Hemoglobin A ≥ 96.5 %<br />
Hemoglobin F < 2.0 % (*)<br />
Hemoglobin A2 ≤ 3.5 %<br />
(*) see Interference and Limitations<br />
It is recommended each laboratory establishes its own normal values.<br />
Interpretation<br />
1. Qualitative abnormalities: Hemoglobinopathies<br />
Most hemoglobinopathies are due to substitution by mutation of a single amino acid in one of the four types of polypeptide chains. The clinical<br />
significance of such a change depends on the type of amino acid and the site involved. In clinically significant disease, either the α-chain or the<br />
ß-chain is affected (even γ chains).<br />
More than 200 variants of adult hemoglobin have been described. The first abnormal hemoglobins studied and the most frequently occuring have an<br />
altered net electric charge, leading to an easy detection by electrophoresis.<br />
There are four main abnormal hemoglobins which present a particular clinical interest: S, C, E and D.<br />
The <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> kits are intended for the preliminary identification of hemoglobinopathies and thalassemias. Once an<br />
abnormal pattern is indicated, its identity should be confirmed by appropriate discriminatory tests (e.g., electrophoresis on acidic agarose gels).<br />
Hemoglobin S<br />
Hemoglobin S is the most frequent. It is due to the replacement of one glutamic acid (an acidic amino acid) of the ß-chain by valine (a neutral amino<br />
acid). Its electrophoretic mobility is therefore slowed down. On alkaline buffered gels, <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, hemoglobin S migrates<br />
between A and A 2 fractions.<br />
Hemoglobin C<br />
One glutamic acid of the ß-chain is replaced by lysine (a basic amino acid): its mobility is strongly reduced. With <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong><br />
procedure, C, E and A 2 are superimposed. When this fraction is > 15 %, hemoglobins C and E must be suspected.<br />
Hemoglobin E<br />
One glutamic acid of the ß-chain is replaced by lysine: hemoglobin E migrates exactly like hemoglobin C using <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong><br />
procedure. Unlike hemoglobin C, it does not separate from hemoglobin A in acidic buffer [<strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>]. This property<br />
allows to differentiate E and C.<br />
Hemoglobin D<br />
One glutamic acid of the ß-chain is replaced by glutamine. With <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure, this hemoglobin migrates exactly like<br />
hemoglobin S. Hemoglobin D does not separate from hemoglobin A in acidic buffer [<strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>] ; this property allows<br />
to differenciate S and D.<br />
2. Quantitative abnormalities: Thalassemias<br />
Thalassemias constitute a quite heterogeneous group of genetic disorders characterized by decreased synthesis of one or several types of the<br />
polypeptide chains. The molecular mechanism of this decrease has not been fully described.<br />
There are two types of thalassemia syndromes:<br />
Alpha-thalassemias<br />
They are characterized by the decrease of synthesis of the α-chains, consequently affecting the synthesis of all normal hemoglobins.<br />
The excess of synthesis of the ß- and γ-chains in relation to α-chains chains induces the formation of tetrameres without any α-chain:<br />
• hemoglobin Bart = γ 4,<br />
• hemoglobin H = ß 4.<br />
Beta-thalassemias<br />
They are characterized by the decrease of synthesis of the ß-chains. Only hemoglobin A synthesis is affected.<br />
Therefore hemoglobin F and hemoglobin A 2 percentages are increased with respect to hemoglobin A.<br />
3. Migration patterns<br />
Migration of normal<br />
hemoglobins<br />
A(A0 + A1 ) A (A0 + A1 )<br />
F<br />
S - D<br />
A2 A2 - C - E<br />
carbonic anhydrase carbonic anhydrase<br />
application point<br />
A0 : The non-glycated fraction of the normal adult hemoglobin A.<br />
A1 : The glycated fraction of the normal adult hemoglobin A.<br />
In the above patterns, the cathode is at the bottom the anode at the top.<br />
Migration of major abnormal<br />
hemoglobins
- 13 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Interference and Limitations<br />
• Do not use hemolyzed blood samples.<br />
• When an abnormal hemoglobin is detected, which behaves differently than the major hemoglobin variants S, C, D and E, use other means of<br />
identification (e.g., isoelectric focusing, globin chain electrophoresis), or consult or send sample to a specialized laboratory.<br />
• The densitometric assay of Hb F (or of any other minor hemoglobin that migrates in the proximity of major fractions) is semi-quantitative as the<br />
values become inaccurate at below 2 % - 3 % of the total hemoglobin.<br />
• Some homozygous "S" subjects receive a "Hydrea"® (hydroxyurea) treatment that can induce synthesis of foetal hemoglobin. The mobility of the<br />
induced hemoglobin F on <strong>HYDRAGEL</strong> 7 <strong>HEMOGLOBIN</strong>(E) has been observed in some cases slightly different from the physiological hemoglobin F.<br />
• On samples stored more than 7 days, the smear located behind the Hb A fraction may become a concentrated fraction, do not interpret this fraction<br />
as an hemoglobin variant, e.g., H or Bart hemoglobins.<br />
Troubleshooting<br />
Call Technical Service of the supplier when the test fails to perform while the instruction for the preparation and storage of materials, and for the<br />
procedure were carefully followed.<br />
Kit reagent Safety Data Sheets and informations on waste products elimination are available from the Technical Service of the supplier.<br />
PERFORMANCE DATA<br />
All performance data are based on a study that included SEBIA <strong>HYDRAGEL</strong> materials and instruments compared to a commercially available agarose<br />
gel system. In addition, concordance studies were performed where the identity of hemoglobins and their values were established by other recognized<br />
methodologies. The results of representative examples of the performance studies are presented here.<br />
All electrophoregrams were interpreted visually. SEBIA’s HYRYS densitometer was used for all densitometric evaluations to complement the visual<br />
data as appropriate.<br />
Reproducibility Within Run<br />
Three blood samples were electrophoresed using <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure on gels from the same lot. Each sample was run in<br />
all the tracks of a single gel. The following table shows the means, SD and CV for each individual hemoglobin component in the three samples<br />
calculated from the densitometric per cent values for each track. In addition, none of the repeats showed false positive or false negative values.<br />
| COMPONENT | MEAN | SD | CV (%) |<br />
| Normal blood |<br />
| Hb A | 97.4 | 0.1 | 0.1 |<br />
| Hb A | 2 2.6 | 0.1 | 5.3 |<br />
| Elevated Hb A2 |<br />
| Hb A | 95.2 | 0.2 | 0.2 |<br />
| Hb A | 2 4.8 | 0.2 | 4.4 |<br />
| Elevated Hb C |<br />
| Hb A | 56.7 | 0.4 | 0.8 |<br />
| Hb C | 43.3 | 0.4 | 1.0 |<br />
Reproducibility In Between Runs<br />
Blood samples were electrophoresed using <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure on gels from a single lot. The samples analyzed included<br />
seven samples with an abnormal hemoglobin (Hb S, Hb F or Hb C), two samples with elevated Hb A 2 and the rest were normal blood samples. The<br />
means, SD and CV were calculated from the data obtained for each component in each sample. Ranges of the means, SD and CV, and the mean CV<br />
representing the pool of individual components are tabulated below. In addition, none of the repeats showed false positive or false negative values.<br />
| COMPONENT | MEAN | SD | CV (%) | MEAN CV (%) |<br />
| Hb A | 18.0 – 97.8 | 0.1 – 1.0 | 0.1 – 4.0 | 0.8 |<br />
| Hb F | 13.3 – 76.3 | 0.5 – 0.6 | 0.7 – 3.4 | 1.8 |<br />
| Hb C | 21.5 – 43.5 | 0.2 – 0.3 | 0.6 – 1.1 | 0.8 |<br />
| Hb S/D | 9.7 – 84.1 | 0.1 – 0.6 | 0.4 – 2.6 | 1.1<br />
| |<br />
Hb A | 2 2.2 – 5.7 | 0.1 – 0.2 | 2.3 – 7.6 | 4.0 |<br />
Accuracy - Detection of Hemoglobin Abnormalities<br />
Sixty three different blood samples were analyzed using <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure and another commercially available agarose<br />
gel system. The blood samples and their diagnostic assessment were provided by a hospital. The diagnosis was based on a routine alkaline gel and<br />
acid gel electrophoresis and/or HPLC. All abnormal hemoglobins or abnormal levels of normal hemoglobins detected with <strong>HYDRAGEL</strong><br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure were in agreement with the comparative gel system, hospital results and clinical diagnosis. There were no case<br />
observed of false positive, i.e., detection of an abnormal band or abnormal level of a normal band where no such abnormality existed.<br />
Accuracy - Quantitative Determination of Hb A 2<br />
The levels of Hb A 2 were measured in 51 blood samples with normal and elevated levels of Hb A 2 both by densitometry of the electrophoretic<br />
separations obtained using <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure. The measured values from both procedures were analyzed by a linear<br />
regression statistical procedure. The results of linear regression analysis are tabulated below (y = <strong>HYDRAGEL</strong>).<br />
| Correlation Coefficient | y-Intercept | Slope | Range of % Values |<br />
| | | | (SEBIA’s system) |<br />
| 0.973 | -0.344 | 0.963 | 1.5 – 5.7 |
BIBLIOGRAPHY<br />
- 14 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
1. Fairbanks V.F., ed. (1980) Hemoglobinopathies and thalassemia: Laboratory methods and case studies. Brian C. Decker, New York.<br />
2. Galacteros F. (1986) Thalassémie, drépanocytose et autres hémoglobinopathies. Techniques et Biologie, 3, 174-178.<br />
3. Huisman T.H.J. and. Jonxis J.H.P (1977) The hemoglobinopathies: techniques of identification. Marcel Dekker, New York.<br />
4. Krauss J.S., Drew P.A., Jonah M.H., Trinh M., Shell S., Black L. and Baisden C.R. (1986) Densitometry and microchromatography compared for<br />
determination of the hemoglobin C and A 2 proportions in hemoglobin C and hemoglobin SC disease and in hemoglobin C trait. Clin. Chem. 32, 5,<br />
860-863.<br />
5. Livingstone C. (1986) The hemoglobinopathies. Edit. London.<br />
6. Maier-Redelsberger M., Girot R. (1989) Diagnostic biologique des maladies de l’hémoglobine. Feuillets de biologie, 170.<br />
7. Schneider R.G. (1978) Methods for detection of hemoglobin variants and hemoglobinopathies in the routine clinical laboratory. CRC Crit. Rev. Clin.<br />
Lab. Sci. 9, 243-271.<br />
8. Vovan L, Lara-Russo D., Orsini A. (1985) Diagnostic biologique des hémoglobinoses. Ann. Pédiat. 32, 9, 780-789.
VERWENDUNGSZWECK<br />
- 15 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Der <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Kit dient zur Abtrennung der normalen Hämoglobine (A und A 2 ) und zum Nachweis der<br />
Haupthämoglobinvarianten: S oder D und C oder E, durch Elektrophorese auf alkalischen Agarosegelen. Die erhaltenen Elektropherogramme werden<br />
visuell auf abnormale Muster untersucht. Die Densitometrie kann bei der Interpretation als Hilfe dienen, weil mit Ihr relative Konzentrationen<br />
individueller Banden gemessen werden können. Eine Elektrophorese auf sauren Gelen, z.B. mit der <strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong><br />
Prozedur, sollte zur Bestätigung der identifizierten Hämoglobinvarianten folgen, insbesondere um die Hämoglobine S von D und E von C zu<br />
unterscheiden.<br />
Jedes Agarosegel im <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Kit ist für sieben Proben bestimmt.<br />
Nur für den diagnostischen in vitro Gebrauch.<br />
TESTPRINZIP<br />
Hämoglobin ist ein komplexes Molekül und besteht aus zwei Paaren von Polypeptidketten. Jede Kette ist mit der Häm-Gruppe, einem Tetrapyrrolkern<br />
(Porphyrin,) der als Chelat ein Eisenatom bindet, verbunden. Der Häm-Teil ist in allen Hämoglobinen und ihren Varianten gleich. Der Typ des<br />
Hämoglobins wird durch den Proteinteil, der Globin genannt wird, bestimmt. Die Polypeptidketten α, ß, δ und γ bilden die normalen Hämoglobine:<br />
• Hämoglobin A = α 2 ß 2<br />
• Hämoglobin A2 = α 2 δ 2<br />
• fötales Hämoglobin F = α 2 γ 2<br />
Die α-Kette ist bei diesen drei Hämoglobinen gleich.<br />
Die räumliche Struktur des Hämoglobins und andere molekulare Eigenschaften (wie bei allen Proteinen) hängt von der Natur und Sequenz der<br />
Aminosäuren ab, die die Ketten bilden. Das Ersetzen von Aminosäuren durch Mutationen, ist für die Bildung der Hämoglobinvarianten verantwortlich.<br />
Diese haben unterschiedliche Oberflächenladungen und dadurch bei Elektrophoresen eine unterschiedliche Beweglichkeit, die ebenso vom pH-Wert<br />
und der Ionenstärke des Puffers abhängt.<br />
Die resultierenden qualitativen (oder strukturellen ) Abnormitäten werden Hämoglobinopathien genannt. Die verminderte Synthese von einer der<br />
Hämoglobinketten führt zu quantitativen (Regulations-) Abnormitäten, die Thalassämien genannt werden.<br />
Der Assay wird mit gewaschenen hämolysierten Roten Blutzellen (Erythrozyten) durchgeführt. Die Hämoglobine werden auf alkalischen Gelen<br />
elektrophoretisch getrennt und die Fraktionen durch Färbung mit Amidoschwarz sichtbar gemacht. Die getrockneten Gele können direkt interpretiert<br />
werden.<br />
REAGENZIEN UND MITGELIEFERTE MATERIALIEN IM <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> KIT<br />
| ARTIKEL | ART.-NR. 3010 |<br />
| Agarosegele (gebrauchsfertig) | 10 Gele |<br />
| Tris-Barbital Puffer (Stammlösung) | 3 Fläschchen, jedes 75 mL |<br />
| Verdünnungslösung (konzentriert) | 1 Fläschchen, 60 mL |<br />
| Amidoschwarz Färbelösung (Stammlösung) | 1 Fläschchen, 20 mL |<br />
| Entfärbelösung (Stammlösung) | 1 Fläschchen, 100 mL |<br />
| Hämolyse-Lösung (gebrauchsfertig) | 1 Fläschchen, 20 mL |<br />
| Applikatoren 7 Zähne (gebrauchsfertig) | 1 Pack von 10<br />
|<br />
|<br />
Filterpapier - Dünn | 1 Pack von 10 |<br />
FÜR OPTIMALE ERGEBNISSE<br />
Alle Reagenzien eines Kits müssen immer zusammen, gemäß den Instruktionen der Packungsbeilage benutzt werden.<br />
BITTE DIE PACKUNGSBEILAGE SORGFÄLTIG LESEN.<br />
1. AGAROSEGELE<br />
Vorbereitung<br />
Agarosegele sind gebrauchsfertig. Jedes Gel enthält: Agarose, 0,8 g/dl ; alkalischen Puffer pH 8,5 ± 0,1 ; Zusätze, ungefährlich bei den eingesetzten<br />
Konzentrationen, nötig für die optimale Durchführung.<br />
Gebrauch<br />
Hilfsmittel für die Elektrophorese der Hämoglobine.<br />
Lagerung, Stabilität und Anzeichen für Verfall<br />
Die Gele horizontal in der Originalverpackung bei Raumtemperatur (15 - 30 °C) oder gekühlt (2 - 8 °C) lagern. (Die Pfeile auf der Vorderseite des Kits<br />
müssen nach oben zeigen). Offensichtliche Temperaturschwankungen vermeiden. (z.B. nicht in der Nähe eines Fensters oder einer Hitzequelle<br />
lagern). Die Gele sind bis zum Ablauf des Verfallsdatums auf der Kitschachtel oder auf der Gelverpackung stabil.<br />
NICHT EINFRIEREN.<br />
Das Gel verwerfen, wenn:<br />
(i) sich Kristalle oder Präzipitate auf der Geloberfläche bilden oder die Geltextur sehr weich wird (dies alles resultiert vom Einfrieren des Gels) ;<br />
(ii) bakterielles - oder Pilzwachstum erscheint,<br />
(iii) sich eine abnormale Flüssigkeitsmenge in der Gelschachtel befindet (Absonderungen von Puffer aus dem Gel durch nicht korrekte<br />
Lagerbedingungen).<br />
SEBIA ARBEITSANLEITUNG - Deutsch
- 16 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
2. TRIS-BARBITAL-PUFFER<br />
Vorbereitung<br />
Der Inhalt jedes Fläschchens soll auf 1 Liter mit destilliertem Wasser oder deionisiertem Wasser verdünnt werden.<br />
Die Pufferlösung enthält nach der Verdünnung: Tris-Barbital pH 9,2 ± 0,3 ; Natriumazid.<br />
WARNUNG: Jedes Fläschchen mit Puffer-Stammlösung enthält 2,45 % Barbital, 13,73 % Natriumbarbital und 0,13 % Natriumazid. Nicht<br />
Verschlucken. Bei Verschlucken sofort ärztlichen Rat einholen! Beim Entsorgen Kontakt mit Säuren, Blei oder Kupfer vermeiden, da von<br />
diesen bekannt ist, dass sie explosive oder giftige Verbindungen mit Natriumazid bilden. Beim Entsorgen immer mit viel Wasser<br />
nachspülen.<br />
Gebrauch<br />
Elektrophoresepuffer.<br />
Lagerung, Stabilität und Anzeichen für Verfall<br />
Die Puffer-Stammlösung bei Raumtemperatur oder gekühlt lagern. Sie ist für mehrere Jahre, mindestens bis zum angegebenen Verfallsdatum auf der<br />
Kitschachtel und auf dem Etikett der Pufferfläschchen stabil. Verdünnte Pufferlösung ist bei Raumtemperatur in einer verschlossenen Flasche für<br />
1 Jahr stabil.<br />
Den Puffer verwerfen, wenn sich sein Aussehen verändert, z.B., wenn er durch mikrobielle Kontamination trübe wird.<br />
3. VERDÜNNUNGSLÖSUNG<br />
Vorbereitung<br />
Die Amidoschwarz-Verdünnungslösung ist wie im Abschnitt “Amidoschwarz-Färbelösung” beschrieben zu verwenden.<br />
Die Lösung enthält Zitronensäure.<br />
Gebrauch<br />
Zum Herstellen der Amidoschwarz-Färbelösung.<br />
Lagerung, Stabilität und Anzeichen für Verfall<br />
Konzentrierte Verdünnungslösung im Kühlschrank oder bei Raumtemperatur aufbewahren. Die Lösung ist bis zum Verfallsdatum (aufgedruckt auf dem<br />
Kit oder auf dem Flaschenetikett) haltbar. NICHT EINFRIEREN!<br />
Geben Sie kein Natriumazid zu.<br />
4. AMIDOSCHWARZ FÄRBELÖSUNG<br />
Vorbereitung<br />
Das Amidoschwarz Färbekonzentrat ist eine hochviskose Flüssigkeit deren Viskosität sich durch Lagerung verändern kann. Die Qualität des<br />
Färbekonzentrats wird durch höhere Viskosität nicht beeinträchtigt.<br />
Bitte beachten Sie die folgende Anleitung zum Herstellen der Färbelösung :<br />
1. 15 ml der Verdünnungslösung zu dem Amidoschwarz Färbekonzentrat geben.<br />
2. Die Färbekonzentrat Flasche fest verschließen.<br />
3. Die Flasche für etwa 5 Sekunden kräftig schütteln.<br />
4. Den Inhalt der Flasche in den Färbecontainer überführen.<br />
5. Schritt 1 – 4 zwei- bis dreimal wiederholen.<br />
6. Die restliche Verdünnungslösung in den Färbecontainer überführen und mit destilliertem oder deionisiertem Wasser auf 300 ml Gesamtvolumen<br />
auffüllen.<br />
7. Den Inhalt des Färbecontainers 5 – 10 Minuten mischen.<br />
Im Anschluss daran ist die Färbelösung gebrauchsfertig.<br />
Nach der Verdünnung enthält die Färbelösung: Zitronensäurelösung pH ≈ 2 ; 0,4 g/dl Amidoschwarz ; 6,7% Ethylenglycol ; zusätzliche Additive zur<br />
Optimierung (ungiftig in den verwendeten Konzentrationen).<br />
WARNUNG: Nicht verschlucken! Bei Verschlucken sofort ärztlichen Rat einholen!<br />
Gebrauch<br />
Zum Färben der Agarose Gele nach elektrophoretischer Trennung.<br />
WICHTIG: Die Färbelösung ist für maximal 10 Färbungen konzipiert. Wechseln Sie deshalb die Färbelösung nach 10 Färbungen aus.<br />
Lagerung, Stabilität und Anzeichen für Verfall<br />
Amidoschwarz- Konzentrat und verdünnte Färbelösung bei Raumtemperatur oder im Kühlschrank verschlossen aufbewahren um Flüssigkeitsverlust durch<br />
Verdunstung zu vermeiden. Das Amidoschwarz-Konzentrat ist bis zum Verfallsdatum (aufgedruckt auf dem Kit oder auf dem Flaschenetikett) haltbar.<br />
Verdünnte Färbelösung ist einen Monat haltbar.<br />
Die gebrauchsfertige Färbelösung nicht neben einer Wärmequelle aufbewahren.<br />
5. ENTFÄRBELÖSUNG<br />
Vorbereitung<br />
Jedes Fläschchen der Entfärbe-Stammlösung muss auf 100 Liter mit destilliertem oder deionisiertem Wasser verdünnt werden. Es ist vorteilhaft,<br />
jeweils nur 1 ml der Stammlösung auf 1,0 Liter zu verdünnen. Die verdünnte Entfärbelösung enthält Zitronensäure, 0,05 g/dl.<br />
Gebrauch<br />
Zum Entfärben, d.h. zum Entfernen von überschüssigem Färbemittel und von Hintergrundfärbung aus den Gelen.<br />
Lagerung, Stabilität und Anzeichen für Verfall<br />
Die Stammlösung der Entfärbelösung bei Raumtemperatur oder gekühlt lagern. Sie ist bis zum Verfallsdatum auf der Kitpackung oder auf dem Etikett<br />
des Entfärbelösungs-Fläschchen stabil. Die verdünnte Entfärbelösung ist bis zu einer Woche bei Raumtemperatur in einer verschlossenen Flasche<br />
stabil. Kein Natriumazid zufügen.<br />
Die verdünnte Entfärbelösung verwerfen, wenn sich ihr Aussehen verändert, z.B., wenn sie durch mikrobielle Kontamination trübe wird.<br />
Um mikrobielles Wachstum in der verdünnten Entfärbelösung bei Lagerung von mehr als einer Woche zu verhindern, sind 5 µl/dl ProClin 300 zu<br />
zufügen.<br />
Die mit ProClin versetzte, gebrauchsfertige Entfärbelösung ist in der verschlossenen Flasche bei Zimmertemperatur oder gekühlt bis zum<br />
Verfallsdatum stabil, das auf der Verpackung oder auf den Flaschenetiketten angegeben ist.
- 17 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
6. HÄMOLYSE-LÖSUNG<br />
Vorbereitung<br />
Die Hämolyse-Lösung ist gebrauchsfertig. Sie eine Pufferlösung mit Zusätzen, ungefährlich bei den eingesetzten Konzentrationen, nötig für die<br />
optimale Durchführung.<br />
Gebrauch<br />
Zur Hämolyse der Erythrozyten.<br />
Lagerung, Stabilität und Anzeichen für Verfall<br />
Die Hämolyse-Lösung bei Raumtemperatur oder gekühlt lagern. Sie ist bis zum Verfallsdatum auf der Kitpackung oder auf dem Etikett des Hämolyse-<br />
Lösungs-Fläschchens stabil.<br />
Die Hämolyse-Lösung verwerfen, wenn sich ihr Aussehen verändert, z.B., wenn sie durch mikrobielle Kontamination trübe wird.<br />
7. APPLIKATOREN<br />
Gebrauch<br />
Applikatoren für den einmaligen Gebrauch zum Probenauftrag.<br />
Lagerung<br />
Die Applikatoren an einem trockenen Platz bei Raumtemperatur oder gekühlt lagern.<br />
8. FILTERPAPIERE – DÜNN<br />
Gebrauch<br />
Für den einmaligen Gebrauch, um überschüssige Feuchtigkeit von der Geloberfläche vor der Probenaufgabe abzublotten.<br />
Lagerung<br />
Dünnes Filterpapier, vor Feuchtigkeit geschützt, bei Zimmertemperatur oder im Kühlschrank lagern.<br />
NICHT MITGELIEFERTE ABER BENÖTIGTE REAGENZIEN<br />
1. PHYSIOLOGISCHE KOCHSALZLÖSUNG<br />
Vorbereitung<br />
Stellen Sie eine 0,15 M (0,9 g/dl) NaCl-Lösung in destilliertem oder deionisiertem Wasser her.<br />
Gebrauch<br />
Zum Waschen der Erythrozyten.<br />
Lagerung, Stabilität und Anzeichen für Verfall<br />
Bei Raumtemperatur oder gekühlt lagern. Die Lösung nach drei Monaten verwerfen, wenn sich ihr Aussehen verändert, z.B., wenn sie durch<br />
mikrobielle Kontamination trübe wird. Für längere Lagerperioden, Natriumazid zugeben, 0,1 g/dl.<br />
2. FIXIERLÖSUNG (optional)<br />
Vorbereitung<br />
Mindestens 15 Minuten vor Gebrauch eine Lösung vorbereiten die folgende Volumenanteile enthält: 60 % Ethanol ; 10 % Essigsäure und<br />
30 % destilliertes oder deionisiertes Wasser. Gut mischen.<br />
Gebrauch<br />
Zur Fixierung elektrophoretisch getrennter Hämoglobine in Agarosegelen.<br />
Lagerung, Stabilität und Anzeichen für Verfall<br />
Die Fixierlösung dicht verschlossen, um Verdampfungen zu verhindern, bei Raumtemperatur lagern. Nach 3 Monaten verwerfen. Nicht mehr als 4 Gele<br />
in jeweils 150 ml fixieren.<br />
NICHT MITGELIEFERTE ABER BENÖTIGTE AUSRÜSTUNG UND ZUBEHÖR<br />
1. Netzgerät: GD 61 D SEBIA, Art.-Nr. 1300 ; GD 251 D SEBIA, Art.-Nr. 1301 ; MG 300 SEBIA, Art.-Nr. 1302 oder MG 500 SEBIA, Art.-Nr. 1303.<br />
2. <strong>HYDRAGEL</strong> <strong>K20</strong> APPLIKATOR SEBIA, Art.-Nr. 1409, enthält den <strong>HYDRAGEL</strong> <strong>K20</strong> Applikatorträger.<br />
3. Feuchte Kammer, Art.-Nr. 1270.<br />
4. Elektrophorese-Kammer: <strong>K20</strong> SEBIA, Art.-Nr. 1400.<br />
5. Behälter und Gelhalter zum Abarbeiten der Gele: <strong>HYDRAGEL</strong> <strong>K20</strong> Zubehörkit SEBIA, Art.-Nr. 1420.<br />
6. Pipetten: 5 µl, 10 µl und 200 µl.<br />
7. Inkubator-Trockner: IS 80 SEBIA, Art.-Nr. 1430.<br />
8. Densitometer / Flachbett-Scanner um Gele von 82 x 51 mm bei 570 nm (Gelbfilter) einzulesen: HYRYS SEBIA, DVSE SEBIA oder PHORESIS<br />
Software für Flachbett-Scanner. Zur Durchführung und für die Kalibrierung, siehe die Bedienungsanleitung des Herstellers.<br />
ANALYSENPROBEN<br />
Probensammlung und Lagerung<br />
Frische Blutproben mit Antikoagulantien werden für die Analyse empfohlen. Die üblichen Antikoagulantien solche die EDTA, Citrat oder Heparin<br />
enthalten sind akzeptabel. Keine Antikoagulantien mit Jodacetat verwenden. Die Blutproben sollten gemäß den etablierten Regeln zur<br />
Probenentnahme für klinische Proben gewonnen werden. Bei Bedarf können die Proben für bis zu 5 Tagen bei 2 – 8 °C gelagert werden.<br />
Probenvorbereitung<br />
• Das Probenröhrchen vor der Entnahme der Blutprobe mischen.<br />
• Blut mit Antikoagulanz bei 5 000 Upm für 5 Minuten zentrifugieren.<br />
• Das Plasma verwerfen.
