- Page 2 and 3:
Osseointegration and Dental Implant
- Page 4 and 5:
Asbjorn Jokstad, DDS, PhD, is Profe
- Page 6 and 7:
vi Contents 4 Comprehensive Treatme
- Page 8 and 9:
viii Contents What Have We Learned
- Page 10 and 11:
Osseointegration and implant dentis
- Page 12 and 13:
xiv Contributing Authors of Dentist
- Page 14 and 15:
xvi Contributing Authors Engineerin
- Page 16 and 17:
The improvements in implant technol
- Page 18 and 19:
tion techniques related to dental i
- Page 20 and 21:
lum in most dental faculties worldw
- Page 22 and 23:
Table 1.1. Implant producers of the
- Page 24 and 25:
6 Osseointegration and Dental Impla
- Page 26 and 27:
8 Osseointegration and Dental Impla
- Page 28 and 29:
10 Osseointegration and Dental Impl
- Page 30 and 31:
12 Osseointegration and Dental Impl
- Page 32 and 33:
14 Osseointegration and Dental Impl
- Page 34 and 35:
16 Osseointegration and Dental Impl
- Page 36 and 37:
18 Osseointegration and Dental Impl
- Page 38 and 39:
20 Osseointegration and Dental Impl
- Page 40 and 41:
22 Osseointegration and Dental Impl
- Page 42 and 43:
24 Osseointegration and Dental Impl
- Page 44 and 45:
26 Osseointegration and Dental Impl
- Page 46 and 47:
28 Osseointegration and Dental Impl
- Page 48 and 49:
30 Osseointegration and Dental Impl
- Page 50 and 51:
32 Osseointegration and Dental Impl
- Page 52 and 53:
34 Osseointegration and Dental Impl
- Page 54 and 55:
36 Osseointegration and Dental Impl
- Page 56 and 57:
38 Osseointegration and Dental Impl
- Page 58 and 59:
40 Osseointegration and Dental Impl
- Page 60 and 61:
42 Osseointegration and Dental Impl
- Page 62 and 63:
44 Osseointegration and Dental Impl
- Page 64 and 65: 46 Osseointegration and Dental Impl
- Page 66 and 67: 48 Osseointegration and Dental Impl
- Page 68 and 69: 50 Osseointegration and Dental Impl
- Page 70 and 71: 52 Osseointegration and Dental Impl
- Page 72 and 73: 54 Osseointegration and Dental Impl
- Page 74 and 75: 56 Osseointegration and Dental Impl
- Page 76 and 77: 58 Osseointegration and Dental Impl
- Page 78 and 79: 60 Osseointegration and Dental Impl
- Page 80 and 81: 62 Osseointegration and Dental Impl
- Page 82 and 83: 64 Figure 4.1a. Patient was diagnos
- Page 84 and 85: 66 Osseointegration and Dental Impl
- Page 86 and 87: 68 Osseointegration and Dental Impl
- Page 88 and 89: 70 Osseointegration and Dental Impl
- Page 90 and 91: Table 4.1. Distribution of tooth lo
- Page 92 and 93: 74 Osseointegration and Dental Impl
- Page 94 and 95: 76 Osseointegration and Dental Impl
- Page 96 and 97: 78 Osseointegration and Dental Impl
- Page 98 and 99: 80 Osseointegration and Dental Impl
- Page 100 and 101: 82 Osseointegration and Dental Impl
- Page 102 and 103: 84 Osseointegration and Dental Impl
- Page 104 and 105: 86 Osseointegration and Dental Impl
- Page 106 and 107: 88 Osseointegration and Dental Impl
- Page 108 and 109: 90 Osseointegration and Dental Impl
- Page 110 and 111: 92 Osseointegration and Dental Impl