- 18 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
• Erythrozyten zweimal mit 10fachen Volumen physiologischer Kochsalzlösung waschen ; mit großer Sorgfalt vorgehen, wenn das zu verarbeitende<br />
Volumen der Erythrozyten kleiner als 10 µl ist.<br />
• Die überschüssige Salzlösung von den roten Blutkörperchen entfernen. Die Blutzellen mischen und 10 µl für die Hämolyse abnehmen.<br />
• Hämolysieren Sie 10 µl gepackte Erythrozyten mit 130 µl Hämolyse-Lösung.<br />
• Für 10 Sekunden mischen und für 5 Minuten bei Raumtemperatur inkubieren.<br />
HINWEISE:<br />
- Um Hämolysate von Proben mit milder Anämie (ungefähr 10 g/dl Hb) oder mit starker Anämie (< 7 g/dL Hb) herzustellen, kann das Volumen von<br />
gepackten Eryzhrozyten auf 15 µl bzw. 20 µl erhöht werden. Die Intensität der Färbung wird dadurch erhöht, aber die relativen Konzentration<br />
individueller Banden werden nicht verändert.<br />
- Das Hämolysat muss nicht gefiltert oder zentrifugiert werden.<br />
- Die SEBIA Hämolyselösung beeinträchtigt das instabile Bart’s Hämoglobin nicht.<br />
PROZEDUR<br />
I. MIGRATIONSSCHRITT<br />
1. Den <strong>HYDRAGEL</strong> <strong>K20</strong> Applikatorträger auf eine flache Oberfläche legen (Abb. 1) und den Applikatorträger hochklappen.<br />
2. 120 µl destilliertes Wasser oder deionisiertes Wasser auf das untere Drittel des Rahmens geben, der auf dem <strong>HYDRAGEL</strong> <strong>K20</strong><br />
Applikatorträger aufgedruckt ist.<br />
3. Das <strong>HYDRAGEL</strong> Agarosegel auspacken.<br />
4. Ein dünnes Filterpapier vorsichtig und gleichmäßig auf die Oberfläche legen um überschüssige Feuchtigkeit zu entfernen. Das Filterpapier<br />
sofort wieder entfernen.<br />
WARNUNG: Das Filterpapier nicht zu lange mit dem Gel in Kontakt lassen, um ein Austrocknen des Gels zu vermeiden.<br />
5. Das Gel (Gelseite nach oben) mit seinem Rand gegen den Halter am Boden des aufgedruckten Rahmens (Abb. 2) legen.<br />
6. Das Gel biegen und in den Wasservorrat hineindrücken (Abb. 2). Sicherstellen, dass keine Luftblasen eingeschlossen werden, dass sich<br />
Wasser unter dem gesamten Gel befindet, und dass das Gel sich in einer Linie mit dem aufgedruckten Rahmen befindet.<br />
7. Den Applikatorträger (mit hochgestelltem Hebel) bis zur mittleren Position herabsenken.<br />
8. Einen Applikator so auf eine flache Oberfläche legen, dass die Nummern (Vertiefungen) nach oben zeigen (Abb. 3).<br />
9. In die Vertiefungen des Applikators je 10 µl der hämolysierten Probe auftragen. Den Applikator innerhalb von 2 Minuten beladen. Den<br />
Applikator ohne Verzögerungen einsetzen. Bei späterem Gebrauch (bis zu 8 Stunden) muss der Applikator in der Feuchten Kammer mit<br />
Zähnen nach oben aufbewahrt werden (die Applikatoren am Zahnschutzrahmen anfassen). Die gesamte Kammer gekühlt lagern und das Gel<br />
erst unmittelbar vor Gebrauch auf den <strong>HYDRAGEL</strong> <strong>K20</strong> Applikatorträger legen.<br />
Für weitere Details siehe: Bedienungsanleitung „Feuchte-Kammer“.<br />
10. Den Schutzrahmen für die Applikatorzähne abnehmen.<br />
11. Den Applikator mit den Proben in die Position 4 auf dem Applikatorträger einlegen.<br />
WICHTIG: Die aufgedruckten Nummern auf den Applikatoren müssen zum Bediener zeigen. (Abb. 4).<br />
12. Den Applikatorträger durch Drehen des Hebels absenken, sodass der Applikator die Geloberfläche berührt. Den Träger nicht vollständig<br />
herunterdrücken.<br />
13. Nach einer Minute die Applikatoren durch Drehen des Hebels hochfahren und verwerfen.<br />
14. Das Gel in eine passende Elektrophoresekammer mit den Proben zur kathodischen Seite überführen. Beim Verwenden der SEBIA <strong>K20</strong><br />
Kammer, das <strong>HYDRAGEL</strong> auf die Brücke mit der Gelseite nach unten platzieren. Das Gel sollte an jeder Seite ungefähr 1 cm in den Puffer<br />
eintauchen.<br />
Für weitere Details siehe Bedienungsanleitung der Kammer <strong>K20</strong>.<br />
15. Die Kammer mit dem Netzgerät verbinden.<br />
| MIGRATIONS-BEDINGUNGEN | SEBIA <strong>K20</strong> |<br />
| Puffervolumen pro Kammer | 150 ml |<br />
| Gesamtpuffervolumen | 300 ml |<br />
| Migrationszeit | 15 Minuten |<br />
| Konstante Spannung | 165 V<br />
|<br />
|<br />
Einschaltstrom (ein Gel) | 7 ± 2 mA |<br />
16. Nach der Migration, den Stromfluss in der Kammer unterbrechen und das Gel entfernen.<br />
II. FIXATION<br />
Die Gele nach einer der nachfolgenden Prozeduren weiterbehandeln.<br />
Heißluftfixierung (Nur mit dem SEBIA IS 80 Inkubator-Trockner empfohlen):<br />
Das Gel vollständig im Inkubator-Trockner bei 80 °C (für 10 Minuten) trocknen.<br />
Fixierung mit Fixierlösung:<br />
1. Das Gel im Gelhalter platzieren (enthalten im SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong> Zubehör Kit).<br />
2. Den Behälter mit (enthalten im SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong> Zubehör Kit) 150 ml Fixierlösung füllen.<br />
3. Das Gel für 15 Minuten in der Fixierlösung eintauchen.<br />
4. Das Gel herausnehmen und mit Heißluft bei 80 ° C im Inkubator-Trockner trocknen.<br />
WICHTIG: Das Gel muss vollständig trocken sein.<br />
III. FÄRBEN UND ENTFÄRBEN<br />
1. Das getrocknete und abgekühlte Gel für 5 Minuten in die Färbelösung eintauchen.<br />
2. In drei aufeinanderfolgenden Bädern mit Entfärbelösung das Gel entfärben bis der Hintergrund vollständig farblos und klar ist.<br />
3. Überschüssige Flüssigkeit von der Geloberfläche mit einem saugfähigem Papier absaugen und das Gel bei 80 °C mit Heißluft trocknen. Bei<br />
Bedarf die Rückseite (plastikverstärkte Seite) des Gels mit einem feuchten Tuch reinigen.
- 19 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
IV. EINLESEN<br />
Das Gel mit einem Densitometer bei 570 nm oder mit einem Gelbfilter einlesen. Bei Verwendung von HYRYS oder DVSE Densitometern, die<br />
A 2 -Fraktion bei der 5 mm Markierung auf dem Scanfenster positionieren: die Nullstellung des Hintergrunds wird zwischen der A 2 - und der Carbo-<br />
Anhydrase-Fraktion beim niedrigsten Punkt durchgeführt.<br />
HINWEIS : Zur Erzielung bester Ergebnisse folgendes beachten:<br />
- Die Einleselänge einstellen um vollständige Elektrophoresemuster einzuschließen (≈ 30 mm).<br />
- Sicherstellen dass die Minima auf beiden Seiten der A 2 -Fraktion ganz am Fuß des A 2 –Peak positioniert sind.<br />
Es wird empfohlen das gefärbte Gel ohne Verzögerung einzulesen. Als Referenz für die Zukunft können sie in einer Schutzhülle an einem trocken<br />
dunklen Platz fern von Hitzequellen gelagert werden und innerhalb von mindestens 3 Monaten visuell interpretiert werden.<br />
ERGEBNISSE<br />
Qualitätskontrolle<br />
Es wird empfohlen bei jedem Lauf ein Kontrollblut oder ein bekanntes Blut, das die Hämoglobine A, F, C und S enthält, zur Kontrolle mitlaufenzulassen.<br />
Werte<br />
Durch das Einlesen von gefärbten Elektropherogrammen mit dem Densitometer werden relative Konzentrationen (Prozente) individueller<br />
Hämoglobinbanden erhalten.<br />
Normalwerte (Mittelwert ± 2 SD) wurden mit der <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Prozedur von einer gesunden Population von 200 Erwachsenen<br />
(Männer und Frauen) bestimmt:<br />
Hämoglobin A ≥ 96,5 %<br />
Hämoglobin F < 2,0 % (*)<br />
Hämoglobin A2 ≤ 3,5 %<br />
(*) siehe Interferenz und Limitationen<br />
Jedem Labor wird empfohlen eigene Normalwerte festzulegen.<br />
Interpretation<br />
1. Qualitative Abnormitäten: Hämoglobinopathien<br />
Die meisten Hämoglobinopathien werden durch Mutationen verursacht, die zu einzelnen Aminosäureaustauschen in einem Typ der vier<br />
Polypeptidketten führen. Die klinische Signifikanz eines solchen Austauschen hängt vom Typ der Aminosäure und von der betroffenen Stelle ab. Bei<br />
klinisch signifikanten Erkrankungen ist entweder die α-Kette oder die ß-Kette (sogar die γ-Ketten) betroffen.<br />
Mehr als 200 Varianten des adulten Hämoglobins sind bislang beschrieben worden. Die ersten untersuchten abnormalen Hämoglobine und die am<br />
häufigsten vorkommenden haben eine veränderte elektrische Nettoladung, wodurch sie mit Elektrophorese einfach nachweisbar sind.<br />
Es gibt vier abnormale Haupt-Hämoglobine, welche von besonderem klinischen Interesse sind: S, C, E und D.<br />
Die <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Kits werden für eine vorläufige Identifikation von Hämoglobinopathien und Thalassämien. Sobald ein<br />
abnormales Muster festgestellt wird, sollte seine Identität mit entsprechenden ausschließenden Tests bestätigt werden (z. B. mit Gelelektrophoresen<br />
auf sauren Agarose Gelen).<br />
Hämoglobin S<br />
Das Hämoglobin S kommt am häufigsten vor. Es entsteht durch den Austausch eines Glutaminsäurerestes (saure Aminosäure) der Beta-Kette durch<br />
Valin (eine neutrale Aminosäure). Seine elektrophoretische Mobilität wird dadurch verlangsamt. Auf alkalisch gepufferten Gelen wie <strong>HYDRAGEL</strong><br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> wandert das Hämoglobin S zwischen den Fraktionen A und A 2 .<br />
Hämoglobin C<br />
Ein Glutaminsäurerest der Beta-Kette wurde durch einen Lysinrest ersetzt (basische Aminosäure): seine Mobilität ist stark verringert. Bei der<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Prozedur überlagern sich die Fraktionen C, E, und A 2 . Wenn diese Fraktion > 15 % beträgt, müssen die<br />
Hämoglobine C und E vermutet werden.<br />
Hämoglobin E<br />
Ein Glutaminsäurerest der Beta-Kette wird durch Lysin ersetzt. Bei der <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Prozedur wandert das Hämoglobin E<br />
genau wie das Hämoglobin C. Aber im Unterschied zu Hämoglobin C, trennt es sich nicht vom Hämoglobin A in sauren Puffer [<strong>HYDRAGEL</strong> ACID(E)<br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>]. Diese Eigenschaft erlaubt die Unterscheidung zwischen E und C.<br />
Hämoglobin D<br />
Ein Glutaminsäurerest der Beta-Kette wird durch einen Glutaminrest ersetzt. Bei der <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Prozedur wandert dieses<br />
Hämoglobin ganz genau wie das Hämoglobin S. Das Hämoglobin D trennt sich in sauren Puffer nicht vom Hämoglobin A [<strong>HYDRAGEL</strong> ACID(E)<br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>]. Diese Eigenschaft erlaubt die Unterscheidung zwischen S und D.<br />
2. Quantitative Abnormitäten: Thalassämien<br />
Thalassämien stellen eine sehr heterogene Gruppe von genetischen Störungen dar, die durch eine verminderte Synthese eines oder mehrerer Typen<br />
von Polypeptidketten gekennzeichnet sind. Der molekulare Mechanismus dieser Verminderung ist bis jetzt nicht vollständig beschrieben.<br />
Es gibt zwei Arten von Thalassämiesyndromen:<br />
Alpha-Thalassämien<br />
Sie werden durch eine verminderte Synthese der α-Ketten charakterisiert, was konsequenterweise die Synthese aller normalen Hämoglobine betrifft.<br />
Die überschüssige Synthese von ß-Ketten und γ-Ketten im Verhältnis zu α-Ketten induziert die Bildung von Tetrameren ohne jede α-Kette:<br />
• Hämoglobin Bart = γ 4,<br />
• Hämoglobin H = ß 4.
Beta-Thalassämien<br />
Sie werden durch eine verminderte Synthese der Beta-Kette gekennzeichnet. Nur das Hämoglobin A ist betroffen.<br />
Dafür sind die Prozentanteile von Hämoglobin F und A 2 im Vergleich zu Hämoglobin A erhöht.<br />
3. Migrationsmuster<br />
Migration bei normalen<br />
Hämoglobinen<br />
A(A0 + A1 ) A (A0 + A1 )<br />
F<br />
S - D<br />
A2 A2 - C - E<br />
Anhydrase Anhydrase<br />
Auftragungspunkt<br />
A 0 : Die nicht-glykolisierte Fraktion des normalen adulten Hämoglobin A.<br />
A 1 : Die glykolisierte Fraktion des normalen adulten Hämoglobin A.<br />
Im obigen Muster befindet sich unten die Anode und oben die Kathode.<br />
- 20 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Interferenzen und Limitationen<br />
• Keine hämolysierten Blutproben verwenden.<br />
• Wenn ein abnormales Hämoglobin nachgewiesen wird, welches ein anderes Verhalten als die Haupthämoglobinvarianten S, C, D und E zeigt,<br />
sollten andere Eigenschaften für die Identifizierung herangezogen werden, (wie z.B.: Isoelektrische Fokussierung, Globinketten-Elektrophorese)<br />
oder ein spezialisiertes Labor konsultiert oder die Probe in ein spezialisiertes Labor gesendet werden.<br />
• Der densitometrische Assay von Hb F (oder irgend einem anderen geringem Hämoglobin, das in der Nähe der Hauphämoglobinfraktionen wandert)<br />
ist nur semiquantitative, da die Analyse bei Werten unterhalb von 2 % - 3 % vom Gesamthämoglobin ungenau wird.<br />
• Einige homozygote „S“ Patienten erhalten eine Behandlung mit Hydrea® (Hydroxyharnstoff), die zur Induktion der Synthese von fetalem<br />
Hämoglobin führen kann. In einigen Fällen wurde beobachtet, dass die Mobilität des induzierten Hämoglobin F auf <strong>HYDRAGEL</strong> 7 <strong>HEMOGLOBIN</strong>(E)<br />
im Vergleich zu physiologischem Hämoglobin F leicht unterschiedlich ist.<br />
• Bei längerer Lagerung der Proben (über 7 Tage), kann sich der Hintergrund hinter der Hb A Fraktion als distinkte Fraktion darstellen. Interpretieren<br />
sie diese Fraktion nicht als Hämoglobin-Variante, z.B. als Hämoglobin H oder Bart.<br />
Fehlersuche<br />
Bitte rufen Sie den Technischen Service von SEBIA an, wenn der Test nicht richtig funktioniert, obwohl die Anweisungen zur Vorbereitung, Lagerung<br />
und zur Durchführung sorgfältig beachtet wurden.<br />
Datensicherheitsblätter sowie Informationen zur Abfallentsorgung sind bei SEBIA GmbH, Fulda zu erfragen.<br />
CHARAKTERISTISCHE DATEN<br />
Migration der wichtigsten<br />
anomalen Hämoglobine<br />
Alle charateristischen Daten basieren auf einer Studie, die durch vergleichende Untersuchungen von SEBIA <strong>HYDRAGEL</strong> Materialien und Geräte mit<br />
einem anderen kommerziell erhältlichen Gelelektrophoresesystem erhalten wurden. Zusätzlich wurden Konkordanz-Untersuchungen durchgeführt,<br />
wenn die Identifizierung der Hämoglobine und die Werte durch andere anerkannte Methoden ermittelt wurden. Die Ergebnisse von repräsentativen<br />
Beispielen werden hier aufgeführt.<br />
Alle Elektropherogramme wurden visuell interpretiert. Für alle densitometrischen Messungen wurde das HYRYS Densitometer von SEBIA verwendet,<br />
um die visuellen Daten angemessen zu vervollständigen.<br />
Reproduzierbarkeit innerhalb eines Laufs<br />
Drei Blutproben wurden mit der <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Prozedur mit Gelen einer Charge untersucht. Jede Probe wurde auf sämtlichen<br />
Laufspuren eines Gels aufgetragen. Die folgende Tabelle zeigt die Mittelwerte, Standardabweichung und den Variationskoeffizient für jede individuelle<br />
Hämoglobinkomponente in den drei Proben, die mittels der densitometrischen Prozentwerte für jede einzelne Laufspur errechnet wurden. Weiterhin<br />
zeigten die Wiederholungen keine falsch positiven oder falsch negativen Werte.<br />
| KOMPONENTE | MITTELWERT | SD | CV (%) |<br />
| Normales Blut |<br />
| Hb A | 97,4 | 0,1 | 0,1 |<br />
| Hb A | 2 2,6 | 0,1 | 5,3 |<br />
| Erhöhtes Hb A2 |<br />
| Hb A | 95,2 | 0,2 | 0,2 |<br />
| Hb A | 2 4,8 | 0,2 | 4,4 |<br />
| Erhöhtes Hb C |<br />
| Hb A | 56,7 | 0,4 | 0,8<br />
|<br />
|<br />
Hb C | 43,3 | 0,4 | 1,0 |<br />
Reproduzierbarkeit innerhalb verschiedener Läufe<br />
Blutproben wurden mit der <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Prozedur mit Gelen einer Charge elektrophoretisch getrennt. Unter den analysierten<br />
Proben befanden sich sieben Proben mit einem abnormalen Hämoglobin (Hb S, Hb F oder Hb C), zwei Proben mit erhöhtem Hb A 2 , die restlichen<br />
Proben waren normale Blutproben. Die Mittelwerte, Standardabweichung und die Variationskoeffizienten wurden aus den Daten für jede individuelle<br />
Hämoglobinkomponente aus jeder Probe berechnet. Der Wertebereich um die Mittelwerte, Standardabweichungen und um die Variationskoeffizienten<br />
und die Mittelwerte aus den Variationskoeffizienten, die die Gesamtheit der individuellen Komponenten repräsentieren sind unten in der Tabelle<br />
aufgeführt. Im übrigen zeigten die Wiederholungen keine falsch positiven oder falsch negativen Werte.
- 21 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
| KOMPONENTE | MITTELWERTE | SD | VK (%) | MITTLERER |<br />
| | | | | VK (%) |<br />
| Hb A | 18,0 – 97,8 | 0,1 – 1,0 | 0,1 – 4,0 | 0,8 |<br />
| Hb F | 13,3 – 76,3 | 0,5 – 0,6 | 0,7 – 3,4 | 1,8 |<br />
| Hb C | 21.5 – 43,5 | 0,2 – 0,3 | 0,6 – 1,1 | 0,8 |<br />
| Hb S/D | 9,7 – 84,1 | 0,1 – 0,6 | 0,4 – 2,6 | 1,1<br />
| |<br />
Hb A | 2 2.2 – 5,7 | 0,1 – 0,2 | 2,3 – 7,6 | 4,0 |<br />
Genauigkeit Nachweis von Hämoglobin-Abnormitäten<br />
63 unterschiedliche Blutproben wurden mit der <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Prozedur und einem anderen kommerziell erhältlichem<br />
Agarosegelsystem untersucht. Die Blutproben und ihre diagnostische Bewertung wurden von einem Krankenhaus zur Verfügung gestellt. Die<br />
Diagnose basierte auf Gelelektrophoresen auf alkalischen und sauren Gelen und/oder auf HPLC-Analysen. Alle abnormalen Hämoglobine oder<br />
abnormale Spiegel normaler Hämoglobine, die mit der <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Prozedur nachgewiesen wurden, waren in<br />
Übereinstimmung mit dem vergleichbaren System, den Krankenhaus Resultaten und der klinischen Diagnose. Es gab keinen Fall von falsch positivem<br />
Resultat, wie z.B. den Nachweis von abnormalen Banden oder abnormale Spiegel einer normalen Bande, bei denen keine Abnormalität existierte.<br />
Genauigkeit - Quantitative Bestimmung von Hb A 2<br />
Die Spiegel von 51 Blutproben mit normalen und erhöhten Spiegeln von Hb A 2 wurden beide durch Densitometrie der Gele, die mit der <strong>HYDRAGEL</strong><br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> Prozedur abgearbeitet wurden, gemessen. Die gemessenen Werte von beiden Verfahren wurden durch Berechnung der<br />
linearen Regression miteinander verglichen. Die Ergebnisse der linearen Regression werden unten in der Tabelle aufgeführt: (y = <strong>HYDRAGEL</strong>)<br />
| Korrelationskoeffizient | y-Achsenabschnitt | Steigung | Wertebereich der % Werte |<br />
| | | | (System von SEBIA) |<br />
| 0,973 | -0,344 | 0,963 | 1,5 – 5,7 |<br />
LITERATUR<br />
1. Fairbanks V.F., ed. (1980) Hemoglobinopathies and thalassemia: Laboratory methods and case studies. Brian C. Decker, New York.<br />
2. Galacteros F. (1986) Thalassémie, drépanocytose et autres hémoglobinopathies. Techniques et Biologie, 3, 174-178.<br />
3. Huisman T.H.J. and. Jonxis J.H.P (1977) The hemoglobinopathies: techniques of identification. Marcel Dekker, New York.<br />
4. Krauss J.S., Drew P.A., Jonah M.H., Trinh M., Shell S., Black L. and Baisden C.R. (1986) Densitometry and microchromatography compared for<br />
determination of the hemoglobin C and A 2 proportions in hemoglobin C and hemoglobin SC disease and in hemoglobin C trait. Clin. Chem. 32, 5,<br />
860-863.<br />
5. Livingstone C. (1986) The hemoglobinopathies. Edit. London.<br />
6. Maier-Redelsberger M., Girot R. (1989) Diagnostic biologique des maladies de l’hémoglobine. Feuillets de biologie, 170.<br />
7. Schneider R.G. (1978) Methods for detection of hemoglobin variants and hemoglobinopathies in the routine clinical laboratory. CRC Crit. Rev. Clin.<br />
Lab. Sci. 9, 243-271.<br />
8. Vovan L., Lara-Russo D., Orsini A. (1985) Diagnostic biologique des hémoglobinoses. Ann. Pédiat. 32, 9, 780-789.
GEBRUIKSINDICATIE<br />
- 22 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> kit is ontwikkeld voor de scheiding van normale hemoglobine (A en A 2 ) en voor de detectie van de belangrijke<br />
hemoglobine varianten: S of D en C of E, door middel van elektroforese op alkalisch gebufferde agarose gels. De resulterende elektroforegrammen<br />
worden visueel geëvalueerd op afwijkende patronen. Densitometrie kan als hulpmiddel dienen bij de interpretatie door het leveren van relatieve<br />
concentraties van de afzonderlijke fracties.<br />
Elektroforese op een zure gel, bijvoorbeeld in de <strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure is essentieel voor de bevestiging van de<br />
identificatie van de hemoglobine varianten, met name om de hemoglobinen S van D en E van C te onderscheiden.<br />
Iedere agarosegel in de <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> kit is bedoeld voor de analyse van 7 monsters.<br />
Voor gebruik bij in vitro diagnostiek.<br />
PRINCIPE VAN DE TEST<br />
Hemoglobine is een complex molecuul dat is samengesteld uit twee paar polypeptideketens. Elke keten is verbonden aan het haem, een<br />
tetrapyrollische kern (porfyrine) dat een ijzeratoom cheleert. Het haem deel komt bij alle hemoglobinen en hun varianten voor. Het type hemoglobine<br />
wordt vastgesteld op basis van het proteïnedeel dat globine genoemd wordt. Het normale menselijke hemoglobine wordt samengesteld uit de<br />
polypeptideketens α, ß, δ en γ:<br />
• hemoglobine A ................................... = α 2 ß 2<br />
• hemoglobine A 2 .................................. = α 2 δ 2<br />
• foetale hemoglobine F........................ = α 2 γ 2<br />
Deze drie hemoglobinen hebben de α-keten gemeenschappelijk.<br />
De open structuur van hemoglobine (zoals bij alle proteïnen) hangt samen met de soort en de volgorde van de aminozuren die de ketens vormen. De<br />
verbindingen tussen de verschillende aminozuren zijn verantwoordelijk voor de vorm van het molecuul, zijn stabiliteit en eigenschappen. Substitutie<br />
van aminozuren door mutatie is verantwoordelijk voor de formering van hemoglobinevarianten met een andere oppervlaktelading en dus een andere<br />
elektroforetische mobiliteit, hetgeen ook afhankelijk is van de pH en de ionische sterkte van de buffer. Bij een zure pH-waarde wordt de mobiliteit<br />
eveneens beïnvloed door elektrostatische interactie tussen de positief geladen hemoglobinemoleculen en de negatief geladen moieteiten in de agar.<br />
De resulterende kwalitatieve (of structurele) abnormaliteiten worden hemoglobinopathiën genoemd. De verminderde synthese van een van de<br />
hemoglobineketens voert tot kwantitatieve (of regulering) abnormaliteiten hetgeen thalassemie genoemd wordt.<br />
De toetsing wordt uitgevoerd op het hemolysaat van gewassen rode bloedlichaampjes. De hemoglobinen worden elektroforetisch gescheiden op zure<br />
gels en de fracties worden gevisualiseerd door kleuring met amidozwart. De gedroogde gels zijn gereed voor interpretatie.<br />
DE <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> KIT BEVAT DE VOLGENDE REAGENTIA EN ANDERE MATERIALEN<br />
| BESTANDDELEN | PRODUKTNR. 3010 |<br />
| Agarose-gels (klaar voor gebruik) | 10 gels |<br />
| Tris-Barbitalbuffer (concentraat) | 3 flesjes van 75 ml |<br />
| Verdunner voor de kleuroplossing (concentraat) | 1 flesje van 60 ml |<br />
| Amidozwart kleurstof (concentraat) | 1 flesje van 20 ml |<br />
| Ontkleuringoplossing (concentraat) | 1 flesje van 100 ml |<br />
| Hemolyserende oplossing (gebruiksklaar) | 1 flesje, 20 ml |<br />
| Applicatoren met 7 tanden (gebruiksklaar) | 1 pakje van 10 stuks<br />
|<br />
|<br />
Filterpapier - dun | 1 pakje van 10 stuks |<br />
VOOR OPTIMALE RESULTATEN<br />
Onderdelen uit dezelfde kit dienen altijd samen te worden gebruikt en in overeenstemming met de instructies op de bijsluiter.<br />
LEES DE GEBRUIKSAANWIJZING ALTIJD ZORGVULDIG DOOR.<br />
1. AGAROSE-GELS<br />
Voorbereiding<br />
De agarosegels zijn klaar voor gebruik. Iedere gel bevat: agarose, 8 g/l ; alkalische buffer, pH 8,5 ± 0,1 ; in de gebruikte concentraties niet schadelijke<br />
toevoegingen die noodzakelijk zijn voor een optimale werking.<br />
Gebruik<br />
Hulpmedium voor hemoglobinen-elektroforese.<br />
Opslag, stabiliteit en tekenen van verval<br />
De gels moeten horizontaal worden opgeslagen in de originele beschermende verpakking en bij kamertemperatuur (15 ° tot 30 °C) bewaard worden<br />
of gekoeld (2 ° tot 8 °C) (De pijl op de voorzijde van de verpakking moet naar boven wijzen.). Aanzienlijke temperatuurschommelingen moeten<br />
vermeden worden tijdens de periode van opslag (dus bijvoorbeeld niet bewaren in de buurt van een raam of een warmtebron). De gels zijn stabiel tot<br />
de houdbaarheidsdatum die op de verpakking, of op het verpakkingslabel van de gel, staat aangegeven. NIET BEVRIEZEN.<br />
Verwijder de gel wanneer er:<br />
(i) zich kristallen of neerslag op het oppervlak van de gel vormen, of wanneer de textuur van de oppervlakte van de gel erg zacht wordt (dit geeft aan<br />
dat de gel bevroren is geweest) ;<br />
(ii) bacteriële of schimmelgroei wordt waargenomen ;<br />
(iii) een abnormale hoeveelheid vloeistof in de gelbox aanwezig is (wijst er op dat afscheiding van buffer uit de gel heeft plaatsgevonden tijdens<br />
onjuiste opslagomstandigheden).<br />
SEBIA INSTRUCTIEBLAD - Nederlands
- 23 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
2. TRIS-BARBITAL BUFFER<br />
Voorbereiding<br />
Elk flesje van het bufferconcentraat wordt verdund tot 1 liter met gedestilleerd of gedeïoniseerd water. Na verdunning bevat de bufferoplossing :<br />
Tris-barbital pH 9,2 ± 0,3 ; natriumazide, 0,10 g/l ; en in de gebruikte concentraties niet schadelijke toevoegingen die noodzakelijk zijn voor een<br />
optimale werking.<br />
WAARSCHUWING: Elk flesje buffer bevat 2,45 % barbital, 13,73 % natriumbarbital en 0,13 % natriumazide. Niet voor inwendig gebruik! Bij<br />
abusievelijke inname dient onmiddellijk een arts gewaarschuwd te worden! Natriumazide kan explosieve of toxische verbindingen aangaan<br />
met zuren, lood of koper. Bij verwijdering altijd spoelen met een grote hoeveelheid water.<br />
Gebruik<br />
Elektroforese buffer.<br />
Opslag, stabiliteit en tekenen van verval<br />
Het bufferconcentraat bij kamertemperatuur of gekoeld opslaan. Het blijft gedurende enige jaren stabiel, tenminste tot de houdbaarheidsdatum zoals<br />
aangegeven op de verpakking of de labels op de flesjes met buffer. De verdunde bufferoplossing is gedurende een jaar stabiel in een gesloten fles.<br />
Verwijder de verdunde buffer zodra er uiterlijke veranderingen optreden, bijvoorbeeld wanneer deze troebel wordt als gevolg van besmetting met<br />
microben.<br />
3. VERDUNNER VOOR DE KLEUROPLOSSING<br />
Bereiding<br />
De voorraad verdunner voor de kleuroplossing moet toegepast worden volgens de beschrijving in de paragraaf "AMIDOZWART KLEUROPLOSSING".<br />
Het bevat een zure oplossing.<br />
Toepassing<br />
Bij de preparatie van de amidozwart kleuroplossing.<br />
Opslag, stabiliteit en tekenen van verval<br />
De voorraad verdunner voor de kleuroplossing wordt bewaard bij kamertemperatuur of gekoeld. De verdunner is stabiel tot de houdbaarheidsdatum<br />
zoals deze is aangegeven op de verpakking van de kit of op de labels van de flesjes met verdunner voor de kleuroplossing. DIT PRODUCT NIET<br />
INVRIEZEN!<br />
Geen natriumazide toevoegen.<br />
4. AMIDOZWART KLEUROPLOSSING<br />
Bereiding<br />
De geconcentreerde amidozwart kleuringoplossing is een viskeuze oplossing die kan geleren. De integriteit van de basisoplossing wordt niet beïnvloed<br />
door de toename van de viscositeit of de hardwording.<br />
In alle gevallen adviseren wij u de hieronder beschreven procedure te volgen om de perfecte kleuring te behouden:<br />
1. Voeg 15 ml verdunningsmiddel aan het flesje met geconcerteerd amidozwart toe.<br />
2. Sluit het flesje zorgvuldig.<br />
3. Schut het flesje nu stevig gedurende ongeveer 5 seconden.<br />
4. Giet de oplossing in de houder van waaruit de kleuroplossing verwerkt wordt.<br />
5. Herhaal deze stap tweemaal, zo nodig driemaal.<br />
6. Giet de resterende verdunner in de houder en vul het volume aan tot 300 ml met gedestilleerd of gedeioniseerd water.<br />
7. Meng de inhoud van de cubitainer stevig gedurende 5 tot 10 minuten.<br />
De kleuringoplossing is nu gereed voor gebruik.<br />
Na verdunning bevat de werkzame verdunde kleuroplossing: zuuroplossing pH ≈ 2 ; amidozwart, 0.4 g/dl ; ethyleenglycol, 6.7 % ; additieven,<br />
ongevaarlijk bij te toegepaste concentraties die nodig zijn voor optimale werking.<br />
WAARSCHUWING: Schadelijk bij inname.<br />
Toepassing<br />
Bij het kleuren van gels tijdens elektroforetische proteïneseparatie.<br />
BELANGRIJK : De kleuroplossing is ontwikkeld voor het kleuren van een maximum van 10 gels. Na het kleuren van 10 gels dient u de oplossing te<br />
vervangen.<br />
Opslag, stabiliteit en tekenen van verval<br />
Zowel de standaard als de gebruiksoplossingen dienen bij kamertemperatuur of gekoeld bewaard te worden in gesloten containers om verdamping<br />
te voorkomen. De standaard kleuroplossing is stabiel tot de houdbaarheidsdatum zoals deze is aangegeven op de verpakking van de kit of op het<br />
label van de flesjes met kleuroplossing.<br />
De gebruiksoplossing is gedurende 1 maand stabiel.<br />
De verdunde oplossing kleurstof niet in de buurt van een warmtebron bewaren.<br />
5. ONTKLEURINGSOPLOSSING<br />
Voorbereiding<br />
Elk flesje ontkleuringconcentraat wordt verdund tot 100 liter met gedestilleerd of gedeïoniseerd water. Het is praktisch om een verdunning van een<br />
klein deel, bijv. 1/1000 van het concentraat aan te maken, bijvoorbeeld 1 ml concentraat te verdunnen tot 1 liter. Na verdunning bevat de<br />
ontkleuringoplossing: citroenzuur, 0,5 g/l.<br />
Gebruik<br />
Voor het ontkleuren van gels, d.w.z. het verwijderen van overtollige en achtergrondkleur uit de gels.<br />
Opslag, stabiliteit en tekenen van verval<br />
De concentraat-ontkleuringsoplossing is stabiel bij kamertemperatuur of gekoeld tot de houdbaarheidsdatum zoals aangegeven op de verpakking of<br />
de labels op de flesjes met ontkleuringoplossing. De verdunde ontkleuringoplossing is, in een afgesloten fles en bij kamertemperatuur, gedurende<br />
1 week stabiel.<br />
Verwijder de verdunde ontkleuringoplossing zodra er uiterlijke veranderingen optreden, bijvoorbeeld als hij troebel wordt als gevolg van besmetting<br />
met microben.<br />
Voeg geen natriumazide toe.<br />
Om besmetting met microben te voorkomen in een oplossing die langer dan een week bewaard moet worden voegt u 50 µl/l ProClin 300 toe.<br />
De verdunde, ProClin bevattende ontkleuringsoplossing blijft, indien bewaard in een afgesloten fles bij kamertemperatuur of in de koeling, stabiel tot<br />
aan de uiterste houdbaarheidsdatum die vermeld staat op de verpakking van de kit of op de etiketten van de flesjes ontkleuringsoplossing.
- 24 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
6. HEMOLYSERENDE OPLOSSING<br />
Voorbereiding<br />
De hemolyserende oplossing is gebruiksklaar. Dit is een buffer met toevoegingen, niet schadelijk in de gebruikte concentratie, doch noodzakelijk voor<br />
een optimale werking.<br />
Gebruik<br />
Voor de hemolyse van rode bloedcellen.<br />
Opslag, stabiliteit en tekenen van verval<br />
Bewaar de hemolyserende oplossing gekoeld of bij kamertemperatuur. Deze oplossing is stabiel tot de houdbaarheidsdatum zoals aangegeven op de<br />
verpakking of de labels op de flesjes met hemolyserende oplossing.<br />
Verwijder de hemolyserende oplossing zodra er uiterlijke veranderingen optreden, bijvoorbeeld als hij troebel wordt als gevolg van besmetting met<br />
microben.<br />
7. APPLICATORS<br />
Gebruik<br />
Voorgesneden applicatoren, voor eenmalig gebruik, voor het aanbrengen van de monsters.<br />
Opslag<br />
De applicatorstrips worden op een droge plaats bij kamertemperatuur of gekoeld bewaard.<br />
8. FILTERSTRIPS - DUN<br />
Gebruik<br />
Velletjes dun filterpapier, voor eenmalig gebruik, voor het opnemen van overtollige vloeistof van het geloppervlak vóór het aanbrengen van de<br />
monsters.<br />
Opslag<br />
Bewaar de dunne velletjes filterpapier op een droge plaats bij kamertemperatuur of in de koeling.<br />
BENODIGDE, NIET BIJGELEVERDE REAGENTIA<br />
1. FYSIOLOGISCHE ZOUTOPLOSSING<br />
Voorbereiding<br />
Maak 0,15 M (9 g/l) NaCl-oplossing met gedestilleerd of gedeïoniseerd water.<br />
Gebruik<br />
Voor het wassen van rode bloedcellen en voor de verdunning van hemolysaten.<br />
Opslag, stabiliteit en tekenen van verval<br />
De zoutoplossing kan bij kamertemperatuur bewaard worden. Verwijder de oplossing na 3 maanden of wanneer er uiterlijke veranderingen optreden,<br />
bijvoorbeeld als hij troebel wordt als gevolg van besmetting met microben. Voor opslag gedurende langere perioden kan 1 g/l natriumazide worden<br />
toegevoegd.<br />
2. FIXEEROPLOSSING (optioneel)<br />
Voorbereiding<br />
Maak, ten minste 15 minuten vóór gebruik, een oplossing van de volgende bestanddelen (vol. / vol.): 60 % ethanol ; 10 % azijnzuur en<br />
30 % gedestilleerd of gedeïoniseerd water. Goed mengen.<br />
Gebruik<br />
Voor het fixeren van door middel van elektroforese gescheiden proteïnen in agarose gels.<br />
Opslag, stabiliteit en tekenen van verval<br />
De fixeeroplossing kan bij kamertemperatuur of gekoeld worden bewaard in een hermetisch afgesloten fles, om verdamping te voorkomen. Verwijder<br />
de oplossing na 3 maanden. Fixeer niet meer dan 4 gels per 150 ml fixeeroplossing.<br />
BENODIGDE UITRUSTING EN ACCESSOIRES<br />
1. Elektriciteitsvoorziening: GD 61 D SEBIA, Prod. nr. 1300 ; GD 251 D SEBIA, Prod. nr. 1301 ; MG 300 SEBIA, Prod. nr. 1302 of MG 500 SEBIA,<br />
Prod. nr. 1303.<br />
2. <strong>HYDRAGEL</strong> <strong>K20</strong> APPLICATOR SEBIA, prod. nr. 1409, bevat de <strong>HYDRAGEL</strong> <strong>K20</strong> applicatordrager.<br />
3. Kamer voor natte opslag, Prod. nr. 1270.<br />
4. Elektroforesekamer: <strong>K20</strong> SEBIA, prod. nr. 1400.<br />
5. Tanks en gelhouders voor de verwerking van gelplaten: <strong>HYDRAGEL</strong> <strong>K20</strong> Accessory Kit SEBIA, Prod. nr. 1420.<br />
6. Pipetten: 5 µl, 10 µl en 200 µl.<br />
7. Incubatordroger: IS 80 SEBIA, prod. nr. 1430.<br />
8. Densitometer / flat-bed scanner die gels van 82 x 51 mm kan scannen bij 570 nm (geelfilter), bijv.: HYRYS SEBIA, DVSE SEBIA of PHORESIS<br />
software voor flat-bed scanner. Voor de instructies met betrekking tot de installatie, werking en kalibratie wordt u naar de instructies van de<br />
fabrikant verwezen.<br />
MONSTERS VOOR ANALYSE<br />
Verzameling en opslag van monsters<br />
Verse bloedmonsters met anti-coaguleermiddel verdienen de voorkeur bij analyse (vermijd heparine jodiumacetaat als anti-coaguleermiddel).<br />
Algemeen toegepaste anti-coaguleermiddelen zoals de middel die EDTA, citroenzuur of heparine bevatten zijn geschikt ; vermijd het gebruik van<br />
middelen met jodiumacetaat. Het bloed moet volgens vastgestelde procedures, zoals toegepast bij testen in klinische laboratoria, verzameld worden.<br />
Indien nodig de monsters gekoeld (bij 2 tot 8 °C) opslaan gedurende 5 dagen.
- 25 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Voorbereiding van het monster<br />
• Het primaire buisje schudden voor u de totale hoeveelheid te behandelen bloed afneemt ;<br />
• Centrifugeer bloed met anticoaguleermiddel gedurende 5 minuten bij 5000 rpm ;<br />
• Verwijder het plasma ;<br />
• Spoel de rode bloedcellen 2 maal met 10 volumedelen fysiologische zoutoplossing ; zeer omzichtig dient men te werk te gaan bij de verwerking van<br />
volumedelen met rode bloedcellen kleiner dan 10 µl ;<br />
• Verwijder het surplus aan saline (fysiologische zoutoplossing) over de rode bloedcellen pellet en vortex deze alvorens 10 µL te nemen voor de<br />
hemolyse ;<br />
• Hemolyseer 10 µl rode bloedcellen met 130 µl hemolyserende oplossing ;<br />
• Meng dit gedurende 10 seconden in de vortexmixer, en laat het dan bij kamertemperatuur gedurende 5 minuten incuberen.<br />
OPMERKINGEN:<br />
- Om hemolysaat te prepareren van proefpersonen die licht anemisch (ongeveer 10 g/dl Hb) of ernstig anemisch ( < 7 g/dl Hb), kan het volume van<br />
verpakte RBC verhoogd worden tot respectievelijk 15 µl en 20 µl. De keuringsintensiteit zal zodoende toenemen, maar de relatieve concentraties<br />
van de afzonderlijke fracties zal niet veranderen ;<br />
- Het hemolysaat hoeft niet gefilterd of gecentrifugeerd te worden.<br />
- De hemolyserende oplossing van SEBIA heeft geen invloed op het onstabiele hemoglobine van Bart.<br />
PROCEDURE<br />
I. MIGRATIE<br />
1. Plaats de <strong>HYDRAGEL</strong> <strong>K20</strong> applicatordrager op een plat oppervlak (Fig. 1) en til het gedeelte van de applicatordrager op dat genummerde<br />
uitsparingen heeft.<br />
2. Giet 120 µl gedestilleerd of gedeïoniseerd water op het onderste 1/3 deel van het frame dat op de <strong>HYDRAGEL</strong> <strong>K20</strong> applicatordrager is gedrukt.<br />
3. Neem de <strong>HYDRAGEL</strong> agarose gel uit de verpakking.<br />
4. Rol een dun filter voorzichtig en gelijkmatig over het oppervlak om zo het teveel aan vloeistof te absorberen. Verwijder het filterpapier direct.<br />
WAARSCHUWING: Laat het filterpapier niet te lang in contact met de gel om uitdroging te vermijden.<br />
5. Plaats de gelplaat (met de gelzijde naar boven) met een zijde tegen de rand aan de onderzijde van het gedrukte frame (Fig. 2).<br />
6. Buig de gel en breng deze naar beneden in het eerder uitgegoten water (Fig. 2). Zorg er voor dat er geen luchtbellen onder de gel gevangen<br />
worden, dat het water onder de gehele gelplaat wordt verdeeld en dat de gel gepositioneerd is conform het frame.<br />
7. Breng de applicatordrager met de genummerde uitsparingen in de tussenpositie waarbij de schakelaar in de hoogste stand staat.<br />
8. Plaats een applicator op een plat oppervlak zodat de putnummers zich in de ‘rechterzijde omhoog’ positie bevinden (Fig. 3)<br />
9. Breng 10 µl op correcte wijze verdund serummonster aan in elke spleet. Laad de applicator binnen 2 minuten.<br />
- Gebruik de applicator zonder vertraging<br />
- Voor later gebruik (tot 8 uur later) plaatst u de applicator in een natte opslagruimte, met de ‘tanden’ omhoog (alleen aan het plastic frame<br />
dat de tanden beschermd vastpakken). Zorg er voor dat de opslagruimte gekoeld is en plaats de gelplaat direct voorafgaand aan gebruik<br />
op de <strong>HYDRAGEL</strong> <strong>K20</strong> applicatiedrager.<br />
Voor verdere informatie wordt u naar de bijsluiter van de natte opslagruimte verwezen.<br />
10. Breek het beschermende plastic frame van de tanden af.<br />
11. Plaats de monsterapplicator in positie nr. 4 op de applicatiedrager.<br />
BELANGRIJK: De nummers die op de monsterapplicator zijn gedrukt moeten voor u zichtbaar zijn (Fig. 4).<br />
12. Breng de applicatordrager naar beneden zodat de applicator in contact komt met het oppervlak van de gel. FORCEER DE CARRIERS NIET<br />
HELEMAAL NAAR BENEDEN!<br />
13. Na 1 minuut draait u de schakelaar om zodat de applicator omhoog gebracht kan worden. Verwijder de applicator.<br />
14. Plaats de gel in een geschikte elektroforesekamer, in overeenstemming met de polariteit die op de gel staat aangegeven, de onderzijde van<br />
de gel aan de kant van de kathode. Bij gebruik van de SEBIA <strong>K20</strong> kamer, plaatst u de <strong>HYDRAGEL</strong> op de brug, waarbij de gelkant naar<br />
beneden gericht wordt ; de gel moet op een afstand van ongeveer 1 cm van elke zijde in de buffer zakken.<br />
Voor meer details wordt u verwezen naar de bijsluiter in de verpakking van de <strong>K20</strong> kamer.<br />
15. Sluit de kamer aan op de stroomvoorziening.<br />
| MIGRATIECONDITIES | SEBIA <strong>K20</strong> |<br />
| Volume buffer per compartiment | 150 ml |<br />
| Totaal buffervolume | 300 ml |<br />
| Migratietijd | 15 minuten |<br />
| Constant voltage | 165 V<br />
| |<br />
Initiële stroom (per gel) | 7 ± 2 mA |<br />
16. Na migratie de kamer ontkoppelen en de gelplaat verwijderen.<br />
II. FIXATIE<br />
Bewerk de gels volgens een van de hierna beschreven methoden.<br />
Fixatie doormiddel van hete lucht (bijvoorkeur alleen in combinatie met de SEBIA IS 80 Incubatordroger) :<br />
Droog de gel volledig in de incubatordroger bij een temperatuur van 80 °C (gedurende tenminste 10 minuten).<br />
Fixatie doormiddel van een fixeeroplossing :<br />
1. Plaats de gelplaat in een gelhouder (geleverd als onderdeel van de SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong> Accessory Kit) voor verdere verwerking.<br />
2. Vul een container (geleverd als onderdeel van de SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong> Accessory Kit) met 150 ml fixeeroplossing.<br />
3. Dompel de gedroogde en gekoelde gel gedurende precies 15 minuten onder in de fixeeroplossing.<br />
4. Verwijder de gel en droog deze met een hete luchtstroom in de incubatordroger type IS-80, bij een temperatuur van 80 °C.<br />
BELANGRIJK: De gel moet volledig droog zijn!
- 26 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
III. KLEURING - ONTKLEURING<br />
1. Dompel de gedroogde en gekoelde gel gedurende 5 minuten onder in de kleuringoplossing.<br />
2. Ontkleur vervolgens in drie opeenvolgende baden met ontkleuringoplossing totdat de achtergrond volkomen kleurloos en helder is.<br />
3. Absorbeer de overtollige vloeistof op de gel met tissuepapier en droog de gel met hete lucht (80 °C). Indien nodig kunt u de achterzijde van<br />
de droge film met een natte tissue schoonmaken.<br />
IV. SCANNEN<br />
Scan met behulp van een densitometer / scanner met een geel filter of bij 570 nm. Bij het gebruik van de HYRYS of DVSE densitometers wordt de<br />
A 2 fractie op de 5 mm markering van de scanplaat geplaatst. De nulinstelling van de achtergrond wordt vastgesteld tussen de A 2 en de koolzure<br />
anhydrase fracties bij het laagste punt.<br />
OPMERKING :<br />
Om de meest nauwkeurige en consistente resultaten te garanderen, kunt u het volgende doen:<br />
- Stel de scanlengte bij zodat hij het gehele elektroforetische patroon omvat (30 mm)<br />
- De achtergrondnul wordt geplaatst vóór de koolzuur anhydrase fractie, op het laagste punt ;<br />
- Zorg ervoor dat de minima op de beide zijden van de A 2 fractie zich helemaal aan de basis van de A 2 piek bevinden.<br />
Het is een goede gewoonte om de gekleurde gels direct te interpreteren. Voor eventueel later gebruik kunnen de gels in een beschermende afdekking<br />
op een droge en donkere plaats, verwijderd van warmtebronnen bewaard worden en gedurende een periode van tenminste 3 maanden nog voor<br />
visuele interpretatie gebruikt worden.<br />
RESULTATEN<br />
Kwaliteitscontrole<br />
Het wordt aanbevolen een gekeurd controlebloedserum of een normaal controlebloedmonster dat de hemoglobinen A, F, C en S bevat, toe te voegen<br />
aan elke serie monsters.<br />
Waarden<br />
Scannen met de densitometer van gekleurde elektroforegrammen levert de relatieve concentraties (percentages) van de afzonderlijke proteïnezones op.<br />
Normale waarden (gemiddeld ± 2 SD) voor de afzonderlijke proteïnezones in <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>-gels zijn vastgesteld op basis van<br />
een gezonde populatie van 200 volwassenen (mannen en vrouwen):<br />
Hemoglobine A ≥ 96,5 %<br />
Hemoglobine F < 2 % (*)<br />
Hemoglobine A 2 ≤ 3,5 %<br />
(*) zie ook Interferentie en begrenzingen.<br />
Het wordt aanbevolen dat elk laboratorium zijn eigen normaalwaarden vaststelt.<br />
Interpretatie<br />
1. Kwalitatieve afwijkingen: hemoglobinopathiën<br />
De meeste hemoglobinopathiën worden veroorzaakt door substitutie van een enkel aminozuur in een van de vier typen polypeptideketens als gevolg<br />
van mutatie. De klinische betekenis van dergelijke veranderingen hangt af van het type aminozuur en de betrokken locatie. Bij een klinisch belangrijke<br />
ziekte wordt of de α- of de ß-keten aangetast.<br />
Er zijn inmiddels meer dan 200 varianten van volwassenenhemoglobine beschreven. De eerste abnormale hemoglobinen die werden bestudeerd en<br />
die het meest frequent voorkomen, hebben een gewijzigde elektrische lading, hetgeen detectie door middel van elektroforese eenvoudig maakt.<br />
De vier belangrijkste abnormale hemoglobinen die in een bepaald klinisch belang vertegenwoordigen zijn: S, C, E en D.<br />
De <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> kits zijn bedoeld voor de voorlopige identificatie van hemoglobinopathiën en thalassemiën. Als er eenmaal een<br />
abnormaal patroon wordt vastgesteld dan moet de identiteit door middel van de juiste onderscheidende test zoals elektroforese op zure agarose gels,<br />
worden bevestigd.<br />
Hemoglobine S<br />
Hemoglobine S is het meest frequent. Het komt voort uit een vervanging van een glutaminezuur (een zuur aminozuur) van de ß-keten door valine (een<br />
neutraal aminozuur). Zijn elektroforetische mobiliteit wordt hierdoor geringer. Op alkalisch gebufferde gels, <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>,<br />
migreert hemoglobine S tussen de A en A 2 fracties.<br />
Hemoglobine C<br />
Een glutaminezuur van de ß-keten wordt vervangen door lysine (een basisch aminozuur): de mobiliteit hiervan wordt sterk verminderd. Middels de<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure worden C, E en A 2 gesuperponeerd. Wanneer deze fractie is > 15 %, dient men verdacht te zijn op de<br />
aanwezigheid van hemoglobinen C en E.<br />
Hemoglobine E<br />
Een glutaminezuur van de ß-keten wordt vervangen door lysine (een basisch aminozuur): hemoglobine E migreert op exact dezelfde wijze als<br />
hemoglobine C gebruikmakend van de <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure. In tegenstelling tot hemoglobine C scheidt het zich echter niet<br />
af van hemoglobine A in een zure buffer [<strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>]. Deze eigenschap maakt onderscheid van E en C mogelijk.<br />
Hemoglobine D<br />
Een glutaminezuur van de ß-keten wordt vervangen door glutamine. Dit hemoglobine migreert op exact dezelfde wijze als hemoglobine S via de<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure. In tegenstelling tot hemoglobine S scheidt hemoglobine D zich echter niet af van hemoglobine A in<br />
een zure buffer [<strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>]. Deze eigenschap maakt onderscheid van S en D mogelijk.
2. Kwantitatieve afwijkingen: thalassemie<br />
- 27 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Thalassemie omvat een vrij heterogene groep genetische afwijkingen die gekarakteriseerd worden door een afgenomen synthese van een type van<br />
de polypeptideketens. Het moleculaire mechanisme achter deze afname is nog niet geheel beschreven.<br />
Er zijn twee typen thalassemie-syndroom bekend:<br />
Alfa-thalassemie<br />
Deze worden gekarakteriseerd door een afname van de synthese van de α-ketens, hetgeen vervolgens de synthese van de 3 fysiologische<br />
hemoglobinen aantast. Het exces aan synthese van ß- en α-ketens ten opzichte van α-ketens zorgt voor de vorming van tetrameren zonder α-keten.<br />
• hemoglobine Bart = γ 4,<br />
• hemoglobine H = ß 4.<br />
Bèta-thalassemie<br />
Deze worden gekarakteriseerd door de afname van de synthese van de ß-ketens. Alleen de synthese van hemoglobine A wordt beïnvloed. Daarom<br />
zijn de percentages hemoglobine F en hemoglobine A 2 hoger ten opzichte van hemoglobine A.<br />
3. Migratiepatronen<br />
Migratie van normale<br />
hemoglobinen<br />
A(A0 + A1 ) A (A0 + A1 )<br />
F<br />
S - D<br />
A2 A2 - C - E<br />
koolzure anhydrase koolzure anhydrase<br />
applicatiepunt<br />
A 0 : De niet-geglyceerde fractie van het normaal volwassenen hemoglobine A.<br />
A 1 : De geglyceerde fractie van het normaal volwassenen hemoglobine A.<br />
In de hierboven weergegeven patronen is de anodo beneden en de kathode aan de bovenzijde.<br />
Interferentie en begrenzingen<br />
• Gebruik geen gehemolyseerde bloedmonsters.<br />
• Als er een afwijkend hemoglobine wordt waargenomen dat zich anders gedraagt dan de belangrijkste hemoglobine varianten S, C, D en E, dan<br />
moeten andere identificatiemiddelen gebruikt worden (bijv. isoelectrische focussering, globine-keten elektroforese), of vraag advies bij of zend een<br />
monster aan, een gespecialiseerd laboratorium.<br />
• De densitometrische keuring van Hb F (of enig ander minder belangrijk hemoglobine dat in de buurt van de belangrijke fracties migreert) is semikwantitatief<br />
aangezien de waarden onnauwkeurig worden beneden de 2 - 3 % van het totale hemoglobine.<br />
• De monsters van bepaalde patiënten met een homozygote hemoglobine S, die behandeld zijn met Hydrea® (hydroxycarbamide) kunnen een<br />
hemoglobine F vertonen die door deze behandeling is gesynthetiseerd. Bij enkele gevallen heeft men kunnen waarnemen dat deze geïnduceerde<br />
hemoglobine F een mobiliteit heeft op de <strong>HYDRAGEL</strong> 7 <strong>HEMOGLOBIN</strong>(E)-gels die licht verschilt van die van de natuurlijke hemoglobine F.<br />
• Soms, wanneer monsters langer dan zeven dagen bewaard worden, kan er een geconcentreerde fractie worden waargenomen door de vlek die<br />
zich achter de Hb A-fractie bevindt. Deze fractie mag niet worden verward met een hemoglobinevariant, zoals bijvoorbeeld hemoglobine H of Bart.<br />
Troubleshooting<br />
Bel de technische dienst van de leverancier als de test mislukt terwijl de instructies voor de voorbereiding en opslag van materialen, en voor de<br />
procedure, nauwkeurig werden gevolgd.<br />
De veiligheidsbladen behorend bij de reagentia in de Kit als ook informatie over de verwerking van afval of restproducten kunt u verkrijgen bij de<br />
Technische Dienst van de leverancier.<br />
UITSLAGGEGEVENS<br />
Migratie van belangrijke<br />
afwijkende hemoglobinen<br />
Alle uitslaggegevens zijn gebaseerd op een studie in meerdere laboratoria waarbij de <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure en een ander<br />
op de markt verkrijgbaar agarose gelsysteem werd toegepast. In aanvulling hierop werden concordantiestudies uitgevoerd waarbij de identiteit van de<br />
hemoglobinen en hun waarden werden vastgesteld met behulp van andere, geaccepteerde, methoden. De resultaten van representatieve voorbeelden<br />
van de studies worden hier gepresenteerd.<br />
Alle elektroforegrammen zijn visueel geïnterpreteerd. SEBIA’s HYRYS densitometer werd bij alle densitometrische evaluaties toegepast om waar<br />
nodig de visuele informatie aan te vullen.<br />
Reproduceerbaarheid binnen een serie<br />
Er werd elektroforese uitgevoerd op drie bloedmonsters, op een enkele partij gels gebruikmakend van de <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong><br />
procedure. Elk van de monsters werd getest in alle tracks van een enkele gel. De onderstaande tabel toont de gemiddelden, SD en CV voor ieder<br />
afzonderlijk hemoglobinecomponent in de drie monsters, berekend aan de hand van de densitometrische percentage waarden voor ieder track. Verder<br />
zijn bij geen van de herhalingen valse negatieve of valse positieve waarden geconstateerd.
- 28 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
| COMPONENT | GEMIDDELDE | SD | CV (%) |<br />
| Normaal bloed |<br />
| Hb A | 97.4 | 0.1 | 0.1 |<br />
| Hb A | 2 2.6 | 0.1 | 5.3 |<br />
| Verhoogd Hb A2 |<br />
| Hb A | 95.2 | 0.2 | 0.2 |<br />
| Hb A | 2 4.8 | 0.2 | 4.4 |<br />
| Verhoogd Hb C |<br />
| Hb A | 56.7 | 0.4 | 0.8 |<br />
| Hb C | 43.3 | 0.4 | 1.0 |<br />
Reproduceerbaarheid tussen series<br />
Er werd elektroforese uitgevoerd op bloedmonsters, gebruikmakend van de <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure, op gels uit een enkele<br />
partij. Onder de geanalyseerde monsters bevonden zich zeven monsters met een afwijkend hemoglobine (Hb S, Hb F of Hb C), twee monsters met<br />
een verhoogd Hb A 2 , en de rest bestond uit normale bloedmonsters. De gemiddelden, SD en CV werden berekend aan de hand van de gegevens die<br />
verkregen waren voor iedere component in elk monster. De spreiding van de gemiddelden, SD en CV, en de gemiddelde CV die de verzamelde<br />
afzonderlijke componenten vertegenwoordigt, zijn in onderstaande tabel weergegeven. Verder zijn bij geen van de herhalingen valse negatieve of<br />
valse positieve waarden geconstateerd.<br />
| COMPONENT | GEMIDDELDE | SD | CV (%) | GEMIDDELDE CV (%) |<br />
| Hb A | 18.0 - 97.8 | 0.1 - 1.0 | 0.1 - 4.0 | 0.8 |<br />
| Hb F | 13.3 - 76.3 | 0.5 - 0.6 | 0.7 - 3.4 | 1.8 |<br />
| Hb C | 21.5 - 43.5 | 0.2 - 0.3 | 0.6 - 1.1 | 0.8 |<br />
| Hb S/D | 9.7 - 84.1 | 0.1 - 0.6 | 0.4 - 2.6 | 1.1<br />
| |<br />
Hb A | 2 2.2 - 5.7 | 0.1 - 0.2 | 2.3 - 7.6 | 4.0 |<br />
Nauwkeurigheid - detectie van hemoglobineafwijkingen<br />
Drieënzestig (63) verschillende bloedmonsters werden geanalyseerd met behulp van de <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure en een ander<br />
op de markt verkrijgbaar agarose gelsysteem. De bloedmonsters en hun diagnostische beoordeling werden geleverd door een ziekenhuis. De<br />
diagnose was gebaseerd op een routine alkalische gel en zure gel elektroforese en/of HPLC. Alle afwijkende hemoglobinen of afwijkende niveaus van<br />
normale hemoglobinen die met de <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure werden gedetecteerd, kwamen overeen met het vergelijkende<br />
gelsysteem, de ziekenhuisresultaten en de klinische diagnose. Er werden geen gevallen aangetroffen van incorrecte positieven, d.w.z. detectie van<br />
een afwijkende band of een afwijkend niveau van een normale band waar een dergelijke afwijking niet bestond in de realiteit.<br />
Nauwkeurigheid - kwantitatieve determinering van Hb A 2<br />
De Hb A 2 niveaus werden gemeten bij 51 bloedmonsters met normale en verhoogde Hb A 2 niveaus door middel van densitometrie van de<br />
elektroforetische scheidingen verkregen met de <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> procedure. De gemeten waarden uit de procedure werden<br />
geanalyseerd met een statistische lineaire regressie procedure en verscheidene statistische hulpmiddelen voor aanname/verwerping van de<br />
nulhypothese van geen verschil tussen twee procedures. De resultaten van de lineaire regressie analyse worden in onderstaande tabel weergegeven<br />
(y = <strong>HYDRAGEL</strong>).<br />
| Correlatie | y-Intercept | Helling | Spreiding van % waarden |<br />
| coëfficiënt | | | (SEBIA-systeem) |<br />
| 0.973 | -0.344 | 0.963 | 1.5 - 5.7 |<br />
BIBLIOGRAFIE<br />
1. Fairbanks V.F., ed. (1980) Hemoglobinopathies and thalassemia: Laboratory methods and case studies. Brian C. Decker, New York.<br />
2. Galacteros F. (1986) Thalassémie, drépanocytose et autres hémoglobinopathies. Techniques et Biologie, 3, 174-178.<br />
3. Huisman T.H.J. and. Jonxis J.H.P (1977) The hemoglobinopathies: techniques of identification. Marcel Dekker, New York.<br />
4. Krauss J.S., Drew P.A., Jonah M.H., Trinh M., Shell S., Black L. and Baisden C.R. (1986) Densitometry and microchromatography compared for<br />
determination of the hemoglobin C and A 2 proportions in hemoglobin C and hemoglobin SC disease and in hemoglobin C trait. Clin. Chem. 32, 5,<br />
860-863.<br />
5. Livingstone C. (1986) The hemoglobinopathies. Edit. London.<br />
6. Maier-Redelsberger M., Girot R. (1989) Diagnostic biologique des maladies de l’hémoglobine. Feuillets de biologie, 170.<br />
7. Schneider R.G. (1978) Methods for detection of hemoglobin variants and hemoglobinopathies in the routine clinical laboratory. CRC Crit. Rev. Clin.<br />