- Page 112 and 113: 94 Osseointegration and Dental Impl
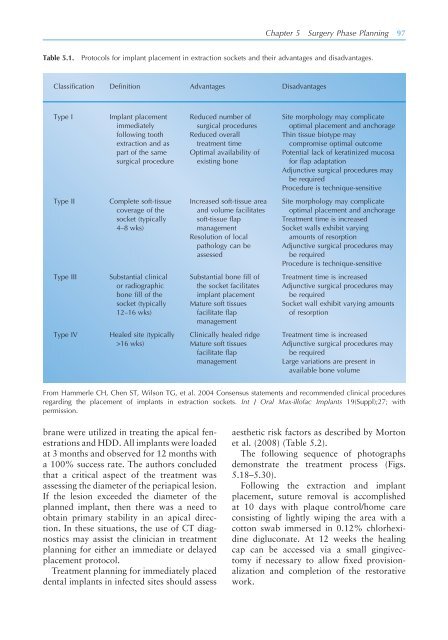
- Page 116 and 117: 98 Osseointegration and Dental Impl
- Page 118 and 119: Figure 5.23. The implant bed prepar
- Page 120 and 121: 102 Osseointegration and Dental Imp
- Page 122 and 123: 104 Osseointegration and Dental Imp
- Page 124 and 125: 106 Osseointegration and Dental Imp
- Page 126 and 127: e f Figures 5.32e and f. Following
- Page 128 and 129: 110 Osseointegration and Dental Imp
- Page 130 and 131: 112 Osseointegration and Dental Imp
- Page 132 and 133: 114 Osseointegration and Dental Imp
- Page 134 and 135: 116 Osseointegration and Dental Imp
- Page 136 and 137: 118 Osseointegration and Dental Imp
- Page 138 and 139: Figure 6.5a. Preoperative radiograp
- Page 140 and 141: Figure 6.7a. Preoperative CT scan i
- Page 142 and 143: 124 Osseointegration and Dental Imp
- Page 144 and 145: 126 Osseointegration and Dental Imp
- Page 146 and 147: a. b. 128 Osseointegration and Dent
- Page 148 and 149: 130 Osseointegration and Dental Imp
- Page 150 and 151: Figure 6.19. Augmentation of the in
- Page 152 and 153: 134 Osseointegration and Dental Imp
- Page 154 and 155: 136 Osseointegration and Dental Imp
- Page 156 and 157: 138 Osseointegration and Dental Imp
- Page 158 and 159: 140 Osseointegration and Dental Imp
- Page 160 and 161: 142 Osseointegration and Dental Imp
- Page 162 and 163: 144 Osseointegration and Dental Imp
- Page 164 and 165:
146 Osseointegration and Dental Imp
- Page 166 and 167:
148 Osseointegration and Dental Imp
- Page 168 and 169:
150 Osseointegration and Dental Imp
- Page 170 and 171:
152 Osseointegration and Dental Imp
- Page 172 and 173:
154 Osseointegration and Dental Imp
- Page 174 and 175:
156 Osseointegration and Dental Imp
- Page 176 and 177:
158 Osseointegration and Dental Imp
- Page 178 and 179:
160 Osseointegration and Dental Imp
- Page 180 and 181:
162 Osseointegration and Dental Imp
- Page 182 and 183:
164 Osseointegration and Dental Imp
- Page 184 and 185:
8 Pre-implant Surgical Intervention
- Page 186 and 187:
Figure 8.1. Sinus core 100% Bio-Oss
- Page 188 and 189:
Figure 8.8. Meisinger balloon contr
- Page 190 and 191:
ing bone formation in maxillary sin
- Page 192 and 193:
and concern for our patients, to ma
- Page 194 and 195:
growth factors have been studied ex
- Page 196 and 197:
clinical benefi t in the long-term
- Page 198 and 199:
composite bone graft: Preliminary r
- Page 200 and 201:
9 Biomaterials and Substances for S
- Page 202 and 203:
one graft in combination with a bar
- Page 204 and 205:
Figure 9.5. Photomicrograph of trep
- Page 206 and 207:
to harvest autogenous bone or use a
- Page 208 and 209:
the canine supraalveolar, peri-impl
- Page 210 and 211:
hBMP-2/ACS has also been shown to s
- Page 212 and 213:
References Adell R, Lekholm U, Rock
- Page 214 and 215:
10 Implant Surgery Interventions TH
- Page 216 and 217:
Figure 10.4. Interactive interpreta