Lab. Sci. 9, 243-271.<br />
8. Vovan L., Lara-Russo D., Orsini A. (1985) Diagnostic biologique des hémoglobinoses. Ann. Pédiat. 32, 9, 780-789.
UTILIZZO<br />
- 29 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Il kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> è stato progettato per la separazione delle emoglobine normali (A e A 2 ) e per la rivelazione delle maggiori<br />
varianti dell’emoglobina: S o D e C o E mediante elettroforesi su gel di agarosio tamponato in mezzo alcalino. Gli elettroforegrammi risultanti sono<br />
interpretati visivamente per la valutazione dei quadri anormali. La densitometria trova applicazione pratica nell’aiuto all’interpretazione dei quadri<br />
elettroforetici, fornendo la quantificazione relativa delle singole frazioni. Per confermare l’identificazione delle emoglobine varianti, in particolare per<br />
differenziare l’emoglobina S dalla D e la E dalla C, dovrebbe essere eseguita l’elettroforesi su gel acido, utilizzando la metodica <strong>HYDRAGEL</strong> ACID(E)<br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>.<br />
Ogni gel di agarosio del kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, permette di processare 7 campioni.<br />
Per uso diagnostico in vitro.<br />
PRINCIPIO DEL METODO<br />
L’emoglobina è una molecola complessa composta da due coppie di catene polipeptidiche. Ogni catena è collegata all’eme, un nucleo tetrapirrolico<br />
(porfirina) chelato ad un atomo di ferro. L’eme è comune a tutte le emoglobine e alle loro varianti. Il tipo di emoglobina è determinato dalla parte<br />
proteica chiamata globina. Le catene polipeptidiche α, ß, δ e γ costituiscono le emoglobine umane normali:<br />
• emoglobina A....................... = α 2 ß 2<br />
• emoglobina A 2 ..................... = α 2 δ 2<br />
• emoglobina fetale F............. = α 2 γ 2<br />
La catena α è comune a queste tre emoglobine.<br />
La struttura spaziale e le altre proprietà molecolari dell’emoglobina (come quelle di tutte le proteine), dipendono dalla natura e dalla sequenza degli<br />
aminoacidi che formano le catene. La sostituzione di un aminoacido per mutazione è responsabile della formazione di emoglobine varianti che hanno<br />
differenti cariche superficiali e quindi diversa mobilità elettroforetica, in funzione anche del pH e della forza ionica del tampone.<br />
Le risultanti anomalie qualitative (o strutturali) sono chiamate emoglobinopatie. La diminuzione di sintesi di una delle catene emoglobiniche, comporta<br />
anormalità di tipo quantitativo (o di regolazione), denominate talassemie.<br />
L’analisi è eseguita con emolisato di globuli rossi lavati. Le emoglobine sono separate elettroforeticamente su gels alcalini e le frazioni sono colorate<br />
con una soluzione di amidoschwarz. I gels essiccati sono pronti per l’interpretazione.<br />
REAGENTI E MATERIALI FORNITI NEL KIT <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong><br />
| COMPONENTI | PN 3010 |<br />
| Gels di Agarosio (pronti all’uso) | 10 gels |<br />
| Tampone tris-barbital (soluzione concentrata) | 3 flaconi da 75 mL |<br />
| Diluente per la soluzione colorante (soluzione concentrata) | 1 flacone da 60 mL |<br />
| Colorante Amidoschwarz (soluzione concentrata) | 1 flacone da 20 mL |<br />
| Soluzione decolorante (soluzione concentrata) | 1 flacone da 100 mL |<br />
| Soluzione emolizzante (pronta all’uso) | 1 flacone da 20 mL |<br />
| Applicatori a 7 dentini (pronti all’uso) | 1 confezione da 10<br />
|<br />
|<br />
Cartine da filtro – Sottili | 1 confezione da 10 |<br />
PER RISULTATI OTTIMALI<br />
I componenti di uno stesso kit devono sempre essere utilizzati insieme, in accordo con le istruzioni contenute nel kit.<br />
LEGGERE ATTENTAMENTE LE ISTRUZIONI PER L’USO.<br />
1. GELS DI AGAROSIO<br />
Preparazione<br />
I gels di agarosio sono pronti all’uso. Ogni gels di agarosio contiene: agarosio, 0.8 g/dL ; tampone alcalino pH 8.5 ± 0.1 ; additivi, non rischiosi alle<br />
concentrazioni usate, necessari per ottimizzare l’analisi.<br />
Utilizzo<br />
Mezzo di supporto per elettroforesi delle emoglobine.<br />
Conservazione, stabilità e segni di deterioramento<br />
Conservare i gels orizzontalmente, nella confezione originale protettiva, a temperatura ambiente (15 - 30 °C) o in frigorifero (2 - 8 °C). I gels sono<br />
stabili fino alla data di scadenza indicata sulla scatola del kit o sulla confezione del gel. (La freccia sulla scatola del kit deve essere rivolta verso l’alto).<br />
Evitare, durante la conservazione, significative variazioni di temperatura (es., non conservare in prossimità di finestre o di sorgenti di calore).<br />
NON CONGELARE.<br />
Non utilizzare il gel quando:<br />
(i) sono presenti cristalli o precipitati sulla superficie del gel oppure la struttura del gel è divenuta molto molle (entrambe conseguenze del<br />
congelamento del gel),<br />
(ii) è presente muffa o flora batterica,<br />
(iii) è presente, nella scatola che contiene il gel, una quantità anormale di liquido (risultato di una fuoriuscita del tampone dal gel dovuta a condizioni<br />
di conservazione improprie).<br />
2. TAMPONE TRIS-BARBITAL<br />
Preparazione<br />
Ogni flacone di soluzione tampone concentrata deve essere diluito ad 1 litro con acqua distillata o deionizzata. Dopo la diluizione, la soluzione di<br />
utilizzo contiene: tris-barbital pH 9.2 ± 0.3 ; sodio azide.<br />
FOGLIO DI ISTRUZIONI SEBIA - Italiano
- 30 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
AVVERTENZA: Ogni flacone di tampone in soluzione concentrata contiene 2.45 % di barbital, 13.73 % di barbital sodico e 0.13 % di sodio<br />
azide. Non ingerire! Se ingerito consultare immediatamente un medico! Evitare il contatto con acidi, piombo o rame poiché possono<br />
originare composti esplosivi o tossici con la sodio azide. Quando smaltito, fare scorrere un’abbondante quantità d’acqua.<br />
Utilizzo<br />
Tampone per elettroforesi.<br />
Conservazione, stabilità e segni di deterioramento<br />
Conservare la soluzione concentrata a temperatura ambiente o refrigerata. La soluzione concentrata è stabile fino alla data di scadenza indicata sulla<br />
confezione del kit o sull’etichetta del flacone di tampone. La soluzione tampone diluita è stabile per un anno se conservata a temperatura ambiente<br />
in un flacone chiuso.<br />
Eliminare la soluzione tampone diluita se muta di aspetto, per esempio, diviene torbida a causa di contaminazioni batteriche.<br />
3. DILUENTE PER LA SOLUZIONE COLORANTE<br />
Preparazione<br />
Il diluente per il colorante deve essere utilizzato come descritto nel paragrafo "COLORANTE AMIDOSCHWARZ".<br />
Contiene una soluzione acida.<br />
Utilizzo<br />
Per la preparazione della soluzione colorante amidoschwarz.<br />
Conservazione, stabilità e segni di deterioramento<br />
Conservare il diluente concentrato per il colorante a temperatura ambiente o in frigorifero. E’ stabile fino alla data di scadenza indicata sulla scatola<br />
del kit o sull’etichetta del diluente. NON CONGELARE.<br />
Non aggiungere sodio azide.<br />
4. COLORANTE AMIDOSCHWARZ<br />
Preparazione<br />
Il colorante amidoschwarz concentrato è una soluzione viscosa, che può eventualmente gelificare, senza che la qualità della soluzione finale e del<br />
suo potere colorante siano minimamente alterati.<br />
Per ottenere una perfetta ricostituzione del colorante, bisogna rispettare il seguente protocollo.<br />
1. Aggiungere circa 15 mL di diluente del colorante al flacone di amidoschwarz concentrato.<br />
2. Chiudere accuratamente il flacone.<br />
3. Agitare con molto vigore il flacone per almeno 5 secondi.<br />
4. Versare la soluzione ottenuta nel recipiente di preparazione della soluzione di colorazione.<br />
5. Ripetere questa operazione due o tre volte se necessario.<br />
6. Versare il resto del diluente nel recipiente di preparazione della soluzione di colorazione.<br />
7. Completare a 300 mL con acqua distillata o demineralizzata.<br />
8. Agitare perfettamente questa soluzione per 5 - 10 minuti.<br />
Il colorante è pronto all’uso.<br />
Dopo la diluizione, la soluzione di colorante contiene: soluzione acida pH ≈ 2 ; amidoschwarz, 4 g/L ; Etilen-glicol, 6,7 % ; componenti, non pericolosi<br />
alle concentrazioni utilizzate, necessarie per i risultati ottimali.<br />
AVVERTENZA: Nocivo in caso di ingestione.<br />
Utilizzo<br />
Per la colorazione dei gels dopo la separazione elettroforetica delle proteine.<br />
IMPORTANTE: La soluzione colorante è destinata alla colorazione di solamente 10 gels. Sostituire la soluzione colorante dopo 10 cicli di colorazione.<br />
Conservazione, stabilità e segni di deterioramento<br />
Conservare sia la soluzione concentrata del colorante sia quella diluita a temperatura ambiente o in frigorifero, in contenitore chiuso per prevenire<br />
l’evaporazione. La soluzione concentrata del colorante è stabile fino alla data di scadenza indicata sulla scatola del kit o sull’etichetta del colorante.<br />
Il colorante diluito è stabile 1 mese.<br />
Non conservare la soluzione di colorante diluita in prossimità di una sorgente di calore.<br />
5. SOLUZIONE DECOLORANTE<br />
Preparazione<br />
Il flacone di soluzione decolorante deve essere diluito a 100 litri con acqua deionizzata o distillata. Per convenienza diluire 1 mL di soluzione<br />
concentrata ad un litro.<br />
Dopo la diluizione, la soluzione decolorante contiene: acido citrico, 0.05 g/dL.<br />
Utilizzo<br />
Come decolorante, ossia per rimuovere l’eccesso di colorante e la colorazione di fondo dal gel.<br />
Conservazione, stabilità e segni di deterioramento<br />
Conservare la soluzione decolorante concentrata a temperatura ambiente o refrigerata. La soluzione concentrata è stabile fino alla data di scadenza<br />
indicata sulla scatola del kit o sull’etichetta del decolorante. La soluzione diluita del decolorante è stabile per una settimana a temperatura ambiente<br />
in flacone chiuso.<br />
Eliminare la soluzione decolorante diluita se muta d’aspetto, per esempio, diviene torbida a causa di contaminazioni microbiche.<br />
Non aggiungere sodio azide.<br />
Per periodi di conservazione superiori ad una settimana, prevenire i fenomeni di proliferazione microbica aggiungendo, nella soluzione decolorante<br />
diluita, 5 µL/dL di ProClin 300.<br />
La soluzione decolorante diluita addizionata con ProClin e conservata a temperatura ambiente o in frigorifero in bottiglia chiusa, è stabile fino alla data<br />
di scadenza indicata sulla confezione o sull’etichetta del flacone di decolorante.<br />
6. SOLUZIONE EMOLIZZANTE<br />
Preparazione<br />
La soluzione emolizzante è pronta all’uso. Costituita da tampone con additivi, non rischiosi alle concentrazioni utilizzate, necessari per ottimizzare<br />
l’analisi.<br />
Utilizzo<br />
Per emolizzare i globuli rossi.
- 31 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Conservazione<br />
Conservare la soluzione emolizzante a temperatura ambiente o refrigerata. La soluzione concentrata è stabile fino alla data di scadenza indicata sulla<br />
scatola del kit o sull’etichetta del flacone.<br />
Eliminare la soluzione emolizzante se muta d’aspetto, per esempio, diviene torbida a causa di contaminazioni microbiche.<br />
7. APPLICATORI<br />
Utilizzo<br />
Applicatori monouso pretagliati, per l’applicazione dei campioni sul gel.<br />
Conservazione<br />
Conservare gli applicatori in un luogo asciutto, a temperatura ambiente o in frigorifero.<br />
8. CARTINE DA FILTRO - SOTTILI<br />
Utilizzo<br />
Cartine assorbenti, monouso, per eliminare l’eccesso di liquido dalla superficie del gel, prima dell’applicazione del campione.<br />
Conservazione<br />
Conservare le cartine da filtro sottili in luogo secco a temperatura ambiente o in frigorifero.<br />
REAGENTI RICHIESTI MA NON FORNITI<br />
1. SOLUZIONE FISIOLOGICA<br />
Preparazione<br />
Preparare una soluzione 0.15 M (0.9 g/dL) di NaCl in acqua distillata o deionizzata.<br />
Utilizzo<br />
Per il lavaggio dei globuli rossi.<br />
Conservazione, stabilità e segni di deterioramento<br />
Conservare a temperatura ambiente o refrigerata. Eliminare comunque dopo 3 mesi oppure se muta di aspetto, es., diviene torbida a causa di<br />
contaminazione microbica. Per una conservazione più lunga aggiungere sodio azide, 0.1 g/dL.<br />
2. SOLUZIONE FISSATIVA (facoltativa)<br />
Preparazione<br />
Almeno 15 minuti prima dell’utilizzo preparare una soluzione contenente (vol./vol.): 60 % etanolo, 10 % acido acetico, e 30 % acqua distillata o<br />
deionizzata. Agitare bene.<br />
Utilizzo<br />
Per fissare le emoglobine separate elettroforeticamente su gel di agarosio.<br />
Conservazione, stabilità e segni di deterioramento<br />
Conservare a temperatura ambiente in flacone chiuso, per evitare l’evaporazione. Non fissare più di quattro gel con i medesimi 150 mL di fissativo.<br />
Eliminare dopo tre mesi.<br />
APPARECCHIATURE ED ACCESSORI RICHIESTI MA NON FORNITI<br />
1. Alimentatore: GD61D SEBIA, PN 1300 ; GD251D SEBIA, PN 1301 ; MG300 SEBIA, PN 1302 o MG500 SEBIA, PN 1303.<br />
2. APPLICATORE <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA, PN 1409, contenente il porta applicatori <strong>HYDRAGEL</strong> <strong>K20</strong>.<br />
3. Camera umida di conservazione, PN 1270.<br />
4. Camera elettroforetica: <strong>K20</strong> SEBIA, PN 1400.<br />
5. Vaschette e telai porta gel per processare le lastrine di gel: Kit Accessori <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA, PN 1420.<br />
6. Pipette: 5 µL, 10 µL e 200 µL.<br />
7. Essiccatore-incubatore: IS 80 SEBIA, PN 1430.<br />
8. Densitometro / Scanner in grado di effettuare la scansione di gels 82 x 51 mm a 570 nm (filtro giallo): HYRYS SEBIA, DVSE SEBIA o programma<br />
PHORESIS per Scanner a piano fisso. Fare riferimento alle istruzioni del produttore per le procedure di lavoro e di calibrazione.<br />
CAMPIONI PER L’ANALISI<br />
Raccolta e conservazione del campione<br />
Per l’analisi sono consigliati campioni di sangue freschi trattati con anticoagulante. Sono utilizzabili i comuni anticoagulanti, come quelli contenenti<br />
EDTA, citrato o eparina ; evitare gli anticoagulanti con iodoacetato. I campioni di sangue devono essere prelevati seguendo la procedura<br />
convenzionale per i tests clinici di laboratorio. Se necessario conservare i campioni a 2 - 8 °C fino ad un massimo di 5 giorni.<br />
Preparazione del campione<br />
• Agitare la provetta primaria prima di prelevare il volume di sangue totale da trattare.<br />
• Centrifugare il sangue con anticoagulante a 5000 rpm per 5 minuti.<br />
• Eliminare il plasma.<br />
• Lavare i globuli rossi 2 volte con 10 volumi di soluzione fisiologica ; grande cura deve essere posta quando si trattano volumi di globuli rossi inferiori<br />
a 10 µl.<br />
• Eliminare l’eccesso di soluzione fisiologica sovranatante ai globuli rossi impaccati, quindi agitare con vortex prima di prelevare i 10 µL da emolisare.<br />
• Emolizzare 10 µl di globuli rossi impaccati con 130 µl di soluzione emolizzante.<br />
• Agitare per 10 secondi ed incubare per 5 minuti a temperatura ambiente.
- 32 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
NOTA:<br />
- Per preparare emolisati di soggetti lievemente anemici (Hb di circa 10 g/dL) o gravemente anemici (Hb < 7 g/dL), il volume di globuli rossi<br />
impaccati deve essere incrementato rispettivamente a 15 µl e a 20 µl. L’intensità della colorazione risulterà aumentata, ma le concentrazioni<br />
relative delle singole frazioni non cambieranno.<br />
- L’emolisato non deve essere filtrato o centrifugato.<br />
- La Soluzione Emolizzante SEBIA non ha effetti sulla stabilità dell’emoglobina Bart’s.<br />
PROCEDURA<br />
I. MIGRAZIONE<br />
1. Posizionare il porta applicatore <strong>HYDRAGEL</strong> <strong>K20</strong> su una superficie piana (Fig. 1) ed alzare la cornice porta applicatore (quella con le fessure<br />
numerate).<br />
2. Dispensare 120 µL di acqua distillata o deionizzata sul terzo inferiore del riquadro stampato sul porta applicatore <strong>HYDRAGEL</strong> <strong>K20</strong>.<br />
3. Estrarre il gel <strong>HYDRAGEL</strong> dalla confezione.<br />
4. Eliminare rapidamente l’eccesso di liquido in superficie, tamponando il gel con una carta assorbente sottile<br />
ATTENZIONE : Fate attenzione a non lasciare la carta da filtro troppo a lungo a contatto con il gel per evitarne la disidratazione.<br />
5. Posizionare la lastrina del gel (gel rivolto verso l’alto) con l’estremità inferiore a ridosso dello scalino alla base del riquadro (Fig. 2)<br />
6. Curvare il gel ed adagiarlo sulla goccia d’acqua (Fig. 2). Assicurarsi che non siano rimaste intrappolate bolle d’aria. L’acqua deve essere<br />
uniformemente stratificata sotto la lastrina di gel e questa deve essere allineata all’interno del riquadro stampato.<br />
7. Abbassare la cornice porta applicatore fino alla posizione intermedia, con la manopola ruotata in alto.<br />
8. Posizionare un applicatore su di una superficie piana con i numeri dei pozzetti orientati correttamente verso l’alto (Fig. 3).<br />
9. Applicare in ogni pozzetto 10 µL di campione emolizzato. Caricare l’applicatore entro 2 minuti.<br />
- Utilizzare l’applicatore senza alcun ritardo.<br />
- Per un utilizzo successivo (fino ad 8 ore), inserire l’applicatore nella camera umida di conservazione, con i dentini rivolti verso l’alto<br />
(maneggiare il depositore mediante la cornice protettiva in plastica), mantenendo l’intera camera in frigorifero e preparando la lastrina di gel,<br />
sul porta applicatore <strong>HYDRAGEL</strong> <strong>K20</strong>, appena prima dell’uso.<br />
Consultare l’inserto all’interno della confezione della camera umida per ulteriori dettagli.<br />
10. Staccare la cornice protettiva dei dentini dell’applicatore.<br />
11. Inserire l’applicatore sulla cornice mobile in posizione No. 4.<br />
IMPORTANTE: I numeri stampati sull’applicatore devono essere rivolti verso l’operatore (Fig. 4).<br />
12. Abbassare la cornice porta applicatore in modo che l’applicatore entri in contatto con la superficie del gel. NON FORZARE LA CORNICE AD<br />
ABBASSARSI ULTERIORMENTE.<br />
13. Dopo 1 minuto, ruotare la manopola per sollevare l’applicatore, rimuovere l’applicatore ed eliminarlo.<br />
14. Mettere il gel in un’appropriata camera elettroforetica, in accordo alla polarità indicata sul gel. Quando è utilizzata la camera SEBIA <strong>K20</strong>,<br />
posizionare il gel sul ponte in modo che la superficie del gel sia rivolta verso il basso ; il gel deve essere immerso per circa 1 cm nel tampone<br />
su entrambi i lati.<br />
Per ulteriori dettagli consultare l’inserto contenuto nella camera <strong>K20</strong>.<br />
15. Collegare la camera all’alimentatore.<br />
| CONDIZIONI DI MIGRAZIONE | SEBIA <strong>K20</strong> |<br />
| Volume di tampone per compartimento | 150 mL |<br />
| Volume totale di tampone | 300 mL |<br />
| Tempo di migrazione | 15 minuti |<br />
| Voltaggio costante | 165 V<br />
|<br />
|<br />
Amperaggio iniziale (un gel) | 7 ± 2 mA |<br />
16. Dopo la migrazione, scollegare la camera e rimuovere la lastrina di gel.<br />
II. FISSAZIONE<br />
Trattare i gels con una delle seguenti procedure.<br />
Fissazione con aria calda (raccomandata solo con essiccatore-incubatore SEBIA IS 80):<br />
Essiccare completamente il gel nell’incubatore-essiccatore ad 80 °C (per un minimo di 10 min.).<br />
Fissazione con soluzione fissativa<br />
1. Posizionare il gel nel telaio porta gel (fornito con il Kit Accessori <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA) per i trattamenti successivi.<br />
2. Riempire una vaschetta (fornita con il Kit Accessori <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA) con 150 mL di soluzione fissativa.<br />
3. Immergere verticalmente il gel nella soluzione fissativa per 15 minuti.<br />
4. Rimuovere il gel ed essiccarlo con un flusso di aria calda ad 80 °C nell’incubatore-essiccatore IS 80.<br />
IMPORTANTE: Il gel deve essere perfettamente essiccato.<br />
III. COLORAZIONE - DECOLORAZIONE<br />
1. Dopo l’essiccazione immergere verticalmente il gel asciugato e raffreddato nella soluzione colorante per 5 minuti.<br />
2. Decolorare in tre successivi bagni di soluzione decolorante fino a quando il gel è privo di colorazione di fondo.<br />
3. Rimuovere l’eccesso di liquido sulla superficie del gel con una cartina assorbente ed essiccare il gel con aria calda ad 80 °C. Se necessario<br />
pulire il retro della lastrina (faccia di supporto) con carta morbida inumidita.
- 33 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
IV. SCANSIONE<br />
Effettuare la scansione usando un densitometro / scanner con filtro giallo o a 570 nm.<br />
Quando si utilizza uno dei densitometri HYRYS o DVSE, posizionare la frazione A 2 sul segno dei 5 mm della piastra di lettura: lo zero è effettuato, nel<br />
punto più basso, tra le frazioni A 2 e anidrasi carbonica.<br />
NOTA: Per assicurare i risultati più accurati e precisi, attenersi alla seguente procedura:<br />
- Regolare la lunghezza di scansione per includere l’intero quadro elettroforetico (30 mm).<br />
- Assicurarsi che i minimi, su ambedue i lati della frazione A 2 , siano posti ai piedi del picco.<br />
E’ buona prassi leggere i gels colorati senza ritardi. Per consultazioni successive, possono essere conservati in un astuccio protettivo, all’asciutto,<br />
protetti dalla luce e lontani da fonti di calore ed interpretati visivamente entro 3 mesi.<br />
RISULTATI<br />
Controllo Qualità<br />
Si consiglia di includere, in ogni gruppo di campioni processati, un sangue di controllo o un campione di sangue noto contenente emoglobine A, F, C e S.<br />
Valori<br />
La lettura densitometrica degli elettroforegrammi colorati, fornisce le concentrazioni relative (percentuali) delle singole zone proteiche.<br />
I valori normali (media ± 2 DS), utilizzando la metodica <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, sono stati determinati su una popolazione sana di<br />
200 adulti (uomini e donne) :<br />
Emoglobina A ≥ 96,5 %<br />
Emoglobina F < 2,0 % (*)<br />
Emoglobina A2 ≤ 3,5 %<br />
(*) vedi Interferenze e limitazioni<br />
Si raccomanda ad ogni laboratorio di stabilire i propri valori normali.<br />
Interpretazioni<br />
1. Anomalie qualitative: Emoglobinopatie<br />
La maggior parte delle emoglobinopatie sono dovute alla sostituzione, per mutazione, di un singolo aminoacido in una dei quattro tipi di catene<br />
polipeptidiche. Il significato clinico della mutazione varia in funzione del tipo di aminoacido e della posizione coinvolti. Nelle malattie clinicamente<br />
significative, è affetta la catena α o la catena ß (talvolta la catena γ).<br />
Più di 200 varietà di emoglobine adulte sono già state descritte. Le prime emoglobine anomale studiate, nonché le più numerose, presentano<br />
un’alterata carica elettrica netta e ciò ne consente una semplice individuazione attraverso l’elettroforesi.<br />
Sono quattro le principali emoglobine anomale che presentano un particolare interesse clinico: S, C, E e D.<br />
Il kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, è rivolto alla identificazione preliminare delle emoglobinopatie e delle talassemie. Quando si evidenzia un<br />
quadro anormale, l’identificazione deve essere confermata da un test discriminatorio appropriato (es., elettroforesi su gel di agarosio acido).<br />
Emoglobina S<br />
L’emoglobina S è la più frequente. E’ dovuta alla sostituzione di un acido glutammico (aminoacido acido) della catena ß, con valina (aminoacido<br />
neutro). La sua mobilità elettroforetica è quindi rallentata. Su <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> tamponato in mezzo alcalino, l’emoglobina S migra<br />
fra le frazioni A e A 2 .<br />
Emoglobina C<br />
Un acido glutammico della catena ß è sostituito dalla lisina (aminoacido basico): la sua mobilità è fortemente ridotta. Con la metodica <strong>HYDRAGEL</strong><br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, le emoglobine C, E ed A 2 sono sovrapposte. Quando questa frazione è superiore al 15 % deve essere sospettata la presenza<br />
di emoglobine C ed E.<br />
Emoglobina E<br />
Un acido glutammico della catena ß è sostituito dalla lisina: con la metodica <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, l’emoglobina E migra esattamente<br />
come la C. Diversamente dalla C, non si separa dalla A in tampone acido (<strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>). Questa proprietà permette<br />
di differenziare la E e la C.<br />
Emoglobina D<br />
Un acido glutammico della catena ß è sostituito dalla glutammina: su <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, l’emoglobina D migra esattamente come<br />
la S. Diversamente dall’emoglobina S, la D non si separa dalla A in tampone acido (<strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>). Questa proprietà<br />
permette di differenziare la S e la D.<br />
2. Anomalie quantitative: Talassemie<br />
Le talassemie costituiscono un gruppo pressoché eterogeneo di affezioni genetiche caratterizzate dalla riduzione del livello di sintesi di uno o più tipi<br />
di catena polipeptidica. Il meccanismo molecolare di questa riduzione non è stato ancora completamente descritto.<br />
Ci sono due tipi di sindromi talassemiche:<br />
Alfa-talassemie<br />
Sono caratterizzate da una ridotta sintesi delle catene α che, quindi, condiziona la sintesi di tutte le emoglobine normali.<br />
L’eccesso di sintesi delle catene ß e γ rispetto alla catena α, induce la formazione di tetrameri senza nessuna catena α:<br />
• Emoglobina Bart = γ 4,<br />
• Emoglobina H = ß 4.
- 34 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Beta-talassemie<br />
Sono caratterizzate da una riduzione di sintesi delle catene ß. Solo la sintesi dell’emoglobina A è compromessa. Ne consegue che la percentuale delle<br />
emoglobine F ed A 2 risulta incrementata rispetto alla A.<br />
3. Quadri di migrazione<br />
Migrazione di<br />
emoglobine normali<br />
A(A0 + A1 ) A (A0 + A1 )<br />
F<br />
S - D<br />
A2 A2 - C - E<br />
anidrasi anidrasi<br />
punto di applicazione<br />
A 0 : la frazione non glicata dell’emoglobina adulta normale A.<br />
A 1 : la frazione glicata dell’emoglobina adulta normale A.<br />
Nei quadri riprodotti, il catodo è in basso e l’anodo in alto<br />
Interferenze e limitazioni<br />
• Non utilizzare campioni di sangue emolizzati.<br />
• Quando è rilevata un’emoglobina anomala, che migra differentemente dalle principali emoglobine varianti S, C, D ed E, utilizzare un metodo<br />
d’identificazione diverso (es., isoelettrofocalizzazione, elettroforesi delle catene globiniche), o consultare o inviare il campione ad un laboratorio<br />
specializzato.<br />
• Il dosaggio densitometrico della Hb F (o di qualunque altra emoglobina minore che migri in prossimità di una frazione maggiore) è semi-quantitativo,<br />
poiché il valore diventa inaccurato quando inferiore al 2 - 3 % dell’emoglobina totale.<br />
• I campioni di alcuni pazienti con emoglobina omozigote “S”, trattati con Hydrea® (idrossiurea), possono presentare una emoglobina F dovuta alla<br />
sintesi indotta dal trattamento. Su <strong>HYDRAGEL</strong> 7 <strong>HEMOGLOBIN</strong>(E), in alcuni casi, è stata osservata una mobilità dell’emoglobina F indotta<br />
leggermente diversa da quella dell’emoglobina F fisiologica.<br />
• In campioni conservati per più di 7 giorni, può essere osservata una focalizzazione dell’addensamento localizzato dietro alla frazione Hb A, che non<br />
deve essere interpretato come una variante emoglobinica, es., emoglobine H o Bart.<br />
Eliminazione errori<br />
Contattare il Servizio di Assistenza Tecnica del fornitore quando, nonostante siano state seguite accuratamente le istruzioni per la preparazione e<br />
conservazione dei materiali e per la procedura di impiego, i risultati del test non rispettino le caratteristiche.<br />
Le Schede di Sicurezza dei componenti del kit e le informazioni per lo smaltimento dei rifiuti sono disponibili presso il Servizio di Assistenza Tecnica<br />
SEBIA.<br />
DATI SULLE PRESTAZIONI<br />
Migrazione delle principali<br />
emoglobine anormali<br />
Tutti i dati sulle prestazioni, sono basati su uno studio che comprende materiali e strumenti SEBIA <strong>HYDRAGEL</strong>, comparati ad un sistema in agarosio<br />
reperibile in commercio. Inoltre, sono stati eseguiti studi di correlazione quando l’identificazione delle emoglobine e dei loro valori erano stati stabiliti<br />
con altre metodiche validate. Di seguito sono presentati esempi rappresentativi degli studi sulle prestazioni. Tutti gli elettroforegrammi sono stati<br />
interpretati visivamente. Per le valutazioni densitometriche è stato utilizzato il densitometro SEBIA HYRYS.<br />
Riproducibilità nella serie<br />
Tre campioni di sangue sono stati processati con la metodica <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> su gels dello stesso lotto. Ogni campione è stato<br />
processato in tutte le piste del singolo gel. La tabella seguente riporta media, SD e CV di ogni componente emoglobinica dei tre campioni, calcolati<br />
dai valori percentuali densitometrici. Inoltre, nessuna ripetizione ha fornito dati falsamente positivi o negativi.<br />
| COMPONENTE | MEDIA | SD | CV (%) |<br />
| Campione normale |<br />
| Hb A | 97.4 | 0.1 | 0.1 |<br />
| Hb A | 2 2.6 | 0.1 | 5.3 |<br />
| Elevata Hb A2 |<br />
| Hb A | 95.2 | 0.2 | 0.2 |<br />
| Hb A | 2 4.8 | 0.2 | 4.4 |<br />
| Elevata Hb C |<br />
| Hb A | 56.7 | 0.4 | 0.8<br />
|<br />
|<br />
Hb C | 43.3 | 0.4 | 1.0 |<br />
Riproducibilità tra serie<br />
Campioni di sangue sono stati processati elettroforeticamente con la metodica <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, su gels di un singolo lotto. I<br />
campioni studiati ne includevano sette con emoglobine anormali (S, F o C), due con emoglobina A 2 elevata e i rimanenti normali. Le medie, SD e CV<br />
sono stati calcolati dai dati di ciascuna componente di ogni campione. Nella tabella seguente sono riportate le oscillazioni della media, della DS e del<br />
CV, oltre al CV medio, relative ai dati aggregati delle componenti. Inoltre, nessuna ripetizione ha fornito dati falsamente positivi o negativi
- 35 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
| COMPONENTE | MEDIA | DS | CV (%) | MEDIA CV (%) |<br />
| Hb A | 18.0 – 97.8 | 0.1 – 1.0 | 0.1 – 4.0 | 0.8 |<br />
| Hb F | 13.3 – 76.3 | 0.5 – 0.6 | 0.7 – 3.4 | 1.8 |<br />
| Hb C | 21.5 – 43.5 | 0.2 – 0.3 | 0.6 – 1.1 | 0.8 |<br />
| Hb S/D | 9.7 – 84.1 | 0.1 – 0.6 | 0.4 – 2.6 | 1.1<br />
| |<br />
Hb A | 2 2.2 – 5.7 | 0.1 – 0.2 | 2.3 – 7.6 | 4.0 |<br />
Accuratezza - Rilevamento delle Anomalie Emoglobiniche<br />
Utilizzando la metodica <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> ed un diverso sistema su gel di agarosio reperibile in commercio, sono stati analizzati<br />
63 campioni di sangue. I campioni di sangue e le loro valutazioni diagnostiche, sono stati forniti da un ospedale. Le diagnosi erano basate sui dati<br />
ottenuti da elettroforesi eseguite su gels acidi ed alcalini e/o da HPLC. Tutte le emoglobine anomale o i livelli alterati di emoglobine normali rilevate<br />
con <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, sono risultati concordanti con il sistema su gel di comparazione, con i risultati e le diagnosi cliniche<br />
dell’ospedale. Non sono stati osservati casi di falsa positività, per esempio, il rilevamento di una frazione anomala o di un livello alterato di una frazione<br />
normale, dove non esistevano anormalità.<br />
Accuratezza - Determinazione Quantitativa della Hb A 2<br />
Utilizzando sia le letture densitometriche di elettroforesi ottenute con <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, sia le letture con HPLC, sono stati misurati<br />
i livelli di Hb A 2 in 51 campioni di sangue con valori normali ed elevati di Hb A 2 . I valori misurati con le due tecniche sono stati analizzati con un test<br />
statistico di regressione lineare. I risultati della regressione lineare sono riportati in tabella (y = <strong>HYDRAGEL</strong>).<br />
| Coefficiente di correlazione | y- Intercetta | Pendenza | Variazione dei valori % |<br />
| | | | (sistema SEBIA) |<br />
| 0.973 | -0.344 | 0.963 | 1.5 – 5.7 |<br />
BIBLIOGRAFIA<br />
1. Fairbanks V.F., ed. (1980) Hemoglobinopathies and thalassemia: Laboratory methods and case studies. Brian C. Decker, New York.<br />
2. Galacteros F. (1986) Thalassémie, drépanocytose et autres hémoglobinopathies. Techniques et Biologie, 3, 174-178.<br />
3. Huisman T.H.J. and. Jonxis J.H.P (1977) The hemoglobinopathies: techniques of identification. Marcel Dekker, New York.<br />
4. Krauss J.S., Drew P.A., Jonah M.H., Trinh M., Shell S., Black L. and Baisden C.R. (1986) Densitometry and microchromatography compared for<br />
determination of the hemoglobin C and A 2 proportions in hemoglobin C and hemoglobin SC disease and in hemoglobin C trait. Clin. Chem. 32, 5,<br />
860-863.<br />
5. Livingstone C. (1986) The hemoglobinopathies. Edit. London.<br />
6. Maier-Redelsberger M., Girot R. (1989) Diagnostic biologique des maladies de l’hémoglobine. Feuillets de biologie, 170.<br />
7. Schneider R.G. (1978) Methods for detection of hemoglobin variants and hemoglobinopathies in the routine clinical laboratory. CRC Crit. Rev. Clin.<br />
Lab. Sci. 9, 243-271.<br />
8. Vovan L., Lara-Russo D., Orsini A. (1985) Diagnostic biologique des hémoglobinoses. Ann. Pédiat. 32, 9, 780-789.
ESPECIFICACIONES DE USO<br />
- 36 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
El kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> está diseñado para la separación de las hemoglobinas normales (A y A 2 ) y para la detección de las<br />
principales variantes de la hemoglobina: S ó D y C ó E, mediante electroforesis en geles de agarosa alcalinos. Las separaciones electroforéticas<br />
resultantes son evaluadas visualmente para la detección de anomalías en el patrón. La densitometría puede usarse como una ayuda en la<br />
interpretación al proporcionar las concentraciones relativas de las fracciones individuales. La electroforesis en geles ácidos, por ejemplo, el<br />
procedimiento <strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, debería utilizarse para confirmar la identificación de las variantes de hemoglobina y, en<br />
concreto, para diferenciar las hemoglobinas S de las D y las E de las C.<br />
Cada gel de agarosa en el kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> está destinado para analizar 7 muestras.<br />
Para Uso Diagnóstico In Vitro.<br />
PRINCIPIO DEL TEST<br />
La hemoglobina es una molécula compleja compuesta por dos pares de cadenas polipeptídicas. Cada cadena está ligada a un hemo, un núcleo<br />
tetrapirrólico (porfirina) al que está coordinado un átomo de hierro. La estructura hemo es común a todas las hemoglobinas y sus variantes. El tipo<br />
de hemoglobina está determinado por la parte proteica, llamada globina. Las cadenas polipeptídicas α, ß, δ y γ constituyen las hemoglobinas humanas<br />
normales:<br />
• hemoglobina A ................. = α 2 ß 2<br />
• hemoglobina A 2 ................ = α 2 δ 2<br />
• hemoglobina fetal F ......... = α 2 γ 2<br />
La cadena α es común a estas tres hemoglobinas.<br />
La estructura espacial de la hemoglobina y otras propiedades moleculares (como en todas las proteínas) depende de la naturaleza y la secuencia de<br />
los aminoácidos que forman las cadenas. La sustitución de aminoácidos por mutación es responsable de la formación de las variantes de la<br />
hemoglobina, que tienen una carga superficial diferente y, por consiguiente, movilidades electroforéticas diferentes, que también dependen del pH y<br />
de la fuerza iónica del tampón.<br />
Las anomalías cualitativas (o estructurales) resultantes se denominan hemoglobinopatías. La síntesis disminuida de una de las cadenas de la<br />
hemoglobina conlleva anomalías cuantitativas (o de regulación), denominadas talasemias.<br />
La técnica se realiza con glóbulos rojos lavados y hemolizados. Las hemoglobinas se separan mediante electroforesis en geles alcalinos y las<br />
fracciones se visualizan mediante tinción con negro amido. Los geles secos están listos para ser interpretados.<br />
REACTIVOS Y MATERIALES SUMINISTRADOS EN LOS KITS <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong><br />
| ARTÍCULOS | PN 3010 |<br />
| Geles de Agarosa (listos para usar) | 10 geles |<br />
| Tampón Tris-Barbital (solución stock) | 3 viales de 75 mL |<br />
| Diluyente del colorante (solución stock) | 1 vial, 60 mL |<br />
| Colorante Negro Amido (solución stock) | 1 vial, 20 mL |<br />
| Solución Decolorante (solución stock) | 1 vial, 100 mL |<br />
| Solución Hemolizante (lista para usar) | 1 vial, 20 mL |<br />
| Aplicadores de 7 dientes (listos para usar) | 1 caja de 10<br />
| |<br />
Papeles de Filtro - Finos | 1 paquete de 10 |<br />
PARA OBTENER RESULTADOS ÓPTIMOS<br />
Los elementos de un mismo kit deben utilizarse conjuntamente y según las instrucciones incluidas.<br />
LEER ATENTAMENTE LAS INSTRUCCIONES.<br />
1. GELES DE AGAROSA<br />
Preparación<br />
Los geles de agarosa están listos para su uso. Cada gel contiene: agarosa, 0.8 g/dL ; tampón alcalino pH 8.5 ± 0.1 ; aditivos, inocuos a las<br />
concentraciones usadas, necesarios para un funcionamiento óptimo.<br />
Uso<br />
Medio de soporte para la electroforesis de hemoglobinas.<br />
Almacenamiento, estabilidad y señales de deterioro<br />
Almacene los geles horizontalmente en sus recipientes protectores originales a temperatura ambiente (15 a 30 °C) o refrigerados (2 a 8 °C). (la flecha<br />
situada en la cara frontal de la caja del kit debe apuntar hacia arriba). Evite fluctuaciones de temperatura evidentes durante el almacenaje (por<br />
ejemplo, no los almacene cerca de una ventana o de una fuente de calor). Los geles son estables hasta la fecha de caducidad indicada en la caja<br />
del kit o en las etiquetas de sus recipientes protectores.<br />
NO LOS CONGELE.<br />
Deseche el gel cuando:<br />
(i) se formen cristales o precipitados en la superficie del gel o su textura sea muy blanda (consecuencias de la congelación del gel),<br />
(ii) se observe crecimiento bacteriano o fúngico,<br />
(iii) haya una cantidad de líquido excesiva en el estuche del gel (consecuencia de la exudación del tampón debida a un almacenamiento inadecuado).<br />
2. TAMPÓN TRIS-BARBITAL<br />
Preparación<br />
Cada vial de la solución stock del tampón se diluye hasta 1 litro con agua destilada o desionizada.<br />
Después de la dilución, la solución de trabajo contiene: tris-barbital pH 9.2 ± 0.3 ; azida sódica.<br />
INSTRUCCIONES SEBIA - Español
- 37 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
ADVERTENCIA: Cada vial de la solución stock del tampón contiene un 2.45 % de barbital, un 13.73 % de barbital sódico y un 0.13 % de<br />
azida sódica. ¡No lo ingiera! ¡Si lo ha ingerido consulte a un médico inmediatamente! Evite el contacto del producto con ácidos, plomo o<br />
cobre, ya que se conoce su tendencia a formar compuestos explosivos o tóxicos en contacto con la azida sódica. Lave siempre con gran<br />
cantidad de agua al desechar el producto.<br />
Uso<br />
Tampón de electroforesis.<br />
Almacenamiento, estabilidad y señales de deterioro<br />
Almacene la solución stock del tampón a temperatura ambiente o refrigerada. La solución stock es estable durante varios años, por lo menos hasta<br />
la fecha de caducidad indicada en la caja del kit o en las etiquetas del vial de tampón. La solución diluida del tampón es estable durante un año a<br />
temperatura ambiente en una botella cerrada.<br />
Deseche el tampón diluido si cambia su aspecto, por ejemplo, se vuelve turbio debido a contaminación microbiana.<br />
3. DILUYENTE DEL COLORANTE<br />
Preparación<br />
El diluyente del colorante concentrado debe ser usado como se ha descrito en el párrafo "COLORANTE NEGRO AMIDO". Contiene una solución<br />
ácida.<br />
Uso<br />
Para la preparación del colorante negro amido.<br />
Conservación, estabilidad y señales de deterioro<br />
El diluyente del colorante concentrado puede conservarse a temperatura ambiente o en la nevera. Es estable hasta la fecha de caducidad indicada<br />
en el kit o en la etiqueta del vial de diluyente. NO LO CONGELE.<br />
No le añada azida sódica.<br />
4. COLORANTE NEGRO AMIDO<br />
Preparación<br />
El colorante negro amido concentrado es una solución viscosa que puede gelificarse, lo que no afecta de ningún modo a la calidad de la solución<br />
final y su capacidad de coloración.<br />
Para obtener una perfecta reconstitución del colorante, siempre hay que prepararlo como se indica a continuación :<br />
1. Añada unos 15 mL de diluyente del colorante en el vial de negro amido concentrado.<br />
2. Cierre el vial con cuidado.<br />
3. Agite el vial intensamente durante un mínimo de 5 segundos.<br />
4. Vierta la solución obtenida en el recipiente de preparación de la solución de coloración.<br />
5. Repita esta operación dos veces, o tres veces si es necesario.<br />
6. Vierta el resto de diluyente en el recipiente de preparación de la solución de coloración.<br />
7. Complete hasta 300 mL con agua destilada o desionizada.<br />
8. Agite esta solución de 5 a 10 minutos.<br />
El colorante está listo para usar.<br />
Después de la dilución, la solución colorante contiene: solución ácida pH ≈ 2 ; negro amido, 4 g/L ; etilén-glicol, 6,7 % ; aditivos inocuos a las<br />
concentraciones usadas, necesarios para un funcionamiento óptimo.<br />
ATENCIÓN: Nocivo en caso de ingestión.<br />
Uso<br />
Para la coloración de los geles después de la separación electroforética de las proteínas.<br />
IMPORTANTE: El colorante está destinado para colorear sólo 10 geles. Cambie el colorante después de 10 usos.<br />
Conservación, estabilidad y señales de deterioro<br />
Las soluciones de colorante concentrada y diluida pueden conservarse a temperatura ambiente o en la nevera, en contenedores cerrados para evitar<br />
la evaporación. La solución concentrada es estable hasta la fecha de caducidad indicada en el kit o en la etiqueta del vial de colorante.<br />
La solución diluida es estable durante 1 mes.<br />
No almacene la solución de colorante diluida cerca de una fuente de calor.<br />
5. SOLUCIÓN DECOLORANTE<br />
Preparación<br />
Cada vial de la solución decolorante stock se diluye hasta 100 litros con agua destilada o desionizada. Es conveniente diluir sólo 1 mL de la solución<br />
stock hasta 1 litro. Después de la dilución, la solución de trabajo del decolorante contiene: ácido cítrico, 0.05 g/dL.<br />
Uso<br />
Para decolorar, esto es, eliminar el exceso de tinción y la coloración de fondo de los geles.<br />
Almacenamiento, estabilidad y señales de deterioro<br />
Almacene la solución decolorante stock a temperatura ambiente o refrigerada. Es estable hasta la fecha de caducidad indicada en la caja del kit o en<br />
las etiquetas del vial de decolorante. La solución decolorante de trabajo es estable durante una semana a temperatura ambiente en una botella<br />
cerrada.<br />
Deseche la solución decolorante de trabajo si cambia su aspecto, por ejemplo, se vuelve turbia debido a contaminación microbiana.<br />
No añada azida sódica.<br />
Para evitar la proliferación microbiana en la solución decolorante diluida que se vaya a almacenar durante más de una semana, añada 5 µL/dL de<br />
ProClin 300.<br />
El decolorante diluido al que se ha añadido ProClin es estable en un contenedor cerrado a temperatura ambiente o en la nevera hasta la fecha de<br />
caducidad indicada en el kit o en la etiqueta del vial de decolorante.<br />
6. SOLUCIÓN HEMOLIZANTE<br />
Preparación<br />
La Solución Hemolizante está lista para su uso. Es un tampón con aditivos, inocuos a las concentraciones usadas, necesarios para un funcionamiento<br />
óptimo.
Uso<br />
Para hemolizar los glóbulos rojos.<br />
- 38 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Almacenamiento, estabilidad y señales de deterioro<br />
Almacene la Solución Hemolizante a temperatura ambiente o refrigerada. Es estable hasta la fecha de caducidad indicada en la caja del kit o en las<br />
etiquetas del vial de Solución Hemolizante.<br />
Deseche la Solución Hemolizante si cambia su aspecto, por ejemplo, se vuelve turbia debido a contaminación microbiana.<br />
7. APLICADORES<br />
Uso<br />
Aplicadores precortados, de un solo uso, para la aplicación de las muestras.<br />
Almacenamiento<br />
Almacene los aplicadores en un lugar seco a temperatura ambiente o refrigerados.<br />
8. PAPELES DE FILTRO - FINOS<br />
Uso<br />
Papeles de filtro finos absorbentes, de un solo uso, para absorber el exceso de humedad de la superficie del gel antes de la aplicación de las<br />
muestras.<br />
Conservación<br />
Conserve los papeles de filtro finos en un lugar seco a temperatura ambiente o en nevera.<br />
REACTIVOS NECESARIOS PERO NO SUMNINISTRADOS<br />
1. SALINA<br />
Preparación<br />
Prepare una solución de NaCl 0.15 M (0.9 g/dL) con agua destilada o desionizada.<br />
Uso<br />
Para lavar los glóbulos rojos.<br />
Almacenamiento, estabilidad y señales de deterioro<br />
Almacene la salina a temperatura ambiente o refrigerada. Deséchela después de 3 meses o si cambia su aspecto, por ejemplo, se vuelve turbia<br />
debido a contaminación microbiana. Para periodos de almacenaje más prolongados, añada azida sódica, 0.1 g/dL.<br />
2. SOLUCIÓN FIJADORA (opcional)<br />
Preparación<br />
Por lo menos 15 minutos antes de usarla, prepare una solución que contenga (vol. / vol.): 60 % de etanol ; 10 % de ácido acético y 30 % de agua<br />
destilada o desionizada.<br />
Mézclela bien.<br />
Uso<br />
Para fijar las separaciones electroforéticas de hemoglobina en geles de agarosa.<br />
Almacenamiento, estabilidad y señales de deterioro<br />
Almacene la solución fijadora a temperatura ambiente cerrada herméticamente para evitar la evaporación. Deséchela después de 3 meses. No fije<br />
más de 4 geles por cada 150 mL de solución fijadora.<br />
EQUIPAMIENTO Y ACCESORIOS NECESARIOS PERO NO SUMINISTRADOS<br />
1. Fuente de alimentación: GD 61 D SEBIA, PN 1300 ; GD 251 D SEBIA, PN 1301 ; MG 300 SEBIA, PN 1302 ó MG 500 SEBIA, PN 1303.<br />
2. APLICADOR <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA, PN 1409, que contiene el soporte del aplicador <strong>HYDRAGEL</strong> <strong>K20</strong>.<br />
3. Cámara de Almacenaje Húmeda, PN 1270.<br />
4. Cubeta de electroforesis: <strong>K20</strong> SEBIA, PN 1400.<br />
5. Tanques y Soportes de Geles para el procesamiento de los geles: Kit de Accesorios <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA, PN 1420.<br />
6. Pipetas: 5 µL, 10 µL y 200 µL.<br />
7. Estufa-Secador: IS 80 SEBIA, PN 1430.<br />
8. Densitómetro / escáner de sobremesa capaz de escanear geles de 82 x 51 mm a 570 nm (filtro amarillo): HYRYS SEBIA, DVSE SEBIA o el<br />
programa PHORESIS para escáner de sobremesa. Consulte las instrucciones del fabricante para los procedimientos de funcionamiento y<br />
calibración.<br />
MUESTRAS PARA EL ANÁLISIS<br />
Extracción y almacenamiento de las muestras<br />
Se recomienda analizar muestras frescas de sangre no coagulada. Los anticoagulantes comunes, como los que contiene EDTA, citrato o heparina<br />
son aceptables ; no utilice los que contengan yodoacetato. La sangre debe obtenerse de acuerdo con los procedimientos establecidos de uso en el<br />
laboratorio clínico. Si es necesario, almacene las muestras entre 2 y 8 °C hasta 5 días.<br />
Preparación de las muestras<br />
• Agite el tubo primario antes de tomar el volumen de sangre total que se va a tratar.<br />
• Centrifugue la sangre no coagulada a 5.000 r.p.m. durante 5 minutos.<br />
• Deseche el plasma.<br />
• Lave los glóbulos rojos 2 veces con 10 volúmenes de salina ; tenga mucho cuidado al procesar volúmenes de glóbulos rojos inferiores a 10 µL.
- 39 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
• Elimine el exceso de solución salina que hay en la superficie del coágulo de glóbulos rojos lavados, y agítelo en el vórtex antes de pipetear los<br />
10 µL que se van a hemolizar.<br />
• Hemolice 10 µL de glóbulos rojos lavados con 130 µL de Solución Hemolizante.<br />
• Agite la mezcla en el vórtex durante 10 segundos e incube durante 5 minutos a temperatura ambiente.<br />
NOTAS:<br />
- Para preparar el hemolizado de sujetos levemente anémicos (aproximadamente 10 g/dL Hb) o gravemente anémicos (< 7 g/dL Hb), el<br />
volumen de glóbulos rojos lavados puede aumentarse hasta 15 µL y 20 µL, respectivamente. La intensidad de la tinción aumentará pero<br />
las concentraciones relativas de las fracciones individuales no cambiará.<br />
- El hemolizado no necesita ser filtrado o centrifugado.<br />
- La solución hemolizante de SEBIA no afecta a la inestable hemoglobina de Bart.<br />
PROCEDIMIENTO<br />
I. MIGRACIÓN<br />
1. Coloque el soporte del aplicador <strong>HYDRAGEL</strong> <strong>K20</strong> en una superficie plana (Fig. 1) y eleve la parte del soporte del aplicador con las muescas<br />
numeradas.<br />
2. Dispense 120 µL de agua destilada o desionizada en el tercio inferior del marco impreso en el soporte del aplicador <strong>HYDRAGEL</strong> <strong>K20</strong>.<br />
3. Saque el gel de agarosa <strong>HYDRAGEL</strong> de su envoltorio.<br />
4. Extienda un papel de filtro fino de manera rápida y uniforme sobre la superficie del gel para absorber el exceso de líquido. Retire el papel<br />
inmediatamente.<br />
ADVERTENCIA: Para evitar que se deshidrate, no deje que el papel de filtro contacte con el gel durante mucho tiempo.<br />
5. Ponga el gel (con el lado de agarosa hacia arriba) con su borde inferior contra el tope situado debajo del marco impreso (Fig. 2).<br />
6. Doble el gel y haga que contacte con el agua (Fig. 2). Asegúrese de que no se formen burbujas de aire, de que el agua esté extendida bajo<br />
toda la superficie del gel y de que éste esté alineado con el marco impreso.<br />
7. Baje el soporte del aplicador con las muescas numeradas hasta la posición intermedia con el interruptor en posición elevada.<br />
8. Coloque un aplicador en una superficie plana con los números de los pocillos hacia arriba (Fig. 3).<br />
9. Aplique 10 µL de muestra hemolizada en los pocillos del aplicador. Cargue cada aplicador en menos de 2 minutos. Use el aplicador sin<br />
demora. Para un uso posterior (hasta 8 horas después), ponga el aplicador en la cámara de almacenaje húmeda con los dientes hacia arriba<br />
[cójalo por el marco protector de plástico de los dientes], mantenga la cámara entera refrigerada y prepare el gel sobre el soporte del aplicador<br />
<strong>HYDRAGEL</strong> <strong>K20</strong> justo antes de usarlo.<br />
Consulte la hoja de instrucciones de la cámara húmeda para más detalles.<br />
10. Rompa el marco protector de los dientes del aplicador.<br />
11. Ponga el aplicador de muestra en la posición No. 4 del soporte del aplicador.<br />
IMPORTANTE: Los números impresos en el aplicador de muestra deben quedar de cara al operario (Fig. 4).<br />
12. Baje el soporte del aplicador con el interruptor de forma que el aplicador contacte con la superficie del gel. NO FUERCE LOS SOPORTES<br />
HACIA ABAJO.<br />
13. Después de 1 minuto, gire el interruptor para elevar el aplicador, saque el aplicador y deséchelo.<br />
14. Ponga el gel en una cubeta de electroforesis apropiada, de acuerdo con la polaridad indicada en el gel. Al usar la cubeta SEBIA <strong>K20</strong>, coloque<br />
el <strong>HYDRAGEL</strong> en el puente con el lado de agarosa hacia abajo ; el gel debe sumergirse en el tampón alrededor de 1 cm por cada lado.<br />
Consulte al hoja de instrucciones de la <strong>K20</strong> para más detalles.<br />
15. Conecte la cubeta a la fuente de alimentación.<br />
| CONDICIONES DE MIGRACIÓN | SEBIA <strong>K20</strong> |<br />
| Volumen de tampón por compartimento | 150 mL |<br />
| Volumen total de tampón | 300 mL |<br />
| Tiempo de migración | 15 minutos |<br />
| Voltaje constante | 165 V<br />
| |<br />
Corriente inicial (por gel) | 7 ± 2 mA |<br />
16. Después de la migración, desconecte la cubeta y saque el gel.<br />
II. FIJACIÓN<br />
Procese los geles utilizando uno de los procedimientos siguientes.<br />
Fijación con aire caliente (recomendada sólo con la Estufa-Secador SEBIA IS 80) :<br />
Seque el gel completamente en la estufa-secador a 80 °C (durante un mínimo de 10 minutos).<br />
Fijación con solución fijadora:<br />
1. Ponga el gel en un soporte de gel (suministrado con el Kit de Accesorios SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong>) para el procesamiento posterior.<br />
2. Llene un tanque (suministrado con el Kit de Accesorios SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong>) con 150 mL de solución fijadora.<br />
3. Sumerja el gel en la solución fijadora durante 15 minutos.<br />
4. Saque el gel y séquelo con una corriente de aire caliente a 80 °C en la estufa-secador IS 80.<br />
IMPORTANTE: El gel debe estar perfectamente seco.<br />
III. TINCIÓN - DECOLORACIÓN<br />
1. Sumerja el gel seco y enfriado en la solución de tinción durante 5 minutos.<br />
2. Decolore en tres baños sucesivos de solución decolorante hasta que la coloración de fondo sea completamente incolora y clara.<br />
3. Absorba el exceso de líquido de la superficie del gel con un pañuelo de papel y seque el gel con aire caliente a 80 °C. Si es necesario, limpie<br />
el reverso del gel seco (el lado de soporte de plástico) con un pañuelo de papel humedecido.
- 40 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
IV. LECTURA<br />
Escanee usando un densitómetro / escáner a 570 nm o con un filtro amarillo. Al usar los densitómetros HYRYS ó DVSE, coloque la fracción A 2 en la<br />
marca de 5 mm de la placa de lectura: el cero de lectura se realiza entre las fracciones de A 2 y de anhidrasa carbónica, en el punto más bajo.<br />
NOTA: Para asegurar que se obtienen los resultados más exactos y constantes posibles, haga lo siguiente:<br />
- Ajuste la longitud de lectura para incluir el patrón electroforético entero (≈ 30 mm).<br />
- Asegúrese de que los mínimos situados a ambos lados de la fracción A 2 están colocados en los pies del pico de A 2 .<br />
Es una buena práctica efectuar la lectura densitométrica de los geles teñidos sin demora. Para consultas futuras, se pueden guardar en una cubierta<br />
protectora en un lugar seco y oscuro, alejado de fuentes de calor y se pueden interpretar visualmente durante 3 meses por lo menos.<br />
RESULTADOS<br />
Control de Calidad<br />
Se aconseja incluir una sangre control valorada o una muestra de sangre valorada que contengan hemoglobinas A, F, C y S en cada análisis de<br />
muestras.<br />
Valores<br />
La lectura densitométrica de las separaciones electroforéticas teñidas proporciona las concentraciones relativas (porcentajes) de las fracciones<br />
individuales de hemoglobina.<br />
Los valores normales (media ± 2 SD) usando el procedimiento <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> han sido establecidos a partir de una población<br />
sana de 200 adultos (hombres y mujeres):<br />
Hemoglobina A ≥ 96.5 %<br />
Hemoglobina F < 2.0 % (*)<br />
Hemoglobina A2 ≤ 3.5 %<br />
(*) consulte Interferencias y Limitaciones<br />
Se recomienda que cada laboratorio establezca sus propios valores de normalidad.<br />
Interpretación<br />
1. Anomalías cualitativas: Hemoglobinopatías<br />
La mayoría de hemoglobinopatías son debidas a la sustitución por mutación de un solo aminoácido en uno de los cuatro tipos de cadenas<br />
polipeptídicas. La importancia clínica de un cambio así depende del tipo de aminoácido involucrado y de su posición. En enfermedades clínicamente<br />
significativas pueden estar afectadas las cadenas α o las ß (incluso las cadenas γ).<br />
Se han descrito más de 200 variantes de hemoglobina en adultos. Las primeras hemoglobinas anormales estudiadas y de aparición más frecuente<br />
tienen una carga eléctrica neta alterada, lo que facilita su detección mediante electroforesis.<br />
Hay cuatro hemoglobinas anormales principales que presentan un interés clínico particular: S, C, E y D.<br />
Los kits <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> están pensados para la identificación preliminar de las hemoglobinopatías y talasemias. Al observarse<br />
un patrón anormal, su identidad debería ser confirmada mediante las pruebas discriminatorias apropiadas (por ejemplo, electroforesis en geles de<br />
agarosa ácidos).<br />
Hemoglobina S<br />
La hemoglobina S es la más frecuente. Es debida a la sustitución de un ácido glutámico (un aminoácido ácido) de la cadena ß por una valina (un<br />
aminoácido neutro). Su movilidad electroforética se ve, por tanto, disminuida. En geles tamponados alcalinos, como el <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E)<br />
<strong>K20</strong>, la hemoglobina S migra entre las fracciones A y A 2 .<br />
Hemoglobina C<br />
Un ácido glutámico de la cadena ß está sustituido por una lisina (un aminoácido básico): su movilidad se ve fuertemente reducida. Con el<br />
procedimiento <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, C, E y A 2 están superpuestas. Cuando esta fracción es > 15 %, debe sospecharse la presencia<br />
de hemoglobinas C y E.<br />
Hemoglobina E<br />
Un ácido glutámico de la cadena ß está sustituido por una lisina: la hemoglobina E migra exactamente como la hemoglobina C usando el<br />
procedimiento <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>. A diferencia de la hemoglobina C, no se separa de la hemoglobina A en tampón ácido<br />
[<strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>]. Esta propiedad permite diferenciar E y C.<br />
Hemoglobina D<br />
Un ácido glutámico de la cadena ß está sustituido por una glutamina. Con el procedimiento <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> esta hemoglobina<br />
migra exactamente como la hemoglobina S. La hemoglobina D no se separa de la hemoglobina A en tampón ácido [<strong>HYDRAGEL</strong> ACID(E)<br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>] ; esta propiedad permite diferenciar S y D.<br />
2. Anomalías cuantitativas: Talasemias<br />
Las talasemias constituyen un grupo bastante heterogéneo de enfermedades genéticas caracterizadas por la disminución en la síntesis de uno o<br />
varios tipos de cadenas polipeptídicas. El mecanismo molecular de esta disminución no ha sido completamente descrito.<br />
Hay dos tipos de síndromes talasémicos:<br />
Talasemias Alfa<br />
Se caracterizan por la disminución en la síntesis de las cadenas α, lo que afecta a la síntesis de todas las hemoglobinas normales.<br />
El exceso de síntesis de cadenas ß y γ en relación con la de las cadenas α induce la formación de tetrámeros sin ninguna cadena α:<br />
• hemoglobina Bart = γ 4,<br />
• hemoglobina H = ß 4.
Beta-talasemias<br />
Se caracterizan por una disminución en la síntesis de las cadenas ß. Sólo se ve afectada la síntesis de la hemoglobina A.<br />
Por tanto, los porcentajes de hemoglobina F y hemoglobina A 2 están incrementados respecto a los de la hemoglobina A.<br />
3. Patrones de migración<br />
Migración de<br />
hemoglobinas normales<br />
A(A 0 + A 1 ) A (A 0 + A 1 )<br />
F<br />
S - D<br />
A2 A2 - C - E<br />
anhidrasa anhidrasa<br />
punto de aplicación<br />
A 0 : Fracción no glicada de la hemoglobina A normal del adulto.<br />
A 1 : Fracción glicada de la hemoglobina A normal del adulto.<br />
En los patrones de encima, el cátodo está abajo y el ánodo arriba.<br />
- 41 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Interferencias y Limitaciones<br />
• No use muestras de sangre hemolizadas.<br />
• Cuando se detecte una hemoglobina anormal que se comporte de forma diferente a como los hacen las variantes principales de la hemoglobina<br />
S, C, D y E, use otros métodos de identificación (por ejemplo, isoelectroenfoque, electroforesis de las cadenas de globina), o consulte o envíe la<br />
muestra a un laboratorio especializado.<br />
• La valoración densitométrica de la Hb F (o de cualquier otra hemoglobina minoritaria que migre en la proximidad de las fracciones principales) es<br />
semicuantitativa en la medida en que los valores se vuelven imprecisos por debajo de un 2 % - 3 % de la hemoglobina total.<br />
• Las muestras de ciertos pacientes con una hemoglobina S homocigota y tratados con Hydrea® (hydroxycarbamida) pueden presentar una<br />
hemoglobina F, cuya síntesis ha sido inducida por el tratamiento. En algunos casos se ha observado que esta hemoglobina F inducida tiene una<br />
movilidad, en los geles <strong>HYDRAGEL</strong> 7 <strong>HEMOGLOBIN</strong>(E), ligeramente diferente a la de la hemoglobina F nativa.<br />
• En algunas muestras que hayan sido conservadas más de 7 días, el rastro situado detrás de la fracción Hb A puede concentrarse, aunque esta<br />
fracción no debe confundirse con una variante de la hemoglobina, por ejemplo, las hemoglobinas H o Bart.<br />
Resolución de problemas<br />
Llame al Servicio de Atención Técnica de su distribuidor cuando la prueba no funcione pese a haber seguido cuidadosamente las instrucciones para<br />
la preparación y el almacenaje de los materiales, y para el procedimiento.<br />
Las hojas de seguridad de los diferentes reactivos del kit, así como las informaciones relativas a la eliminación de los desechos, están disponibles<br />
en el Servicio de Asistencia Técnica de su distribuidor.<br />
CARACTERÍSTICAS TÉCNICAS<br />
Migración de las hemoglobinas<br />
anormales principales<br />
Todos los datos de funcionamiento están basados en un estudio que incluía materiales e instrumentos SEBIA <strong>HYDRAGEL</strong>, comparándolos con un<br />
sistema comercial de geles de agarosa. Además, se hicieron estudios de concordancia en los que la identidad de las hemoglobinas y sus valores fueron<br />
establecidos mediante otros métodos reconocidos. Los resultados de ejemplos representativos de los estudios de funcionamiento se presentan aquí.<br />
Todas las separaciones electroforéticas se interpretaron visualmente. El densitómetro HYRYS de SEBIA se utilizó en todas las evaluaciones<br />
densitométricas para complementar los datos visuales.<br />
Reproducibilidad Intraanálisis (Intraserial)<br />
Tres muestras de sangre se sometieron a electroforesis usando el procedimiento <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> en geles del mimo lote. Cada<br />
muestra se analizó en todos los carriles de un único gel. La tabla siguiente muestra las medias, SD y CV de cada componente individual de la<br />
hemoglobina en las tres muestras, calculados a partir de los valores densitométricos en tanto por ciento de cada carril. Además, ninguna de las<br />
réplicas mostró valores falsos positivos o falsos negativos.<br />
| COMPONENTE | MEDIA | SD | CV (%) |<br />
| Sangre normal |<br />
| Hb A | 97.4 | 0.1 | 0.1 |<br />
| Hb A | 2 2.6 | 0.1 | 5.3 |<br />
| Hb A2 elevadas |<br />
| Hb A | 95.2 | 0.2 | 0.2 |<br />
| Hb A | 2 4.8 | 0.2 | 4.4 |<br />
| Hb C elevada |<br />
| Hb A | 56.7 | 0.4 | 0.8 |<br />
| Hb C | 43.3 | 0.4 | 1.0 |<br />
Reproducibilidad Interanálisis (Interserial)<br />
Se sometieron a electroforesis muestras de sangre usando el procedimiento <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> en geles de un único lote. Las<br />
muestras analizadas incluían siete muestras con una hemoglobina anormal (Hb S, Hb F ó Hb C), dos muestras con la Hb A 2 elevada y el resto eran<br />
muestras de sangre normales. Se calcularon las medias, SD y CV a partir de los datos obtenidos para cada componente en cada muestra. Los rangos<br />
de las medias, SD y CV, y el CV medio, que representa la suma de los componentes individuales, está tabulados debajo. Además, ninguna de las<br />
réplicas mostró valores falsos positivos o falsos negativos.