- Page 218 and 219:
Figure 10.12. Graft marrow complex
- Page 220 and 221:
Figure 10.20. Complex 3-D aesthetic
- Page 222 and 223:
THE HEALING BONE-IMPLANT INTERFACE:
- Page 224 and 225:
was designed to resemble a more con
- Page 226 and 227:
A C BID (microns) 50 45 40 35 30 25
- Page 228 and 229:
sive strains exceeding 30% in the e
- Page 230 and 231:
214 Osseointegration and Dental Imp
- Page 232 and 233:
216 Osseointegration and Dental Imp
- Page 234 and 235:
218 Osseointegration and Dental Imp
- Page 236 and 237:
220 Osseointegration and Dental Imp
- Page 238 and 239:
222 Osseointegration and Dental Imp
- Page 240 and 241:
INFLUENCES OF IMPLANT DESIGN AND SU
- Page 242 and 243:
numerous experimental studies (for
- Page 244 and 245:
Figure 13.2. Microphotograph of an
- Page 246 and 247:
a Clinical Experience with “Short
- Page 248 and 249:
as anchorage units during orthodont
- Page 250 and 251:
———. 1985. Introduction to os
- Page 252 and 253:
Rocci A, Martignoni M, Burgos P, Go
- Page 254 and 255:
240 Osseointegration and Dental Imp
- Page 256 and 257:
242 Osseointegration and Dental Imp
- Page 258 and 259:
244 Osseointegration and Dental Imp
- Page 260 and 261:
246 Osseointegration and Dental Imp
- Page 262 and 263:
Figure 14.17. A clinical situation
- Page 264 and 265:
250 Osseointegration and Dental Imp
- Page 266 and 267:
252 Osseointegration and Dental Imp
- Page 268 and 269:
INTEGRATION OF BIOLOGICAL PRINCIPLE
- Page 270 and 271:
Figure 15.1. Scanning electron micr
- Page 272 and 273:
process of bone bonding in vitro an
- Page 274 and 275:
e g Recent new knowledge may infl u
- Page 276 and 277:
Figure 15.5a. Prepared second left
- Page 278 and 279:
Baylink DJ, Wergedal JE, et al. 199
- Page 280 and 281:
mandible. Clin Oral Implants Res 8(
- Page 282 and 283:
STABILITY OF IMPLANT- ABUTMENT CONN
- Page 284 and 285:
fl at to fl at joints. With most in
- Page 286 and 287:
Figure 16.8. A solid one-piece impl
- Page 288 and 289:
Table 16.1. planning level & decisi
- Page 290 and 291:
When considering immediate restorat
- Page 292 and 293:
17 The Transmucosal Component and t
- Page 294 and 295:
Chapter 17 Transmucosal Component a
- Page 296 and 297:
Chapter 17 Transmucosal Component a
- Page 298 and 299:
Chapter 17 Transmucosal Component a
- Page 300 and 301:
Chapter 17 Transmucosal Component a
- Page 302 and 303:
Chapter 17 Transmucosal Component a
- Page 304 and 305:
Figure 17.14. CAD view (CAM StructS
- Page 306 and 307:
Chapter 17 Transmucosal Component a
- Page 308 and 309:
CONTEMPORARY DENTAL IMPLANTS AND CL
- Page 310 and 311:
the bone level at the time of impla
- Page 312 and 313:
94%. Forty-two percent (226) of the
- Page 314 and 315:
Based on the fi ndings of this stud
- Page 316 and 317:
Chapter 18 The Implant Design and C
- Page 318 and 319:
Figure 18.12b. The PrimaConnex TM i
- Page 320 and 321:
Hatley CL, Cameron SM, Cuenin MF, P
- Page 322 and 323:
emoval. Pract Periodont Aesthet Den