- 42 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
| COMPONENTE | MEDIA | SD | CV (%) | CV MEDIO (%) |<br />
| Hb A | 18.0 – 97.8 | 0.1 – 1.0 | 0.1 – 4.0 | 0.8 |<br />
| Hb F | 13.3 – 76.3 | 0.5 – 0.6 | 0.7 – 3.4 | 1.8 |<br />
| Hb C | 21.5 – 43.5 | 0.2 – 0.3 | 0.6 – 1.1 | 0.8 |<br />
| Hb S/D | 9.7 – 84.1 | 0.1 – 0.6 | 0.4 – 2.6 | 1.1<br />
| |<br />
Hb A | 2 2.2 – 5.7 | 0.1 – 0.2 | 2.3 – 7.6 | 4.0 |<br />
Exactitud – Detección de Anomalías de la Hemoglobina<br />
Se analizaron 63 muestras de sangre diferentes usando el procedimiento <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> y otro sistema comercial de geles de<br />
agarosa. Las muestras de sangre y su evaluación diagnóstica fueron proporcionados por un hospital. El diagnóstico estaba basado en una<br />
electroforesis de rutina en gel alcalino y en gel ácido y/o HPLC. Todas las hemoglobinas anormales o los niveles anormales de hemoglobinas<br />
normales detectados con el procedimiento <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> coincidieron con el sistema de geles comparado, los resultados del<br />
hospital y el diagnóstico clínico. No se observó ningún caso de falso positivo, esto es, la detección de una banda anormal o de un nivel anormal de<br />
una banda normal donde no existía tal anomalía.<br />
Exactitud – Determinación Cuantitativa de la Hb A 2<br />
Se midieron los niveles de Hb A 2 en 51 muestras de sangre con niveles normales y elevados de Hb A 2 , mediante densitometría de las separaciones<br />
electroforéticas obtenidas, usando el procedimiento <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>. Los valores medidos a partir de ambos procedimientos se<br />
analizaron mediante un procedimiento estadístico de regresión lineal. Los resultados del análisis de regresión lineal están tabulados debajo<br />
(y = <strong>HYDRAGEL</strong>).<br />
| Coeficiente de Correlación | Punto de corte en y | Pendiente | Rango de valores en % |<br />
| | | | (sistema SEBIA) |<br />
| 0.973 | -0.344 | 0.963 | 1.5 – 5.7 |<br />
BIBLIOGRAFÍA<br />
1. Fairbanks V.F., ed. (1980) Hemoglobinopathies and thalassemia: Laboratory methods and case studies. Brian C. Decker, New York.<br />
2. Galacteros F. (1986) Thalassémie, drépanocytose et autres hémoglobinopathies. Techniques et Biologie, 3, 174-178.<br />
3. Huisman T.H.J. and. Jonxis J.H.P (1977) The hemoglobinopathies: techniques of identification. Marcel Dekker, New York.<br />
4. Krauss J.S., Drew P.A., Jonah M.H., Trinh M., Shell S., Black L. and Baisden C.R. (1986) Densitometry and microchromatography compared for<br />
determination of the hemoglobin C and A 2 proportions in hemoglobin C and hemoglobin SC disease and in hemoglobin C trait. Clin. Chem. 32, 5,<br />
860-863.<br />
5. Livingstone C. (1986) The hemoglobinopathies. Edit. London.<br />
6. Maier-Redelsberger M., Girot R. (1989) Diagnostic biologique des maladies de l’hémoglobine. Feuillets de biologie, 170.<br />
7. Schneider R.G. (1978) Methods for detection of hemoglobin variants and hemoglobinopathies in the routine clinical laboratory. CRC Crit. Rev. Clin.<br />
Lab. Sci. 9, 243-271.<br />
8. Vovan L., Lara-Russo D., Orsini A. (1985) Diagnostic biologique des hémoglobinoses. Ann. Pédiat. 32, 9, 780-789.
UTILIZAÇÃO<br />
- 43 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
O <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> destina-se à separação das hemoglobinas normais (A e A 2 ) e à detecção das principais hemoglobinas<br />
anómalas: S ou D e C ou E, por electroforese em geles de agarose. A electroforese é feita no hemolisado da lavagem dos glóbulos vermelhos. As<br />
hemoglobinas são separadas em meio alcalino (pH 8,5), fixadas pelo calor ou em meio alcool/ácido e coradas com uma solução de negro de amido.<br />
O excesso de corante é eliminado com uma solução ácida. As electroforeses resultantes podem ser analisadas visualmente ou ser avaliadas por<br />
densitómetria, o que dá uma quantificação relativa e precisa das hemoglobinas com interesse particular, tais como a hemoglobina A 2 no diagnóstico<br />
da ß-talassémia. A electroforese em meio ácido como, por exemplo, o <strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, permite confirmar a identificação<br />
das variantes da hemoglobina, em especial para diferenciar a Hb S da Hb D e a Hb E da Hb C.<br />
Cada gel de agarose poderá analisar 7 amostras no kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>.<br />
Para diagnóstico in vitro. Registado no INFARMED.<br />
PRINCÍPIO DO TESTE<br />
A hemoglobina é uma molécula complexa composta por quatro cadeias polipeptídicas, idênticas duas a duas. Cada cadeia está ligada ao heme, um<br />
núcleo tetrapirrólico (porfirina), ligado a um átomo de ferro. A parte do heme é comum a todas as hemoglobinas e suas variantes. A parte proteica<br />
responsável pelo tipo de hemoglobina é dechamada globina. As cadeias polipeptídicas α, ß, δ e γ constituem as hemoglobinas humanas normais:<br />
• hemoglobina A ………………… = α 2 β 2<br />
• hemoglobina A 2 ……………… = α 2 δ 2<br />
• hemoglobina fetal F…………… = α 2 γ 2<br />
A cadeia α é comum a estas três hemoglobinas.<br />
A estrutura espacial da hemoglobina (como as de todas as proteínas) depende da natureza e da sequência dos aminoácidos que formam as cadeias.<br />
As ligações que se formam entre os diferentes amoinoácidos são responsáveis pela forma da molécula, pela estabilidade e suas propriedades. A<br />
substituição dos aminoácidos por mutação é responsável pela formação de variantes de hemoglobina, que têm diferentes cargas superficiais e,<br />
consequentemente, diferentes mobilidades electroforéticas, também dependentes do pH, da força iónica do tampão e da natureza do suporte.<br />
As anomalias das hemoglobinas são de dois tipos:<br />
• anomalias qualitativas (ou estruturais) resultantes são designadas por hemoglobinopatias ;<br />
• anomalias quantitativas (ou de regulação), provocadas por diminuição da síntese de uma das cadeias de hemoglobina, são designadas por<br />
talassémias.<br />
REAGENTES FORNECIDOS NOS KITS <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong><br />
| ITEM | REF. N° 3010 |<br />
| Geles de agarose (prontos a usar) | 10 geles |<br />
| Tampão Tris-Barbital (solução concentrada) | 3 frascos de 75 ml |<br />
| Diluente da solução corante (solução concentrada) | 1 frasco, 60 ml |<br />
| Negro de amido (solução concentrada) | 1 frasco, 20 ml |<br />
| Descorante (solução concentrada) | 1 frasco de 100 ml |<br />
| Solução hemolisante (pronto a usar) | 1 frasco, 20 ml |<br />
| Aplicadores 7 dentes (prontos a usar) | 1 caixa de 10<br />
|<br />
|<br />
Papéis de filtro finos | 1 pacote de 10 |<br />
PARA OPTIMIZAÇÃO DOS RESULTADOS<br />
Os elementos de um mesmo kit devem ser utilizados em conjunto, e de acordo com as instruções de utilização.<br />
LER ATENTAMENTE AS INSTRUÇÕES DE UTILIZAÇÃO.<br />
1. GELES DE AGAROSE<br />
Preparação<br />
Os geles de agarose estão prontos a usar. Cada gel contém: agarose, 8 g/l ; tampão alcalino pH 8,5 ± 0,1 ; aditivos, não perigosos nas concentrações<br />
usadas, necessários para optimizar o ensaio.<br />
Utilização<br />
Meio de suporte para a electroforese das hemoglobinas.<br />
Armazenamento, estabilidade e sinais de deterioração<br />
Armazenar os geles horizontalmente, na embalagem protectora de origem, à temperatura ambiente (15 - 30 °C) ou no frigorífico (2 - 8 °C). (A seta<br />
existente na parte da frente da caixa do kit deve estar voltada para cima). São estáveis até ao fim da validade indicada na caixa do kit e nos rótulos<br />
das embalagens dos geles. Evitar variações da temperatura durante o armazenamento (ex: não armazenar perto de uma janela ou de uma fonte de<br />
calor).<br />
NÃO CONGELAR!<br />
Deitar fora o gel quando:<br />
(i) houver cristais ou precipitados na superfície do gel ou quando a textura do mesmo for muito macia (isto sucede se o gel for congelado) ;<br />
(ii) há desenvolvimento de bactérias ou fungos ;<br />
(iii) estiver presente uma quantidade anormal de líquido na embalagem do gel (resultante da exsudação do gel devido a condições de<br />
armazenamento inadequadas).<br />
INSTRUÇÕES DE USO SEBIA - Português
- 44 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
2. TAMPÃO TRIS-BARBITAL<br />
Preparação<br />
Cada frasco de tampão concentrado deve ser completado a 1 litro com água destilada ou desmineralizada. Após diluição, a solução contém: tampão<br />
tris-barbital pH 9,2 ± 0,2 ; azida de sódio.<br />
ATENÇÃO: O tampão concentrado contém 2,45 % de barbital, 13,73 % de barbital sódico e 0,13 % de azida de sódio. Não ingerir! Se ingerida,<br />
consultar imediatamente um médico! Quando em contacto com ácidos, chumbo ou cobre a azida de sódio pode levar à formação de<br />
compostos explosivos ou tóxicos. Quando deitar fora lavar abundantemente com grandes quantidades de água.<br />
Utilização<br />
Tampão da electroforese.<br />
Armazenamento, estabilidade e sinais de deterioração<br />
Armazenar o tampão concentrado à temperatura ambiente ou no frigorífico. É estável por vários anos, pelo menos até ao fim da validade indicada<br />
na caixa do kit ou no rótulo do frasco. A solução diluída é estável por um ano, à temperatura ambiente, num frasco rolhado. Deitar fora se o seu<br />
aspecto se alterar ou se ficar turva devido a contaminação microbiana.<br />
3. DILUENTE DA SOLUÇÃO CORANTE<br />
Preparação<br />
O diluente da solução corante deverá ser utilizado como está descrito no parágrafo " SOLUÇÃO CORANTE NEGRO DE AMIDO ".<br />
Contém uma solução ácida.<br />
Utilização<br />
Para a preparação das soluções de corante negro de amido.<br />
Armazenamento, estabilidade e sinais de deterioração<br />
Armazenar o diluente à temperatura ambiente ou no frigorífico. É estável até ao fim da validade indicada na caixa do kit ou no rótulo do frasco. NÃO<br />
CONGELAR.<br />
Não adicionar azida de sódio.<br />
4. CORANTE NEGRO DE AMIDO<br />
Preparação<br />
O corante negro de amido concentrado, é uma solução viscosa que pode eventualmente gelificar, o que não afecta nada a qualidade da solução final<br />
e o seu poder de coloração.<br />
Em qualquer caso, para obter uma perfeita reconstituição do corante, é necessário que seja respeitado o procedimento seguinte:<br />
1. Adicionar cerca de 15 ml do diluente do corante ao frasco do negro de amido concentrado.<br />
2. Fechar cuidadosamente o frasco.<br />
3. Agitar muito vigorosamente o frasco durante pelo menos 5 segundos.<br />
4. Transferir esta solução para o recipiente de preparação da solução de coloração.<br />
5. Repetir esta etapa duas vezes ou se necessário 3 vezes.<br />
6. Transferir o diluente restante para o recipiente de preparação da solução de coloração.<br />
7. Completar o volume para 300 ml com água destilada ou desmineralizada.<br />
8. Agitar muito bem esta solução durante 5 a 10 minutos.<br />
A solução corante está pronta a utilizar.<br />
Após diluição, a solução de corante contém: solução ácida pH ≈ 2 ; negro de amido, 4 g/l ; etilenoglicol, 6,7% ; aditivos, não perigosos nas<br />
concentrações usadas, necessários para optimizar o ensaio.<br />
AVISO: Nocivo em caso de ingestão.<br />
Utilização<br />
Para corar geles depois da electroforese das proteínas.<br />
IMPORTANTE : A solução corante é unicamente destinada à coloração de 10 geles. Recomenda-se a renovação da solução após as 10 utilizações.<br />
Armazenamento, estabilidade e sinais de deterioração<br />
Armazenar a solução de corante concentrada e a solução diluída à temperatura ambiente ou no frigorífico em frascos fechados para evitar a<br />
evaporação.<br />
A solução concentrada é estável até ao fim da validade indicada na caixa do kit ou nos rótulos dos frascos.<br />
A solução diluída de corante é estável por um mês.<br />
Não guardar a solução de trabalho do corante próximo de uma fonte de calor.<br />
5. SOLUÇÃO DESCORANTE<br />
Preparação<br />
Cada frasco de solução descorante concentrada deve ser diluída a 1/1000 com água destilada ou desmineralizada e permite obter 100 litros de<br />
solução total. Diluir 1 ml da solução concentrada em 1 litro com água destilada ou desmineralizada. Após diluição, a solução descorante contém:<br />
ácido cítrico ; 0,5 g/l.<br />
Utilização<br />
Na descoloração, isto é, remoção do excesso de corante do gel.<br />
Armazenamento, estabilidade e sinais de deterioração<br />
Armazenar a solução descorante concentrada à temperatura ambiente ou no frigorífico. É estável até ao fim da validade indicada na caixa do kit ou<br />
no rótulo do frasco da solução descorante. A solução descorante diluída é estável por uma semana à temperatura ambiente, quando conservada em<br />
recipiente fechado.<br />
Deitar fora a solução diluída se se notarem alterações no seu aspecto, por exemplo, se se tornar turva devido a contaminação microbiana.<br />
Não adicionar azida de sódio.<br />
Em caso de conservação mais prolongada da solução diluída (superior a uma semana), adicionar 50 µl/l de ProClin 300 para evitar qualquer<br />
proliferação microbiana.<br />
A solução descorante diluída contendo ProClin é estável à temperatura ambiente (de 15 a 30 °C) ou no frigorífico (entre 2 e 8 °C). É estável até ao<br />
fim da validade indicada na caixa do kit ou no rótulo do frasco do descolorante.<br />
6. SOLUÇÃO HEMOLISANTE<br />
Preparação<br />
A solução hemolisante vem pronta a ser utilizada. Trata-se de um tampão com aditivos, não perigosos nas concentrações utilizadas, necessários para<br />
optimizar o ensaio.
- 45 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Utilização<br />
Para hemolisar os glóbulos vermelhos do sangue.<br />
Armazenamento, estabilidade e sinais de deterioração<br />
Armazenar a solução hemolisante à temperatura ambiente ou no frigorífico. É estável até ao fim da validade indicada na caixa do kit ou no rótulo do<br />
frasco da solução hemolisante.<br />
Deitar fora a solução hemolisante se o seu aspecto se alterar, isto é, se ficar turva devido a contaminação microbiana.<br />
7. APLICADORES<br />
Utilização<br />
Aplicadores pré-cortados, de utilização única, para aplicação das amostras.<br />
Armazenamento<br />
Armazenar os aplicadores em local seco à temperatura ambiente ou no frigorífico.<br />
8. PAPEIS DE FILTRO FINOS<br />
Utilização<br />
Pré-cortados, de utilização única, estes finos papéis absorventes destinam-se à absorção do excesso de líquido da superfície do gel antes da<br />
aplicação da amostra.<br />
Armazenamento<br />
Armazenar os papéis de filtro finos num local seco à temperatura ambiente ou no frigorífico.<br />
REAGENTES NECESSÁRIOS MAS NÃO FORNECIDOS<br />
1. SORO FISIOLÓGICO<br />
Preparação<br />
Preparar uma solução a 0,15 M (9 g/l) de NaCl em água destilada ou desmineralizada.<br />
Utilização<br />
Para lavar os glóbulos vermelhos.<br />
Armazenamento, estabilidade e sinais de deterioração<br />
Armazenar à temperatura ambiente ou no frigorífico. Deitar fora após 3 meses ou se notar alterações no seu aspecto, por exemplo, se se tornar turva<br />
devido a contaminação microbiana. Para conservar por períodos de tempo mais alargado, adicionar azida de sódio (1 g/l).<br />
2. FIXADOR (facultativo)<br />
Preparação<br />
Pelo menos 15 minutos antes da utilização, preparar o fixador (v/v): 60 % de etanol ; 10 % de ácido acético ; 30 % de água destilada ou<br />
desmineralizada. Misturar bem.<br />
Utilização<br />
Fixação das proteínas separadas por electroforese em geles de agarose.<br />
Armazenamento, estabilidade e sinais de deterioração<br />
Armazenar à temperatura ambiente em frasco bem rolhado para evitar a evaporação. Deitar fora passados 3 meses. Não fixar mais que 4 geles em<br />
cada 150 ml de fixador.<br />
EQUIPAMENTO E ACESSÓRIOS NECESSÁRIOS MAS NÃO FORNECIDOS<br />
1. Fonte de alimentação, ex: GD 61 D SEBIA, ref. n° 1300 ; GD 251 D SEBIA, ref. n° 1301 ; MG 300 SEBIA, ref. n° 1302 ou MG 500 SEBIA,<br />
ref. n° 1303.<br />
2. APPLICATEUR <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA, ref. n° 1409, que contém o suporte-aplicador <strong>HYDRAGEL</strong> <strong>K20</strong>.<br />
3. Câmara húmida, ref. n° 1270.<br />
4. Câmara de electroforese: <strong>K20</strong> SEBIA, ref. n° 1400.<br />
5. Tinas e suportes para o tratamento de geles de 7 amostras: kit de acessórios <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA ref. n° 1420.<br />
6. Pipetas: 5 µl, 10 µl e 200 µl.<br />
7. Incubador-secador: IS 80 SEBIA, ref. n° 1430.<br />
8. Densitómetro/scanner capaz de ler geles de 82 x 51 mm a 570 nm (filtro amarelo): HYRYS SEBIA, DVSE SEBIA ou scanner equipado com logiciel<br />
PHORESIS SEBIA. Seguir as instruções de cada aparelho na sua utilização e calibração.<br />
AMOSTRAS A ANALIZAR<br />
Colheita e conservação das amostras<br />
É recomendada a utilização de amostras de sangue frescas colhidas com anticoagulante. Podem ser usados tubos de colheita contendo como<br />
anticoagulante EDTA, citratos ou heparina ; evitar os que contenham iodoacetato. O sangue deve ser colhido de acordo com os métodos utilizados<br />
nos laboratórios de análises clínicas. Se necessário, armazenar o sangue entre 2 - 8 °C até cinco dias.<br />
Preparação das amostras<br />
• Homogeneize o tubo de colheita antes de retirar o sangue total a preparar.<br />
• Centrifugar o sangue com anticoagulante a 5000 rpm durante 5 minutos.<br />
• Deitar fora o plasma.<br />
• Lavar as glóbulos vermelhos 2 vezes com 10 volumes de soro fisiológico: deve ser tomado o maior cuidado quando se estiver a manipular volumes<br />
de glóbulos vermelhos inferiores a 10 µl.
- 46 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
• Elimine o excesso de solução salina que se encontra como sobrenadante dos glóbulos vermelhos e agite-os no vórtex antes de extrair 10 µL para<br />
hemólise.<br />
• Hemolisar 10 µl de glóbulos vermelhos com 130 µl de solução hemolisante.<br />
• Agitar no vortex durante 10 segundos e incubar 5 minutos à temperatura ambiente.<br />
NOTAS:<br />
- Para preparar um hemolisado de indivíduos anémicos o volume de glóbulos vermelhos (obtidos após centrifugação), pode ser aumentado :<br />
- 15 µl para indivíduos levemente anémicos (aproximadamente 0,1 g/ml de Hb)<br />
- 20 µl para indivíduos muito anémicos (< 0,07 g/ml de Hb), e 130 µl de solução hemolisante.<br />
Como consequência, a intensidade da coloração vai aumentar sem modificar a proporção de cada fracção.<br />
- Não é necessário filtrar ou centrifugar o hemolisado.<br />
- A solução hemolisante SEBIA não afecta a hemoglobina instável de Bart.<br />
TÉCNICA<br />
I. MIGRAÇÃO<br />
1. Colocar o suporte-aplicador <strong>HYDRAGEL</strong> <strong>K20</strong> sobre a bancada (Fig. 1) e erguer a parte móvel do mesmo (suporte dos aplicadores).<br />
2. Colocar 120 µl de água destilada ou desmineralizada no terço inferior do quadro impresso no suporte-aplicador.<br />
3. Retirar o gel da embalagem.<br />
4. Eliminar rapidamente o excesso de líquido da superfície do gel com a ajuda de um papel de filtro fino.<br />
ATENÇÃO: Não deixar o papel de filtro em contacto prolongado com o gel, para evitar a sua desidratação.<br />
5. Colocar o gel virado para cima, contra a parte inferior do quadro impresso no suporte-aplicador (Fig. 2).<br />
6. Dar uma forma côncava ao gel (Fig. 2) e baixá-lo lentamente até contacto com a gota de água. A gota deve repartir-se por toda a largura do<br />
gel. Ajustar ligeiramente o gel de modo a eliminar as bolhas de ar que se tenham formado. Baixar o gel até ficar na horizontal. A gota de água<br />
deve-se repartir sobre toda a superfície do gel.<br />
7. Baixar o suporte dos aplicadores até uma posição intermédia, com o botão, situado lateralmente, voltado para cima.<br />
8. Colocar um aplicador numa superfície plana, com os números dos poços virados para cima.<br />
9. Aplicar 10 µl de amostra hemolisada em cada poço. A pipetagem das amostras não deve ultrapassar os 2 minutos.<br />
O aplicador deve ser utilizado imediatamente após a colocação das amostras.<br />
Para uma utilização posterior (8 horas no máximo), colocar o aplicador na câmara húmida com os dentes voltados para cima (segure-o pela<br />
protecção de plástico), pôr a câmara húmida no frigorífico e só colocar o gel no suporte-aplicador <strong>HYDRAGEL</strong> <strong>K20</strong> no momento da sua<br />
utilização.<br />
Ver as instruções de utilização da câmara húmida para mais detalhes.<br />
10. Quebrar e retirar a protecção dos dentes.<br />
11. Colocar o aplicador na posição n° 4 do suporte-aplicador.<br />
IMPORTANTE: Os números impressos no aplicador devem ficar virados para o operador (Fig. 4).<br />
12. Baixar o suporte do aplicador rodando o botão lateral de modo a que o aplicador fique em contacto com o gel. NÃO FORÇAR A DESCIDA<br />
DO SUPORTE DOS APLICADORES.<br />
13. Após 1 minuto de aplicação, rodar o botão lateral para levantar o aplicador. Retirar o aplicador e deitar fora.<br />
14. Colocar o gel na câmara de electroforese, segundo a polaridade indicada no gel,com as amostras no lado do cátodo.<br />
Posicionar o <strong>HYDRAGEL</strong> no suporte da tina <strong>K20</strong> com o lado do gel voltado para baixo ; o gel deve mergulhar cerca de 1cm no tampão, de<br />
cada lado.<br />
Ver instruções da câmara <strong>K20</strong> para mais pormenores.<br />
15. Ligar a tina à fonte de alimentação.<br />
| CONDIÇÕES DE MIGRAÇÃO | SEBIA <strong>K20</strong> |<br />
| Volume de tampão por compartimento | 150 mL |<br />
| Volume total de tampão | 300 mL |<br />
| Tempo de migração | 15 minutes |<br />
| Voltagem constante | 165 V<br />
|<br />
|<br />
Corrente inicial (por gel) | 7 ± 2 mA |<br />
16. Após migração, desligar a tina e retirar o gel.<br />
II. FIXAÇÃO DAS PROTEÍNAS<br />
Pode-se fazer de duas maneiras : fixação pelo calor ou com solução de fixação.<br />
Fixação pelo calor (só com o incubador-secador IS 80 SEBIA) :<br />
Secar o gel sob ar quente a 80 °C no incubador-secador IS 80 até secagem completa (durante 10 minutes mínimo).<br />
Fixação com solução de fixação:<br />
1. Colocar o gel num suporte para geles (fornecido com o kit de acessórios SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong>).<br />
2. Encher uma tina (fornecida com o kit de acessórios SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong>) com 150 ml de solução de fixação.<br />
3. Imergir o gel verticalmente no fixador durante 15 minutos.<br />
4. Retirar o gel e secá-lo sob ar quente a 80 °C no incubador-secador IS 80.<br />
IMPORTANTE : O gel deve estar perfeitamente seco.
- 47 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
III. COLORAÇÃO-DESCOLORAÇÃO<br />
1. Imergir o gel, frio e seco, na solução corante durante 5 minutos.<br />
2. Proceder à remoção do excesso de corante em três banhos sucessivos de descorante, até que o fundo surja limpo e incolor.<br />
3. Retirar o excesso de líquido da superfície do gel com um papel macio e secar o gel sob ar quente a 80 °C. Se necessário, limpar a parte de<br />
trás do gel (suporte plástico) com um papel macio humedecido.<br />
IV. LEITURA<br />
Ler com um densitómetro / scanner a 570 nm ou com filtro amarelo.<br />
Se utilizar os densitómetros HYRYS ou DVSE, posicione a fracção A 2 na marca de 5 mm da placa de leitura, de modo a colocar o zero no ponto mais<br />
baixo entre a fracção A 2 e a fracção anidrase carbónica.<br />
NOTA: Para garantir resultados mais precisos e coerentes :<br />
- Regular o comprimento de leitura a 30 mm, de forma a incluir todo o perfil electroforético.<br />
- Posicionar as mínimas de modo a rodearem o valor da fracção A 2 .<br />
Recomenda-se analisar os perfis electroforéticos o mais rapidamente possível. Os geles, conservados no escuro, em ambiente seco e ao abrigo de<br />
todas as fontes de calor, podem ser interpretados qualitativamente num período de 3 meses.<br />
RESULTADOS<br />
Controlo de qualidade<br />
É aconselhável incluir uma amostra de sangue de controlo contendo as hemoglobinas A, F, C e S, em cada série de amostras.<br />
Valores<br />
A leitura a 570 nm por densitómetria permite definir as concentrações relativas (percentagens) de cada fracção.<br />
Os valores normais (médios mais 2 DP), para cada fracção, nos geles <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> foram estabelecidos a partir de uma<br />
população saudável de 200 adultos (homens e mulheres):<br />
Hemoglobina A ≥ 96,5 %<br />
Hemoglobina F < 2,0 % (*)<br />
Hemoglobina A2 ≤ 3,5 %<br />
(*) Ver Interferências e Limitações<br />
Recomenda-se que cada laboratório estabeleça os seus próprios valores normais.<br />
Interpretação<br />
1. Anomalias qualitativas: hemoglobinopatias<br />
A maioria das hemoglobinopatias deve-se à substituição por mutação de um único aminoácido num dos quatro tipos de cadeias polipeptídicas. O<br />
significado clínico de tal alteração depende do tipo de aminoácido e do local envolvidos. Em doenças clinicamente significativas, a cadeia α ou a cadeia<br />
ß estão afectadas.<br />
Foram descritas mais de 200 variantes de hemoglobina no adulto. As primeiras hemoglobinas anómalas estudadas e as que ocorrem mais frequentemente<br />
têm a sua carga eléctrica alterada, o que leva a uma fácil detecção por electroforese.<br />
Existem quatro hemoglobinas anómalas principais que apresentam um interesse clínico particular, do ponto de vista antropológico e médico: S, C, E e D.<br />
O kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> destina-se à detecção das hemoglobinopatias e talassémias. Uma vez detectado um perfil electroforético<br />
anómalo, este deve ser confirmado por electroforese em meio ácido, em geles de agarose.<br />
Hemoglobina S<br />
A hemoglobina S é a mais frequente. Deve-se à substituição de um ácido glutâmico da cadeia ß (um aminoácido ácido) por uma valina (aminoácido<br />
neutro): a sua mobilidade electroforética vai diminuir. Nos geles <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> em meio alcalino, a hemoglobina S migra em<br />
posição central, entre as fracções A e A 2 .<br />
Hemoglobina C<br />
Um ácido glutâmico da cadeia ß é substituído por uma lisina (aminoácido básico): a sua mobilidade vai diminuir muito. No <strong>HYDRAGEL</strong><br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> as fracções C e E ficam sobrepostas à fracção A 2 . Quando esta fracção é superior a 15 %, deve-se suspeitar das<br />
hemoglobinas C e E.<br />
Hemoglobina E<br />
Um ácido glutâmico da cadeia ß é substituído por uma lisina: a hemoglobina E migra exactamente como a hemoglobina C no <strong>HYDRAGEL</strong><br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>. Ao contrário do que sucede com a hemoglobina C, não se separa das hemoglobinas A e A 2 em meio ácido [<strong>HYDRAGEL</strong><br />
ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>]. Esta propriedade permite diferenciar as hemoglobinas E e C.<br />
Hemoglobina D<br />
Um ácido glutâmico da cadeia ß é substituído por uma glutamina. No <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> esta hemoglobina migra exactamente como<br />
a hemoglobina S. Ao contrário da hemoglobina S, a hemoglobina D não se separa das hemoglobinas A e A 2 em meio ácido [<strong>HYDRAGEL</strong> ACID(E)<br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>] ; esta propriedade permite diferenciar as hemoglobinas S e D.<br />
2. Anomalias quantitativas: Talassémias<br />
As talassémias constituem um grupo bastante heterogéneo de distúrbios genéticos, caracterizadas por uma diminuição da síntese de um dos tipos<br />
de cadeias polipeptídicas. O mecanismo molecular desta diminuição ainda está mal conhecido.<br />
Existem dois tipos de síndromes talassémicos:
- 48 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Alfa-talassémias<br />
Caracterizam - se pela diminuição da síntese das cadeias α, afectando consequentemente a síntese das 3 hemoglobinas fisiológicas. O excesso de<br />
síntese das cadeias ß e γ em relação às cadeias a leva à formação de tetrâmeros sem cadeia α:<br />
• Hemoglobina Bart = γ 4<br />
• hemoglobina H = ß 4<br />
Beta-talassémias<br />
Caracterizam-se pela diminuição da síntese de cadeias ß. Apenas a síntese da hemoglobina A é afectada. As percentagens de hemoglobina F e A 2<br />
aumentam em relação à da hemoglobina A.<br />
3. Perfis electroforéticos<br />
Migração das<br />
hemoglobinas normais<br />
A(A 0 + A 1 ) A (A 0 + A 1 )<br />
F<br />
S - D<br />
A 2<br />
A2 - C - E<br />
anidrase carbónica anidrase carbónica<br />
ponto de aplicação<br />
A0: fracção não glicosilada da hemoglobina A normal do adulto.<br />
A1: fracção glicosilada da hemoglobina A normal do adulto.<br />
Interferências e limitações<br />
• Não usar amostras de sangue hemolisadas.<br />
• Quando uma hemoglobina anómala é detectada, apresentando uma mobilidade electroforética diferente da das principais variantes de<br />
hemoglobinas S, C, D e E, deve-se utilizar outros meios de identificação (ex: electroforese das cadeias de globinas), ou consultar um laboratório<br />
especializado.<br />
• O doseamento da hemoglobina Fetal (Hb F), ou de qualquer outra hemoglobina menor que migra na proximidade de fracções principais, é<br />
aproximado quando a sua concentração representa menos de 2 a 3 % da hemoglobina total.<br />
• As amostras de certos doentes apresentam uma hemoglobina S homozigótica ; quando tratadas com Hydrea® (hidroxicarbamida) podem<br />
apresentar uma hemoglobina F, cuja síntese foi induzida por este tratamento. Em alguns dos casos observados, esta hemoglobina F induzida<br />
apresentou uma mobilidade nos geles <strong>HYDRAGEL</strong> 7 <strong>HEMOGLOBIN</strong>(E) ligeiramente diferente da apresentada pela hemoglobina F fisiológica.<br />
• Nas amostras armazenadas há mais de 7 dias, pode observar-se uma banda concentrada em frente à fracção Hb A. Esta banda concentrada não<br />
deverá ser confundida e interpretada como uma variante da hemoglobina (por exemplo, Hemoglobinas H ou Bart).<br />
Assistência técnica<br />
Em caso de maus resultados contactar os serviços técnicos do fornecedor.<br />
Estão disponíveis nos Serviços Técnicos da SEBIA fichas de dados de segurança dos diversos reagentes do kit, bem como informação relativa à<br />
eliminação dos desperdícios.<br />
CARACTERÍSTICAS DO ENSAIO<br />
Migração das principais<br />
hemoglobinas anómalas<br />
Todas as leituras densitométricas foram efectuadas com o densitómetro HYRYS da SEBIA. Os perfis electroforéticos foram interpretados a olho nú.<br />
Os resultados obtidos por análise quantitativa indicam uma boa repetibilidade e reproductibilidade da técnica <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> em<br />
relação a todos os aspectos testados, com um coeficiente de variação médio de 2,2 %.<br />
Reprodutibilidade intra-ensaio<br />
Três amostras de sangue (uma normal, uma com valores elevados de Hb A2 e uma amostra com Hb C) foram analisadas repetidamente em geles<br />
de um mesmo lote <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>. Os perfis electroforéticos foram analisados por densitómetria e a tabela seguinte apresenta<br />
os valores médios (em %), DP e CV, obtidos para cada fracção de hemoglobina de cada uma das 3 amostras.<br />
NOTA: Os resultados foram concordantes para todas as amostras:<br />
- Amostras com valores normais de Hb A2 apresentaram todos os valores normais.<br />
- Amostras com valores elevados de Hb C e Hb A2 apresentaram todos os valores elevados.<br />
| FRACÇÃO DE Hb | MÉDIA | DP | CV (%) |<br />
| Sangue normal |<br />
| Hb A | 97,4 | 0,1 | 0,1 |<br />
| Hb A | 2 2,6 | 0,1 | 5,3 |<br />
| Sangue com Hb A2 elevado |<br />
| Hb A | 95,2 | 0,2 | 0,2 |<br />
| Hb A | 2 4,8 | 0,2 | 4,4 |<br />
| Sangue com Hb C elevado |<br />
| Hb A | 56,7 | 0,4 | 0,8<br />
|<br />
|<br />
Hb C | 43,3 | 0,4 | 1,0 |<br />
Reprodutibilidade inter-ensaio<br />
Foram analisadas amostras de sangue, em 10 geles <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> de um mesmo lote. As amostras ensaiadas incluíam<br />
7 amostras com uma hemoglobina anormal (Hb S, Hb F ou Hb C) e 2 amostras com um nível elevado de Hb A 2 . Os valores médios (em %), DP e CV<br />
foram calculados para cada fracção de hemoglobina das amostras. Os limites dos valores médios, DP e CV, e a média dos CV representando o<br />
conjunto de cada fracção, estão indicados na tabela abaixo.
NOTA: Os resultados foram concordantes para todas as amostras:<br />
- Amostras com valores normais de Hb A2 apresentaram todos os valores normais.<br />
- Amostras com valores elevados de Hb A2 apresentaram todos os valores elevados.<br />
- 49 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
| FRACÇÃO Hb | MÉDIA | DP | CV (%) | MÉDIA CV (%) |<br />
| Hb A | 18,0 – 97,8 | 0,1 – 1,0 | 0,1 – 4,0 | 0,8 |<br />
| Hb F | 13,3 – 76,3 | 0,5 – 0,6 | 0,7 – 3,4 | 1,8 |<br />
| Hb C/E | 21,5 – 43,5 | 0,2 – 0,3 | 0,6 – 1,1 | 0,8 |<br />
| Hb S/D | 9,7 – 84,1 | 0,1 – 0,6 | 0,4 – 2,6 | 1,1<br />
| |<br />
Hb A | 2 2,2 – 5,7 | 0,1 – 0,2 | 2,3 – 7,6 | 4,0 |<br />
Precisão - Detecção das anomalias da hemoglobina<br />
Foram analisadas 63 amostras de sangue com o kit <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> e com outro sistema em gel de agarose disponível<br />
comercialmente. As amostras de sangue e o respectivo diagnóstico clinico, estabelecido por electroforese em geles alcalino e ácido e/ou HPLC, foram<br />
fornecidas por um hospital.<br />
Os resultados obtidos mostraram uma correlação perfeita entre os dois sistemas com, para a detecção de hemoglobinas normais, uma sensibilidade<br />
de 100 % e uma especificidade de 100 % em relação à técnica de referência, calculados segundo o método recomendado (Wendling, 1986).<br />
Todas as hemoglobinas anómalas, assim como hemoglobinas as normais, detectadas com o <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> estavam de acordo<br />
com o sistema de geles comparativo, com os resultados do hospital e com o diagnóstico clínico. Não foram observados casos de falsos positivos,<br />
isto é, detecção de fracções anómalas quando não existia a anomalia inerente. Também não se observaram casos de falsos positivos (detecção de<br />
uma Hb anómala inexistente ou de uma Hb de valor normal detectada numa taxa anormal).<br />
Precisão - Determinação quantitativa de Hb A 2<br />
51 amostras de sangue, com níveis normais e elevados de Hb A 2 , foram analisadas em paralelo por densitómetria dos perfis electroforéticos, obtidos<br />
em geles <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, e com outro gel disponível comercialmente.<br />
A correlação entre as duas técnicas foi analisada por regressão linear e outros métodos estatísticos (média e coeficiente de regressão linear). Os<br />
parâmetros de correlação entre os 2 sistemas de análise (y = <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>) estão apresentados no quadro seguinte:<br />
| COEFICIENTE DE CORRELAÇÃO | INTERSECÇÃO EM Y | DECLIVE | GAMA DE VALORES % |<br />
| | | | (sistema SEBIA) |<br />
| 0,973 | -0,344 | 0,963 | 1,5 – 5,7 |<br />
BIBLIOGRAFIA<br />
1. Fairbanks V.F., ed. (1980) Hemoglobinopathies and thalassemia: Laboratory methods and case studies. Brian C. Decker, New York.<br />
2. Galacteros F. (1986) Thalassémie, drépanocytose et autres hémoglobinopathies. Techniques et Biologie, 3, 174-178.<br />
3. Huisman T.H.J. and. Jonxis J.H.P (1977) The hemoglobinopathies: techniques of identification. Marcel Dekker, New York.<br />
4. Krauss J.S., Drew P.A., Jonah M.H., Trinh M., Shell S., Black L. and Baisden C.R. (1986) Densitometry and microchromatography compared for<br />
determination of the hemoglobin C and A 2 proportions in hemoglobin C and hemoglobin SC disease and in hemoglobin C trait. Clin. Chem. 32, 5,<br />
860-863.<br />
5. Livingstone C. (1986) The hemoglobinopathies. Edit. London.<br />
6. Maier-Redelsberger M., Girot R. (1989) Diagnostic biologique des maladies de l’hémoglobine. Feuillets de biologie, 170.<br />
7. Schneider R.G. (1978) Methods for detection of hemoglobin variants and hemoglobinopathies in the routine clinical laboratory. CRC Crit. Rev. Clin.<br />
Lab. Sci. 9, 243-271.<br />
8. Vovan L., Lara-Russo D., Orsini A. (1985) Diagnostic biologique des hémoglobinoses. Ann. Pédiat. 32, 9, 780-789.<br />
9. Wendling A. Procédures de diagnostic ou de dépistage : Justification et validité d’un test de diagnostic ou de dépistage-sensibilité-spécificité.<br />
Impact-Internat, 1986 ; Sept : 93-97.
ΠΡΒΛΕΠΜΕΝΗ ΡΗΣΗ<br />
- 50 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Τo κιτ <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> είναι σεδιασµένo για τ διαωρισµ των υσιλγικών αιµσαιρινών (A και A 2 ) και για την<br />
ανίνευση των κύριων παραλλαγών της αιµσαιρίνης: S ή D και C ή E και της εµρυϊκής αιµσαιρίνης F, µε ηλεκτρρηση σε αλκαλική<br />
γέλη αγαρης. Τα πρκύπτντα ηλεκτρρήµατα αιλγύνται πτικά. Η πυκνµέτρηση πρσέρει σετική πστικπίηση των<br />
επιµέρυς ωνών. Θα πρέπει να ακλυθήσει ηλεκτρρηση σε ιν gel π.. <strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> για την<br />
επιεαίωση της ταυτπίησης τυ τύπυ της αιµσαιρίνης, ειδικά για τη διαρπίηση της αιµσαιρίνης S απ την D και της E απ<br />
την C.<br />
Κάθε gel αγαρης στ κιτ <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> πρρίεται για την ανάλυση 7 δειγµάτων.<br />
Για In Vitro διαγνωστική ρήση.<br />
ΑΡΗ ΤΗΣ ∆ΚΙΜΑΣΙΑΣ<br />
Η αιµσαιρίνη είναι ένα σύµπλκ µρι απτελύµεν απ δύ εύγη πλυπεπτιδικών αλυσίδων. Κάθε αλυσίδα συνδέεται µε την αίµη,<br />
έναν τετραπυρρλικ πυρήνα (πρυρίνη) πυ συνδέεται ηλικά µε ένα άτµ σιδήρυ. Τ µρι αίµης είναι κιν για λες τις<br />
αιµσαιρίνες και τις πικιλίες τυς. τύπς της αιµσαιρίνης πρσδιρίεται απ τ πρωτεϊνικ τµήµα πυ νµάεται σαιρίνη. ι<br />
πλυπεπτιδικές αλυσίδες, α, , γ και δ συγκρτύν τις υσιλγικές ανθρώπινες αιµσαιρίνες:<br />
• αιµσαιρίνη A ............................................................= α 2 2<br />
• αιµσαιρίνη A 2 ...........................................................= α 2 δ 2<br />
• εµρυϊκή αιµσαιρίνη F...........................................= α 2 γ 2<br />
Η αλυσίδα α είναι κινή στις τρεις αυτές αιµσαιρίνες.<br />
Η τρισδιάστατη δµή της αιµσαιρίνης και ι άλλες µριακές της ιδιτητες (πως λων των πρωτεϊνών) εαρτώνται απ τη ύση και την<br />
ακλυθία των αµινέων πυ συγκρτύν τις αλυσίδες. Η αντικατάσταση αµινέων µε µετάλλαη είναι υπεύθυνη για τ σηµατισµ<br />
µρίων αιµσαιρίνης µε διαρετικ επιανειακ ρτί και συνεπώς διαρετική ηλεκτρρητική κινητικτητα, η πία επίσης<br />
εαρτάται απ τ pH και την ιντική ισύ τυ ρυθµιστικύ διαλύµατς. Σε ιν pH, η κινητικτητα επηρεάεται επίσης απ την<br />
ηλεκτρστατική αλληλεπίδραση µεταύ των θετικά ρτισµένων µρίων αιµσαιρίνης και των αρνητικά ρτισµένων µάδων στ άγαρ.<br />
ι πρκύπτυσες πιτικές (ή δµικές) ανωµαλίες νµάνται αιµσαιρινπάθειες. Η µειωµένη σύνθεση κάπιας απ τις αλυσίδες της<br />
αιµσαιρίνης δηγεί σε πστικές ανωµαλίες, πυ νµάνται θαλασσαιµίες.<br />
Η ανάλυση πραγµατπιείται σε αιµλυµα απ πλυµένα ερυθρκύτταρα. ι αιµσαιρίνες διαωρίνται µε ηλεκτρρηση σε αλκαλικά<br />
gel και τα κλάσµατα γίννται ρατά µε ρώση µε amidoblack. Τα στεγνωµένα gel είναι έτιµα για ερµηνεία.<br />
ΑΝΤΙ∆ΡΑΣΤΗΡΙΑ ΚΑΙ ΥΛΙΚΑ ΠΑΡΕΜΕΝΑ ΜΕ Τ ΚΙΤ <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong><br />
| ΕΙ∆Σ |<br />
| PN 3010 |<br />
Gel αγαρης (έτιµα πρς ρήση) |<br />
| 10 gel |<br />
Ρυθµιστικ διάλυµα Tris-Barbital (πυκν διάλυµα) |<br />
| 3 ιαλίδια των 75 mL |<br />
Μέσ αραίωσης διαλύµατς ρώσης (πυκν διάλυµα) |<br />
| 1 ιαλίδι, 60 mL |<br />
ρωστική amidoblack (πυκν διάλυµα) |<br />
| 1 ιαλίδι, 20 mL |<br />
∆ιάλυµα απρωµατισµύ (πυκν διάλυµα) |<br />
| 1 ιαλίδι, 100 mL |<br />
Αιµλυτικ διάλυµα (έτιµ πρς ρήση) |<br />
| 1 ιαλίδι, 20 mL |<br />
Εαρµγείς (7 δντια) (έτιµι πρς ρήση) | ∆ιηθητικά αρτιά<br />
|<br />
1 συσκ. των 10<br />
1 συσκ. των 10<br />
|<br />
ΓΙΑ ΑΡΙΣΤΑ ΑΠΤΕΛΕΣΜΑΤΑ<br />
λα τα αντιδραστήρια απ ίδι κιτ πρέπει να ρησιµπιύνται πάντα µαί και σύµωνα µε τις δηγίες ρήσης.<br />
ΠΑΡΑΚΑΛΥΜΕ ∆ΙΑΒΑΣΤΕ ΠΡΣΕΚΤΙΚΑ Τ ΦΥΛΛ ∆ΗΓΙΩΝ.<br />
1. GEL ΑΓΑΡΗΣ<br />
Πρετιµασία<br />
Τα gel αγαρης είναι έτιµα πρς ρήση. Κάθε gel περιέει: αγαρη, 0.8 g/dL, αλκαλικ ρυθµιστικ διάλυµα pH 8.5 ± 0.1, πρσθετα, µη<br />
επιλαή στις ρησιµπιύµενες συγκεντρώσεις, αναγκαία για άριστη απδση.<br />
ρήση<br />
Μέσ για ηλεκτρρηση αιµσαιρίνης.<br />
Φύλαη, σταθερτητα και σηµεία αλλίωσης<br />
Φυλάσσετε τα gel ριντια εντς της συσκευασίας τυς σε θερµκρασία δωµατίυ (15 έως 30 °C) ή στη συντήρηση (2 έως 8 °C). (Τ έλς<br />
στην πρσθια επιάνεια τυ κυτιύ τυ κιτ πρέπει να δείνει πρς τα άνω). Απύγετε την απθήκευση κντά σε παράθυρ ή σε πηγή<br />
θερµτητας. Απύγετε τις µεγάλες διακυµάνσεις θερµκρασίας κατά τη ύλαη. Τα gel είναι σταθερά µέρι την ηµερµηνία λήης πυ<br />
αναγράεται στη συσκευασία τυ κιτ ή των gel.<br />
ΜΗΝ ΚΑΤΑΨΥΕΤΕ.<br />
Πετάτε τα gel ταν:<br />
(i) σηµατιστύν κρύσταλλι ή ίηµα στην επιάνεια τυ gel ή αν η υή τυ gel γίνει πλύ µαλακή (λα αυτά πρκύπτυν αν τ gel<br />
καταψυθεί),<br />
(ii) αναπτυθύν ακτήρια ή µύλα,<br />
(iii) υπάρει µεγαλύτερη απ τ υσιλγικ πστητα στ κυτί τυ gel (απτέλεσµα της είδρωσης τυ ρυθµιστικύ διαλύµατς απ τ<br />
gel λγω ακατάλληλων συνθηκών ύλαης).<br />
∆ΗΓΙΕΣ SEBIA - Ελληνικά
- 51 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
2. ΡΥΘΜΙΣΤΙΚ ∆ΙΑΛΥΜΑ TRIS-BARBITAL<br />
Πρετιµασία<br />
Κάθε ιαλίδι τυ πυκνύ διαλύµατς αραιώνεται µε έως 1 λίτρ απεσταγµένυ ή απινισµένυ ύδατς.<br />
Μετά την αραίωση, τ διάλυµα εργασίας περιέει : tris-barbital pH 9.2 ± 0.3, αίδι τυ νατρίυ.<br />
ΠΡΕΙ∆ΠΙΗΣΗ: Τ ρυθµιστικ διάλυµα στις ταινίες περιέει 2.45 % αριτάλη, 13.73 % νατριύ αριτάλη και 0.13 % αίδι τυ<br />
νατρίυ. Μην τ καταπίνετε! Αν τ καταπιείτε, συµυλευτείτε αµέσως ιατρ ! ταν τ πετάτε απύγετε επαή µε έα, µλυδ ή<br />
αλκ, καθώς µπρεί να σηµατιστύν εκρηκτικές ή τικές ενώσεις µε τ αίδι τυ νατρίυ.<br />
ρήση<br />
Ρυθµιστικ διάλυµα για ηλεκτρρηση.<br />
Φύλαη, σταθερτητα και σηµεία αλλίωσης<br />
Φυλάσσετε τ διάλυµα πρ της αραίωσης σε θερµκρασία δωµατίυ ή στ ψυγεί. Τ πυκν διάλυµα είναι σταθερ για αρκετά ρνια και<br />
τυλάιστν µέρι την ηµερµηνία λήης η πία σηµειώνεται στις ετικέττες της συσκευασίας τυ κιτ και των ιαλιδίων τυ διαλύµατς.<br />
Τ αραιωµέν διάλυµα είναι σταθερ για ένα έτς σε θερµκρασία δωµατίυ σε κλειστ δεί.<br />
Πετάτε τ αραιωµέν διάλυµα αν µεταληθεί η ψη τυ, π.. θλωση λγω µικριακής επιµλυνσης.<br />
3. ΜΕΣ ΑΡΑΙΩΣΗΣ ∆ΙΑΛΥΜΑΤΣ ΡΩΣΗΣ<br />
Πρετιµασία<br />
Τ πυκν µέσ αραίωσης διαλύµατς ρωστικής πρέπει να ρησιµπιείται πως περιγράεται στην παράγρα “ΡΩΣΤΙΚΗ<br />
AMIDOBLACK“.<br />
Περιέει ιν διάλυµα.<br />
ρήση<br />
Για την παρασκευή τυ διαλύµατς ρωστικής amidoblack.<br />
Φύλαη, σταθερτητα και σηµεία αλλίωσης<br />
Φυλάσσετε τ πυκν µέσ αραίωσης διαλύµατς ρωστικής σε θερµκρασία δωµατίυ ή στψυγεί. Είναι σταθερ µέρι την ηµερµηνία<br />
λήης η πία σηµειώνεται στις ετικέττες της συσκευασίας τυ κιτ και των ιαλιδίων. ΜΗΝ ΚΑΤΑΨΥΕΤΕ.<br />
Μην πρσθέτετε αίδι τυ νατρίυ.<br />
4. ΡΩΣΤΙΚΗ AMIDOBLACK<br />
Πρετιµασία<br />
Η πυκνή ρωστική amidoblack είναι ένα ιώδες διάλυµα τ πί ενδέεται να µετατραπεί σε γέλη. Η καταλληλτητα τυ πυκνύ<br />
διαλύµατς ρωστικής δεν επηρεάεται απ την αύηση της γλιτητάς τυ ή τη στερεπίησή τυ.<br />
Σε λες τις περιπτώσεις, για να επιτύετε τέλεια ανασύσταση της ρωστικής, σας συνιστύµε να ακλυθήσετε την εής διαδικασία :<br />
1. Πρσθέστε 15 mL τυ µέσυ αραίωσης ρωστικής στ ιαλίδι τυ πυκνύ διαλύµατς.<br />
2. Κλείστε πρσεκτικά τ ιαλίδι.<br />
3. Ανακινήστε έντνα τ ιαλίδι για περίπυ 5 δευτερλεπτα.<br />
4. Αδειάστε αυτ τ διάλυµα στ δεί πυ πρρίεται για την επεεργασία τυ διαλύµατς ρωστικής.<br />
5. Επαναλάετε αυτ τ ήµα δύ ρές, ή τρεις αν ρειάεται.<br />
6. Αδειάστε τ υπλιπ µέσ αραίωσης στ δεί και συµπληρώστε µε απεσταγµέν ή απινισµέν ύδωρ έως γκυ 300 mL.<br />
7. Ανακινήστε καλά τα περιεµενα τυ δείυ για 5 - 10 λεπτά.<br />
Τ διάλυµα ρωστικής είναι έτιµ πρς ρήση.<br />
Μετά την αραίωση, τ διάλυµα εργασίας της ρωστικής περιέει: ιν διάλυµα pH ≈ 2, amidoblack, 0.4 g/dL, αιθυλενγλυκλη, 6.7 %,<br />
πρσθετα, µη επιλαή στις ρησιµπιύµενες συγκεντρώσεις, αναγκαία για άριστη απδση.<br />
ΠΡΕΙ∆ΠΙΗΣΗ: Επιλαές αν καταπθεί.<br />
ρήση<br />
Για τη ρώση των gel µετά απ ηλεκτρρητικ διαωρισµ πρωτεϊνών.<br />
ΣΗΜΑΝΤΙΚ: Τ διάλυµα ρωστικής είναι σεδιασµέν για ρώση µν 10 gel. Αλλάτε τ διάλυµα µετά απ 10 διαδικασίες ρώσης.<br />
Φύλαη, σταθερτητα και σηµεία αλλίωσης<br />
Φυλάσσετε τα διαλύµατα πρ και µετά την αραίωση σε θερµκρασία δωµατίυ ή στ ψυγεί σε κλειστύς περιέκτες για να απτραπεί η<br />
εάτµιση. Τ πυκν διάλυµα ρωστικής είναι σταθερ µέρι την ηµερµηνία λήης η πία σηµειώνεται στις ετικέττες της συσκευασίας<br />
τυ κιτ και των ιαλιδίων.<br />
Τ διάλυµα εργασίας είναι σταθερ για 1 µήνα.<br />
Μην απθηκεύετε τ διάλυµα ρώσης κντά σε πηγή θερµτητας.<br />
5. ∆ΙΑΛΥΜΑ ΑΠΡΩΜΑΤΙΣΜΥ<br />
Πρετιµασία<br />
Κάθε ιαλίδι ∆ιαλύµατς Απρωµατισµύ αραιώνεται µε έως 100 λίτρα απεσταγµένυ ύδατς. Είναι ευερές να αραιώνεται µν 1 mL<br />
τυ διαλύµατς σε 1 λίτρ. Μετά την αραίωση τ διάλυµα απρωµατισµύ περιέει: κιτρικ ύ 0.05 g/dL.<br />
ρήση<br />
Για απρωµατισµ, δηλαδή ααίρεση της περίσσειας ρωστικής απ τη γέλη.<br />
Για καθαρισµ τυ τµήµατς ρώσης.<br />
Φύλαη, σταθερτητα και σηµεία αλλίωσης<br />
Φυλάσσετε τ διάλυµα πρ της αραίωσης σε θερµκρασία δωµατίυ ή στ ψυγεί. Τ πυκν διάλυµα είναι σταθερ µέρι την ηµερµηνία<br />
λήης η πία σηµειώνεται στις ετικέττες της συσκευασίας τυ κιτ και των ιαλιδίων τυ διαλύµατς.Τ αραιωµέν διάλυµα είναι σταθερ<br />
για µια εδµάδα σε θερµκρασία δωµατίυ σε κλειστ δεί.<br />
Μην πρσθέτετε αίδι τυ νατρίυ.<br />
Πετάτε τ διάλυµα αν µεταληθεί η ψη τυ, π.. θλωση λγω µικριακής επιµλυνσης.<br />
Για να απτρέψετε πλλαπλασιασµ µικρίων στ αραιωµέν διάλυµα απρωµατισµύ αν πρκειται να τ υλάετε για περισστερ<br />
απ µια εδµάδα, πρσθέστε 5 µL/dL ProClin 300.<br />
Τ διάλυµα εργασίας στ πί έει πρστεθεί ProClin είναι σταθερ σε κλειστ δεί σε θερµκρασία δωµατίυ ή στ ψυγεί µέρι την<br />
ηµερµηνία λήης η πία σηµειώνεται στις ετικέττες της συσκευασίας τυ κιτ και των ιαλιδίων.<br />
6. ΑΙΜΛΥΤΙΚ ∆ΙΑΛΥΜΑ<br />
Πρετιµασία<br />
Τ αιµλυτικ διάλυµα είναι έτιµ πρς ρήση. Είναι ένα ρυθµιστικ διάλυµα µε πρσθετα, µη επιλαή στις ρησιµπιύµενες<br />
συγκεντρώσεις, απαραίτητα για άριστη απδση.
- 52 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
ρήση<br />
Για την αιµλυση των ερυθρκυττάρων.<br />
Φύλαη, σταθερτητα και σηµεία αλλίωσης<br />
Φυλάσσετε τ αιµλυτικ διάλυµα σε θερµκρασία δωµατίυ (15 έως 30 °C) ή στη συντήρηση (2 έως 8 °C). Παραµένει σταθερ µέρι την<br />
ηµερµηνία λήης η πία σηµειώνεται στις ετικέττες της συσκευασίας τυ κιτ και της συσκευασίας τυ διαλύµατς.<br />
Πετάτε τ αιµλυτικ διάλυµα αν µεταληθεί η ψη τυ, π.. θλωση λγω µικριακής επιµλυνσης.<br />
7. ΕΦΑΡΜΓΕΙΣ<br />
ρήση<br />
Έτιµι, εαρµγείς µιας ρήσης για τπθέτηση των δειγµάτων.<br />
Φύλαη<br />
Φυλάσσετε τυς εαρµγείς σε ηρ µέρς σε θερµκρασία δωµατίυ ή στ ψυγεί.<br />
8. ∆ΙΗΘΗΤΙΚΑ ΑΡΤΙΑ - ΛΕΠΤΑ<br />
ρήση<br />
Μιας ρήσης απρρητικά αρτιά για στύπωµα της υγρασίας απ την επιάνεια τυ gel πριν την τπθέτηση των δειγµάτων.<br />
Απθήκευση<br />
Τα λεπτά διηθητικά αρτιά απθηκεύνται σε στεγν µέρς, σε θερµκρασία δωµατίυ ή σε ψύη.<br />
ΑΝΤΙ∆ΡΑΣΤΗΡΙΑ ΑΠΑΡΑΙΤΗΤΑ ΑΛΛΑ ΜΗ ΠΑΡΕΜΕΝΑ<br />
1. ΛΩΡΙΝΑΤΡΙΥ ∆ΙΑΛΥΜΑ<br />
Πρετιµασία<br />
Πρετιµάστε διάλυµα 0.15 M (0.9 g/dL) NaCl σε απεσταγµέν ή απινισµέν ύδωρ.<br />
ρήση<br />
Για την έκπλυνση ερυθρκυττάρων και αραίωση των αιµλυµάτων.<br />
Φύλαη, σταθερτητα και σηµεία αλλίωσης<br />
Φυλάσσεται σε θερµκρασία δωµατίυ ή στ ψυγεί. Πετάτε τ διάλυµα µετά 3 µήνες ή αν µεταληθεί η ψη τυ, π.. θλωση λγω<br />
µικριακής επιµλυνσης. Για µεγαλύτερη περίδ διατήρησης πρσθέστε αίδι τυ νατρίυ, 0.1 g/dL.<br />
2. ∆ΙΑΛΥΜΑ ΜΝΙΜΠΙΗΣΗΣ (πραιρετικ)<br />
Πρετιµασία<br />
Τυλάιστν 15 min πριν τη ρήση, παρασκευάστε διάλυµα µε (vol. / vol.): 60 % αιθανλη, 10 % ικ ύ και 30 % απεσταγµέν ή<br />
απινισµέν ύδωρ.<br />
Αναµίτε καλά.<br />
ρήση<br />
Για τη µνιµπίηση ηλεκτρρηµάτων αιµσαιρίνης σε gel.<br />
Φύλαη, σταθερτητα και σηµεία αλλίωσης<br />
Φυλάσσεται σε θερµκρασία δωµατίυ καλά κλεισµέν για να απύγετε την εάτµιση. Πετάτε τ µετά απ 3 µήνες. Μην µνιµπιείτε<br />
περισστερα απ 4 gel σε κάθε 150 mL µνιµπιητικύ διαλύµατς.<br />
ΕΠΛΙΣΜΣ ΚΑΙ ΣΥΜΠΛΗΡΩΜΑΤΙΚΑ ΕΑΡΤΗΜΑΤΑ ΑΠΑΡΑΙΤΗΤΑ ΑΛΛΑ ΜΗ ΠΑΡΕΜΕΝΑ<br />
1. Τρδτικ ρεύµατς: GD 61 D SEBIA, PN 1300, GD 251 D SEBIA, PN 1301, MG 300 SEBIA, PN 1302 ή MG 500 SEBIA, PN 1303.<br />
2. ΕΦΑΡΜΓΕΑΣ <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA, PN 1409, µε τ ρέα τυ εαρµγέα <strong>HYDRAGEL</strong> <strong>K20</strong>.<br />
3. Θάλαµς Υγρής Φύλαης, PN 1270.<br />
4. Θάλαµς ηλεκτρρησης: <strong>K20</strong> SEBIA, PN 1400.<br />
5. ∆εαµενές και στατήρες gel για την επεεργασία πλακών gel : Κιτ συµπληρωµατικών εαρτηµάτων <strong>HYDRAGEL</strong> <strong>K20</strong> SEBIA, PN 1420.<br />
6. Πιπέττες: 5 µL, 10 µL και 200 µL.<br />
7. Κλίανς επώασης - στεγνώµατς: IS 80 SEBIA, PN 1430.<br />
8. Πυκνµετρ / σαρωτής µε δυναττητα σάρωσης gel 82 x 51 mm στα 570 nm (κίτριν ίλτρ) : λγισµικ HYRYS SEBIA, DVSE SEBIA ή<br />
PHORESIS για σαρωτή flat-bed. Ανατρέτε στις δηγίες ρήσης και αθµνµησης τυ κατασκευαστή.<br />
∆ΕΙΓΜΑΤΑ ΠΡΣ ΑΝΑΛΥΣΗ<br />
Λήψη και διατήρηση δειγµάτων<br />
Συνιστάται να ρησιµπιύνται δείγµατα ρέσκυ αίµατς µε αντιπηκτικ. Τα κινά αντιπηκτικά πως EDTA, κιτρικ ή ηπαρίνη είναι<br />
απδεκτά. Απύγετε εκείνα πυ περιέυν ιωδεικ ύ. Τ αίµα πρέπει να συλλέγεται σύµωνα µε τις καθιερωµένες διαδικασίες<br />
κλινικής εργαστηριακής πρακτική. Αν ρειάεται, διατηρήστε τα δείγµατα στυς 2 ως 8 °C για έως 5 ηµέρες.<br />
Πρετιµασία των δειγµάτων<br />
• Ανακινήστε τ σωλήνα συλλγής πριν τη µεταρά τυ αίµατς για πρετιµασία.<br />
• Φυγκεντρήστε αίµα µε αντιπηκτικ στις 5 000 rpm για 5 min.<br />
• Πετάτε τ πλάσµα.<br />
• Πλύνετε τα ερυθρκύτταρα 2 ρές µε 10 γκυς υσιλγικύ ρύ. Ιδιαίτερη ρντίδα ρειάεται ταν επεεργάεστε γκυς<br />
ερυθρκυττάρων µικρτερυς των 10 µL.<br />
• Απρρίψτε την περίσσεια τυ διαλύµατς υσιλγικύ ρρύ πάνω απ τ σαιρίδι των ερυθρών αιµσαιρίων και ανακινήστε τα,<br />
πριν απ την λήψη 10 µL για αιµλυση.<br />
• Αιµλύστε 10 µL συµπυκνωµένων ερυθρών µε 130 µL αιµλυτικύ διαλύµατς.<br />
• Περιδινήστε στ vortex για 10 sec και επωάστε για 5 min σε θερµκρασία δωµατίυ.