- Page 324 and 325:
312 Osseointegration and Dental Imp
- Page 326 and 327:
314 Osseointegration and Dental Imp
- Page 328 and 329:
316 Osseointegration and Dental Imp
- Page 330 and 331:
318 Osseointegration and Dental Imp
- Page 332 and 333:
320 Osseointegration and Dental Imp
- Page 334 and 335:
322 Table 19.2. Systematic reviews
- Page 336 and 337:
324 Osseointegration and Dental Imp
- Page 338 and 339:
Table 19.5. Clinical trials with fo
- Page 340 and 341:
328 Osseointegration and Dental Imp
- Page 342 and 343:
330 Osseointegration and Dental Imp
- Page 344 and 345:
332 Osseointegration and Dental Imp
- Page 346 and 347:
334 Osseointegration and Dental Imp
- Page 348 and 349:
336 Osseointegration and Dental Imp
- Page 350 and 351:
338 Osseointegration and Dental Imp
- Page 352 and 353:
340 Osseointegration and Dental Imp
- Page 354 and 355:
342 Osseointegration and Dental Imp
- Page 356 and 357:
344 Osseointegration and Dental Imp
- Page 358 and 359:
346 Osseointegration and Dental Imp
- Page 360 and 361:
348 Osseointegration and Dental Imp
- Page 362 and 363:
350 Osseointegration and Dental Imp
- Page 364 and 365:
352 Osseointegration and Dental Imp
- Page 366 and 367:
354 Osseointegration and Dental Imp
- Page 368 and 369:
356 Osseointegration and Dental Imp
- Page 370 and 371:
358 Osseointegration and Dental Imp
- Page 372 and 373:
360 Osseointegration and Dental Imp
- Page 374 and 375:
362 Osseointegration and Dental Imp
- Page 376 and 377:
364 Osseointegration and Dental Imp
- Page 378 and 379:
366 Osseointegration and Dental Imp
- Page 380 and 381:
368 Osseointegration and Dental Imp
- Page 382 and 383:
370 Osseointegration and Dental Imp
- Page 384 and 385:
23 Dental Implants in the Habilitat
- Page 386 and 387:
Figure 23.2. Severe loss of vertica
- Page 388 and 389:
Figure 23.8. The planned restoratio
- Page 390 and 391:
Figure 23.17. Occlusal view of maxi
- Page 392 and 393:
24 Minimum Competency for Providing
- Page 394 and 395:
tially restricted to perhaps only t
- Page 396 and 397:
386 Appendix Pre-implant Surgical I
- Page 398 and 399:
388 Appendix Michael A. Pikos Certi
- Page 400 and 401:
390 Appendix Patient Focus on Neuro
- Page 402 and 403:
392 Appendix periodontal plastic an
- Page 404 and 405:
394 Appendix the Norwegian Society
- Page 406 and 407:
396 Appendix prosthodontics. Dr. Kn
- Page 408 and 409:
398 Appendix Myron Nevins Dr. Myron
- Page 410 and 411:
400 Appendix Universidad de los And
- Page 412 and 413:
402 Appendix American College of Pr
- Page 414 and 415:
The University of Toronto, Faculty
- Page 416 and 417:
406 Index Animal studies, 8-9. See
- Page 418 and 419:
408 Index research design, 347 rese
- Page 420 and 421:
410 Index FDA. See Food and Drug Ad
- Page 422 and 423:
412 Index complications, 21t data e
- Page 424 and 425:
414 Index Neoss Bimodal, 229 Neukam
- Page 426 and 427:
416 Index RANKL, 219 Rare disorders
- Page 428 and 429:
418 Index Tatum, Hilt, 167 Taylor,