- 53 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
ΣΗΜΕΙΩΣΕΙΣ:<br />
- Για να ετιµάσετε αιµλυµα απ άτµα, ελαρά αναιµικά (περίπυ 10 g/dL Hb) ή αριά αναιµικά (< 7 g/dL Hb), γκς των<br />
συµπυκνωµένων ερυθρών µπρεί να αυηθεί στα 15 µL και 20 µL αντίστια. Η ένταση της ρώσης θα αυηθεί έτσι αλλά ι<br />
σετικές συγκεντρώσεις των επιµέρυς κλασµάτων δεν θα αλλάυν.<br />
- Τ αιµλυµα δεν ρειάεται διήθηση ή υγκέντρηση.<br />
- Τ αιµλυτικ διάλυµα της SEBIA δεν επηρεάει την ασταθή αιµσαιρίνη Bart’s.<br />
∆ΙΑ∆ΙΚΑΣΙΑ<br />
I. ΣΤΑ∆Ι ΗΛΕΚΤΡΦΡΗΣΗΣ<br />
1. Τπθετήστε τν ρέα τυ εαρµγέα <strong>HYDRAGEL</strong> <strong>K20</strong> σε επίπεδη επιάνεια (Εικ. 1) και σηκώστε τ τµήµα τυ ρέα µε τις<br />
αριθµηµένες εγκπές.<br />
2. Εισαγάγετε 120 µL απεσταγµέν ή απινισµέν ύδωρ µέρι τ κατώτερ τρίτ της κλίµακας πυ είναι τυπωµένη στ ρέα<br />
<strong>HYDRAGEL</strong> <strong>K20</strong>.<br />
3. Ανίτε τη συσκευασία τυ <strong>HYDRAGEL</strong>.<br />
4. Περάστε γρήγρα και µιµρα ένα διηθητικ αρτί στην επιάνεια τυ gel για να απρρήσει την περίσσεια υγρύ.<br />
Ααιρέστε τ αρτί αµέσως.<br />
ΠΡΕΙ∆ΠΙΗΣΗ: Μην αήνετε τ διηθητικ αρτί σε επαή µε τ gel επί µακρν για να µην αυδατωθεί.<br />
5. Τπθετήστε την πλακέτα τυ gel (µε την επιάνεια τυ gel πρς τα άνω) µε τ άκρ της να αγγίει τ stop στ κάτω τµήµα της<br />
τυπωµένης κλίµακας (Εικ. 2).<br />
6. Λυγίστε τ gel και αµηλώστε τ επί της επιάνειας τυ νερύ (Εικ. 3). Βεαιωθείτε τι δεν έυν παγιδευτεί υσαλίδες αέρα, τι<br />
τ νερ έει απλωθεί κάτω απ λκληρη την πλακέτα τυ gel και τ gel είναι ευθυγραµµισµέν µε την τυπωµένη κλίµακα.<br />
7. Κατεάστε τ ρέα στην ενδιάµεση θέση µε τ διακπτη στην υψηλή θέση.<br />
8. Τπθετήστε έναν εαρµγέα σε µια επίπεδη επιάνεια µε τυς αριθµύς των θρίων στη δειά πλευρά (Εικ. 3).<br />
9. Τπθετήστε 10 µL απ τα αιµλυµένα δείγµατα στα θρία τυ εαρµγέα. Φρτώστε τν εαρµγέα εντς 2 min.<br />
- ρησιµπιήστε τν εαρµγέα αµέσως.<br />
- Για ύστερη ρήση (ως 8 ώρες), τπθετήστε τν εαρµγέα στ θάλαµ υγρής ύλαης µε τα δντια πρς τα άνω (κρατήστε τν<br />
απ τ πλαστικ πρστατευτικ κάλυµµα των δντιών), διατηρήστε λ τν θάλαµ στ ψυγεί και τπθετήστε τ gel στ<br />
ρέα <strong>HYDRAGEL</strong> <strong>K20</strong> λίγ πριν τη ρήση.<br />
Βλέπε τ ύλλ δηγιών τυ θαλάµυ υγρής ύλαης για περισστερες λεπτµέρειες.<br />
10. Απσπάστε τ πρστατευτικ κάλυµµα των δντιών τυ εαρµγέα.<br />
11. Τπθετήστε τν εαρµγέα στη θέση No 4 τυ ρέα.<br />
ΣΗΜΑΝΤΙΚ: ι τυπωµένι αριθµί στν εαρµγέα πρέπει να είναι στραµµένι πρς τν ειριστή (Εικ. 4)<br />
12. αµηλώστε τ ρέα τυ εαρµγέα µε τ διακπτη έτσι ώστε να έρθει εαρµγέας σε επαή µε την επιάνεια τυ gel. ΜΗΝ<br />
ΠΙΕΕΤΕ ΤΥΣ ΦΡΕΙΣ ΤΕΛΕΙΩΣ ΠΡΣ ΤΑ ΚΑΤΩ.<br />
13. Μετά απ 1 min, γυρίστε τ διακπτη για να σηκώσετε τν εαρµγέα, ααιρέστε και πετάτε τν εαρµγέα.<br />
14. Τπθετήστε τ gel σε κατάλληλ θάλαµ ηλεκτρρησης, σύµωνα µε την πλικτητά τυ, µε την κατώτερη πλευρά τυ gel πρ<br />
ταν ρησιµπιείτε τ θάλαµ SEBIA <strong>K20</strong>, τπθετήστε τ <strong>HYDRAGEL</strong> στη γέυρα µε την πλευρά τυ gel πρς τα κάτω. Τ gel<br />
πρέπει να υθίεται περίπυ 1 cm στ διάλυµα σε κάθε πλευρά.<br />
Βλέπε τ ύλλ δηγιών τυ θαλάµυ <strong>K20</strong> για περαιτέρω λεπτµέρειες.<br />
15. Συνδέστε τ θάλαµ µε την παρή ρεύµατς.<br />
|<br />
Συνθήκες ηλεκτρρησης | SEBIA <strong>K20</strong> |<br />
γκς ρυθµιστικύ διαλύµατς ανά τµήµα |<br />
| 150 mL |<br />
λικς γκς ρυθµιστικύ διαλύµατς |<br />
ρνς ηλεκτρρησης<br />
Σταθερή τάση<br />
Αρικ ρεύµα (ανά gel)<br />
|<br />
300 mL<br />
15 min<br />
165 V<br />
7 ± 2 mA<br />
|<br />
16. Μετά την ηλεκτρρηση, απσυνδέστε τ θάλαµ απ τ τρδτικ και ααιρέστε τ gel.<br />
II. ΜΝΙΜΠΙΗΣΗ<br />
Υπάλετε τα gel σε µια απ τις ακλυθες επεεργασίες.<br />
Μνιµπίηση µε θερµ αέρα (συστήνεται µν µε τν Κλίαν επώασης-στεγνώµατς SEBIA IS 80) :<br />
Στεγνώστε τ gel τελείως στν κλίαν στυς 80 °C (για 10 min τυλάιστν).<br />
Μνιµπίηση µε διάλυµα µνιµπίησης :<br />
1. Τπθετήστε τ gel σε στατήρα (παρέεται µε τ Κιτ συµπληρωµατικών εαρτηµάτων SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong>).<br />
2. Γεµίστε µια δεαµενή (παρέεται µε τ Κιτ συµπληρωµατικών εαρτηµάτων SEBIA <strong>HYDRAGEL</strong> <strong>K20</strong>) µε 150 mL διαλύµατς<br />
µνιµπίησης.<br />
3. Βυθίστε τ gel στ διάλυµα µνιµπίησης για 15 min.<br />
4. Ααιρέστε τ gel και στεγνώστε τ µε θερµ 80 °C ρεύµα αέρα στν Κλίαν επώασης-στεγνώµατς IS 80.<br />
ΣΗΜΑΝΤΙΚ : Τ gel πρέπει να είναι τελείως στεγν.<br />
III. ΡΩΣΗ - ΑΠΡΩΜΑΤΙΣΜΣ<br />
1. Βυθίστε τ στεγν και ψυρ gel στ διάλυµα ρώσης για 5 min.<br />
2. Απρωµατίστε µε τρία διαδικά λυτρά σε διάλυµα απρωµατισµύ µέρι τ background να γίνει τελείως άρωµ και διαυγές.<br />
3. Σκυπίστε τ υπεράλλν υγρ απ την επιάνεια τυ gel µε απρρητικ αρτί και στεγνώστε τ gel µε θερµ αέρα 80 °C. Αν<br />
ρειαστεί, καθαρίστε την πίσω (πλαστική) επιάνεια τυ στεγνύ ιλµ µε υγρ απρρητικ αρτί.
- 54 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
IV. ΣΑΡΩΣΗ<br />
Σαρώστε µε πυκνµετρ / σαρωτή στα 570 nm ή µε κίτριν ίλτρ. ταν ρησιµπιείτε πυκνµετρα HYRYS ή DVSE, τπθετήστε τ<br />
κλάσµα A2 στ σηµεί των 5 mm της πλάκας σάρωσης: τ σηµεί µηδενισµύ τπθετείται ανάµεσα στ κλάσµα A2 και της καρνικής<br />
ανυδράσης στ κατώτερ σηµεί.<br />
ΣΗΜΕΙΩΣΗ: Για να εασαλίσετε πι ακριή και σταθερά απτελέσµατα:<br />
- Πρσαρµστε τ µήκς σάρωσης ώστε να περιλάετε λ τ ηλεκτρρητικ ίνς (≈ 30 mm).<br />
- Βεαιωθείτε τι ι περιριστές στις δύ πλευρές τυ κλάσµατς A2 είναι τπθετηµένι στις ρίες της αιµής A2 .<br />
Καλ είναι να διαάετε τα ρωµατισµένα gel ωρίς καθυστέρηση. Για µελλντική αναρά, µπρύν να διατηρηθύν σε πρστατευτικ<br />
κάλυµµα σε µέρς ηρ και σκτειν, µακριά απ πηγές θερµτητας.<br />
ΑΠΤΕΛΕΣΜΑΤΑ<br />
Πιτικς έλεγς<br />
Συνιστάται να περιλαµάνεται ένα δείγµα ελέγυ περιέν αιµσαιρίνες A, F, C και S σε κάθε σειρά δειγµάτων.<br />
Τιµές<br />
Η πυκνµετρική σάρωση κερωσµένων ηλεκτρρηµάτων παρέει σετικές συγκεντρώσεις (πσστά) των επιµέρυς ωνών της<br />
αιµσαιρίνης.<br />
ι υσιλγικές τιµές (µ.. ± 2 SD) στα gel ΗYDRAGEL 7 <strong>HEMOGLOBIN</strong>(E) έυν εαθεί απ ένα υγιή πληθυσµ 200 ενηλίκων (ανδρών<br />
και γυναικών):<br />
Αιµσαιρίνη A ≥ 96.5 %<br />
Αιµσαιρίνη F < 2.0 % (*)<br />
Αιµσαιρίνη A2 ≤ 3.5 %<br />
(*) λ. Παρεµλές και Περιρισµί<br />
Συνιστάται κάθε εργαστήρι να διαµρώνει τις δικές τυ υσιλγικές τιµές.<br />
Ερµηνεία<br />
1. Πιτικές διαταραές: Αιµσαιρινπάθειες<br />
ι περισστερες αιµσαιρινπάθειες είλνται σε µετάλλαη αντικατάστασης ενς αµινές σε µια απ τις πλυπεπτιδικές αλυσίδες.<br />
Η κλινική σηµασία µιας τέτιας αλλαγής εαρτάται απ τν τύπ τυ αµινές και τη θέση. Σε κλινικά σηµαντική νσ, επηρεάεται είτε<br />
η α αλυσίδα είτε η .<br />
Περισστερες απ 200 πικιλίες αιµσαιρίνης ενηλίκυ έυν περιγραεί. ι πρώτες πυ µελετήθηκαν και ι συντερα απαντώµενες<br />
έυν αλλαγµέν καθαρ ηλεκτρικ ρτί, µε απτέλεσµα την εύκλη ανίνευσή τυς µε ηλεκτρρηση.<br />
Υπάρυν τέσσερις κύριες παθλγικές αιµσαιρίνες ι πίες παρυσιάυν ειδικ κλινικ ενδιαέρν: S, C, E και D.<br />
Τα κιτ <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> πρρίνται για την πρκαταρκτική ταυτπίηση αιµσαιρινπαθειών και θαλασσαιµιών. ταν<br />
διαπιστωθεί παθλγικ ηλεκτρρητικ πρίλ, θα πρέπει να διερευνάται µε κατάλληλες δκιµασίες (π.. ηλεκτρρηση σε ινη<br />
γέλη αγαρης).<br />
Αιµσαιρίνη S<br />
Η αιµσαιρίνη S είναι η συντερη. είλεται σε αντικατάσταση ενς γλυταµικύ ές (ένα ιν αµινύ) στη ß-αλυσίδα απ αλίνη<br />
(ένα υδέτερ αµινύ). Η ηλεκτρρητική της κινητικτητα είναι επµένως µειωµένη. Στ αλκαλικ <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>,<br />
η αιµσαιρίνη S κινείται µεταύ των κλασµάτων A και A 2 .<br />
Αιµσαιρίνη C<br />
Ένα γλυταµικ ύ της ß-αλυσίδας αντικαθίσταται απ λυσίνη (ένα ασικ αµινύ): η κινητικτητά της είναι σηµαντικά µειωµένη. Στ<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, ι C, E και A 2 συµπίπτυν. ταν τ κλάσµα είναι > 15 %, πρέπει να τίθεται υπψία αιµσαιρινών C και<br />
E.<br />
Αιµσαιρίνη E<br />
Ένα γλυταµικ ύ της ß-αλυσίδας αντικαθίσταται απ λυσίνη: η αιµσαιρίνη E κινείται πως η αιµσαιρίνη C στ <strong>HYDRAGEL</strong><br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>. Αντίθετα µε την αιµσαιρίνη C, δεν διαωρίεται απ την αιµσαιρίνη A σε ιν διάλυµα [<strong>HYDRAGEL</strong> ACID(E)<br />
<strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>]. Αυτή η ιδιτητά της επιτρέπει τ διαωρισµ της E απ τη C.<br />
Αιµσαιρίνη D<br />
Ένα γλυταµικ ύ της ß-αλυσίδας αντικαθίσταται απ γλυταµίνη. Στ <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>, η αιµσαιρίνη κινείται<br />
ακριώς πως η αιµσαιρίνη S. Αντίθετα µε την αιµσαιρίνη S, η αιµσαιρίνη D δεν διαωρίεται απ την αιµσαιρίνη A σε ιν<br />
διάλυµα [<strong>HYDRAGEL</strong> ACID(E) <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong>]. Αυτή η ιδιτητά της επιτρέπει τ διαωρισµ της S απ την D.<br />
2. Πστικές διαταραές: Θαλασσαιµίες<br />
ι θαλασσαιµίες απτελύν µια ετεργενή µάδα γενετικών διαταραών αρακτηριµενων απ µειωµένη σύνθεση κάπιας απ τις<br />
πλυπεπτιδικές αλυσίδες της αιµσαιρίνης. µριακς µηανισµς αυτής της µείωσης δεν έει πλήρως περιγραεί.<br />
Υπάρυν δύ τύπι θαλασσαιµικών συνδρµων:
- 55 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Άλα θαλασσαιµίες<br />
αρακτηρίνται απ µείωση της σύνθεσης των α-αλυσίδων, µε απτέλεσµα επίπτωση στη σύνθεση λων των υσιλγικών<br />
αιµσαιρινών.<br />
Η περίσσεια των ß- και γ- αλυσίδων σε σέση µε τις α-αλυσίδες δηγεί στ σηµατισµ τετραµερών ωρίς α-αλυσίδες :<br />
• αιµσαιρίνη Bart = γ 4,<br />
• αιµσαιρίνη H = ß 4.<br />
Βήτα θαλασσαιµίες<br />
αρακτηρίνται απ µείωση της σύνθεσης των -αλυσίδων. Επηρεάεται µν η σύνθεση της αιµσαιρίνης A.<br />
Επµένως αυάννται τα πσστά των αιµσαιρινών F και A 2 σε σέση µε την αιµσαιρίνη A.<br />
3. Ηλεκτρρητικά πρίλ<br />
Ηλεκτρρητική<br />
κίνηση υσιλγικών<br />
αιµσαιρινών<br />
A(A 0 + A 1 ) A (A 0 + A 1 )<br />
F<br />
S - D<br />
A 2<br />
A2 - C - E<br />
καρνική ανυδράση καρνική ανυδράση<br />
σηµεί εαρµγής<br />
A 0 : Τ µη γλυκυλιωµέν κλάσµα της υσιλγικής αιµσαιρίνης τυ ενηλίκυ A.<br />
A 1 : Τ γλυκυλιωµέν κλάσµα της υσιλγικής αιµσαιρίνης τυ ενηλίκυ A.<br />
Στα παραπάνω πρίλ, η κάθδς είναι κάτω και η άνδς επάνω.<br />
Παρεµλές και περιρισµί.<br />
• Μην ρησιµπιείτε αιµλυµένα δείγµατα αίµατς.<br />
• ταν ανινεύεται µια παθλγική αιµσαιρίνη, η πία κινείται διαρετικά απ τιςκύριες παραλλαγές αιµσαιρίνης S, C, D και E,<br />
ρησιµπιήστε άλλα µέσα ταυτπίησης (π..ισηλεκτρική εστίαση, ηλεκτρρηση αλυσίδων σαιρίνης) ή συµυλευτείτε ή στείλτε<br />
τ δείγµα σε εειδικευµέν εργαστήρι.<br />
• Η πυκνµέτρηση της Hb F (ή πιασδήπτε άλλης ελάσσνς αιµσαιρίνης η πία κινείται κντά στα µείνα κλάσµατα) είναι<br />
ηµιπστική καθώς ι τιµές γίννται ανακριής κάτω απ τ 2 % - 3 % της λικής αιµσαιρίνης.<br />
• Μερικί µυγι “S” λαµάνυν θεραπεία µε “Hydrea”® (υδρυυρία) η πία µπρεί να επάγει παραγωγή εµρυϊκής αιµσαιρίνης.<br />
Η κινητικτητα της επαγµενης αιµσαιρίνης F στ <strong>HYDRAGEL</strong> 7 <strong>HEMOGLOBIN</strong>(E) έει σε ρισµένες περιπτώσεις διαπιστωθεί<br />
διαρετική απ τη υσιλγική αιµσαιρίνη F.<br />
• Σε δείγµατα τα πία έυν υλαθεί επί περισστερες απ 7 ηµέρες, τ απρν ίνς πίσω απ τ κλάσµα Hb A µπρεί να µετατραπεί<br />
σε καλώς εντπισµέν κλάσµα. Μην ερµηνεύετε τ κλάσµα αυτ ως πικιλία αιµσαιρίνης, π.. αιµσαιρίνες H ή Bart.<br />
Αντιµετώπιση πρληµάτων<br />
Καλέστε την Τενική Υπηρεσία τυ πρµηθευτή αν η ανάλυση δεν λειτυργεί παρλ πυ ι δηγίες πρετιµασίας και ύλαης των<br />
υλικών και ι δηγίες λειτυργίας τηρύνται πρσεκτικά.<br />
Τα Φύλλα ∆εδµένων Ασαλείας των αντιδραστηρίων των κιτ και πληρρίες για την ασαλή απρριψή τυς διατίθενται επίσης απ την<br />
Τενική Υπηρεσία τυ πρµηθευτή.<br />
∆Ε∆ΜΕΝΑ ΑΠ∆ΣΗΣ<br />
Ηλεκτρρητική κίνηση<br />
κύριων παθλγικών<br />
αιµσαιρινών<br />
λα τα δεδµένα απδσης ασίνται σε µια µελέτη η πία περιελάµανε υλικά και ργανα SEBIA <strong>HYDRAGEL</strong> και άλλ συγκρίσιµ<br />
εµπρικά διαθέσιµ σύστηµα µε gel αγαρης. Επιπρσθέτως, πραγµατπιήθηκαν µελέτες συµωνίας πυ η ταυτπίηση και η<br />
πστικπίηση των αιµσαιρινών έγιναν µε HPLC ή άλλες καθιερωµένες µεθδυς. Αντιπρσωπευτικά απτελέσµατα παρυσιάνται<br />
παρακάτω. λα τα ηλεκτρρήµατα ερµηνεύτηκαν πτικά. Τ πυκνµετρ SEBIA HYRYS ρησιµπιήθηκε για λες τις πυκνµετρήσεις<br />
συµπληρωµατικά πρς τα πτικά δεδµένα πυ κρίθηκε απαραίτητ.<br />
Αναπαραγωγιµτητα εντς της σειράς ανάλυσης<br />
Τρία δείγµατα αίµατς ηλεκτρρήθηκαν σε gel <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> απ την ίδια παρτίδα. Κάθε δείγµα έτρεε και στα<br />
15 ίνη κάθε gel. ακλυθς πίνακας δείνει τις µέσες τιµές, τις SD και τυς CV για κάθε αιµσαιρινικ κλάσµα στα τρία δείγµατα για<br />
τις εκατστιαίες τιµές για κάθε ίνς. Επιπλέν, καµία απ τις επαναλήψεις δεν έδωσε ψευδώς θετικ ή αρνητικ απτέλεσµα.<br />
| ΚΛΑΣΜΑ | Μ. | SD | CV (%) |<br />
| Φυσιλγικ αίµα |<br />
| Hb A | 97.4 | 0.1 | 0.1 |<br />
| Hb A | 2 2.6 | 0.1 | 5.3 |<br />
| Αυηµένη Hb A2 |<br />
| Hb A | 95.2 | 0.2 | 0.2 |<br />
| Hb A | 2 4.8 | 0.2 | 4.4 |<br />
| Αυηµένη Hb C |<br />
| Hb A | 56.7 | 0.4 | 0.8<br />
|<br />
|<br />
Hb C | 43.3 | 0.4 | 1.0 |
- 56 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
Αναπαραγωγιµτητα µεταύ σειρών ανάλυσης<br />
∆είγµατα αίµατς ηλεκτρρήθηκαν σε gel <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> απ µια παρτίδα. Τα αναλυθέντα δείγµατα περιελάµαναν<br />
επτά δείγµατα µε µια παθλγική αιµσαιρίνη (Hb S, Hb F ή Hb C) και δύ δείγµατα µε αυηµένη Hb A2 . ι µέσες τιµές, SD και CV<br />
υπλγίστηκαν απ τα δεδµένα για κάθε κλάσµα σε κάθε δείγµα. Τ εύρς των µέσων τιµών, SD και CV και µέσς CV απ τα<br />
συγκεντρωµένα δεδµένα για τα επιµέρυς κλάσµατα παρυσιάνται παρακάτω. Επιπλέν, καµία απ τις επαναλήψεις δεν έδωσε<br />
ψευδώς θετικ ή αρνητικ απτέλεσµα.<br />
| ΚΛΑΣΜΑ | Μ. | SD | CV (%) | ΜΕΣΣ CV (%) |<br />
| Hb A | 18.0 – 97.8 | 0.1 – 1.0 | 0.1 – 4.0 | 0.8 |<br />
| Hb F | 13.3 – 76.3 | 0.5 – 0.6 | 0.7 – 3.4 | 1.8 |<br />
| Hb C/E | 21.5 – 43.5 | 0.2 – 0.3 | 0.6 – 1.1 | 0.8 |<br />
| Hb S/D | 9.7 – 84.1 | 0.1 – 0.6 | 0.4 – 2.6 | 1.1<br />
| |<br />
Hb A | 2 2.2 – 5.7 | 0.1 – 0.2 | 2.3 – 7.6 | 4.0 |<br />
Ακρίεια – Ανίνευση ανωµαλιών της αιµσαιρίνης<br />
Εήντα τρία (63) διαρετικά δείγµατα αίµατς αναλύθηκαν µε <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> και άλλ συγκρίσιµ εµπρικά διαθέσιµ<br />
σύστηµα gel αγαρης. Τα δείγµατα αίµατς και η διαγνωστική τυς αιλγηση πρσέρθηκαν απ νσκµεί. Η διάγνωση ασιταν<br />
σε ηλεκτρρηση σε αλκαλικ και ιν gel και/ή HPLC. λες ι παθλγικές αιµσαιρίνες ή τα παθλγικά επίπεδα υσιλγικών<br />
αιµσαιρινών πυ ανινεύθηκαν µε τ <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> ρίσκνταν σε συµωνία µε τ συγκρίσιµ σύστηµα, τα<br />
απτελέσµατα απ τ νσκµεί και την κλινική διάγνωση. ∆εν υπήρε περίπτωση ψευδώς θετικύ, δηλ. ανίνευση µιας παθλγικής<br />
ώνης εκεί πυ δεν υπήρε τέτια ανωµαλία.<br />
Ακρίεια – Πστικς πρσδιρισµς της Hb A2 Τα επίπεδα Hb A2 µετρήθηκαν σε 51 δείγµατα αίµατς µε υσιλγικά και αυηµένα επίπεδα Hb A2 µετρήθηκαν µε πυκνµέτρηση των<br />
ηλεκτρρηµάτων πυ ελήθησαν µε τ <strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> και άλλ συγκρίσιµ εµπρικά διαθέσιµ σύστηµα gel<br />
αγαρης. ι τιµές απ τις δύ διαδικασίες αναλύθηκαν µε στατιστική επεεργασία γραµµικής παλινδρµησης. Τα απτελέσµατα της<br />
ανάλυσης παρυσιάνται παρακάτω (y = <strong>HYDRAGEL</strong>).<br />
| Συντελεστής συσέτισης | Τµή τυ y | Κλίση | Εύρς % τιµών |<br />
| | | | (Σύστηµα της SEBIA)<br />
| |<br />
0.973 | -0.344 | 0.963 | 1.5 – 5.7 |<br />
ΒΙΒΛΙΓΡΑΦΙΑ<br />
1. Fairbanks V.F., ed. (1980) Hemoglobinopathies and thalassemia: Laboratory methods and case studies. Brian C. Decker, New York.<br />
2. Galacteros F. (1986) Thalassémie, drépanocytose et autres hémoglobinopathies. Techniques et Biologie, 3, 174-178.<br />
3. Huisman T.H.J. and. Jonxis J.H.P (1977) The hemoglobinopathies: techniques of identification. Marcel Dekker, New York.<br />
4. Krauss J.S., Drew P.A., Jonah M.H., Trinh M., Shell S., Black L. and Baisden C.R. (1986) Densitometry and microchromatography compared for<br />
determination of the hemoglobin C and A 2 proportions in hemoglobin C and hemoglobin SC disease and in hemoglobin C trait. Clin. Chem. 32, 5,<br />
860-863.<br />
5. Livingstone C. (1986) The hemoglobinopathies. Edit. London.<br />
6. Maier-Redelsberger M., Girot R. (1989) Diagnostic biologique des maladies de l’hémoglobine. Feuillets de biologie, 170.<br />
7. Schneider R.G. (1978) Methods for detection of hemoglobin variants and hemoglobinopathies in the routine clinical laboratory. CRC Crit. Rev. Clin.<br />
Lab. Sci. 9, 243-271.<br />
8. Vovan L., Lara-Russo D., Orsini A. (1985) Diagnostic biologique des hémoglobinoses. Ann. Pédiat. 32, 9, 780-789.
For en dansk version af dette pakningsvedlæg, henvend Dem til den danske distributør af produkter fra SEBIA :<br />
ILS ApS Gydevang 22A DK-3450 Allerød<br />
Tlf : +45 48 14 18 50<br />
Fax : +45 48 14 18 60<br />
e-mail : ils@ilsdk.dk<br />
- 57 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
SEBIA INSTRUKTION - Dansk
1 2 3 4 5 6 7<br />
SCHÉMAS / FIGURES<br />
Figure 1 Figure 2<br />
Figure 3 Figure 4<br />
- 58 -<br />
<strong>HYDRAGEL</strong> <strong>HEMOGLOBIN</strong>(E) <strong>K20</strong> - 2005/03<br />
1 2 3 4 5 6 7<br />
1 2 3 4 5 6 7<br />
1 2 3 4 5 6 7
Parc Technologique Léonard de Vinci<br />
Rue Léonard de Vinci<br />
CP 8010 Lisses<br />
91008 EVRY CEDEX - FRANCE<br />
ISO 13485<br />
Benelux s.a. / n.v.<br />
Rue de la Fusée, 62<br />
Raketstraat, 62<br />
1130 Bruxelles / Brussel<br />
BELGIQUE / BELGIË<br />
GmbH<br />
Michael Henkel Straße 4-6<br />
36043 Fulda<br />
DEUTSCHLAND<br />
Hispania S.A.<br />
C/Sicilia, 394<br />
08025 Barcelona<br />
ESPAÑA<br />
Italia s.r.l.<br />
Via Antonio Meucci, 15/a<br />
Località Ponte a Ema<br />
50012 Bagno a Ripoli, Firenze<br />
ITALIA<br />
Inc.<br />
400-1705 Corporate Drive<br />
Norcross, Georgia 30093<br />
U.S.A.