MassHealth and You Guide - Mass.Gov
MassHealth and You Guide - Mass.Gov
MassHealth and You Guide - Mass.Gov

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
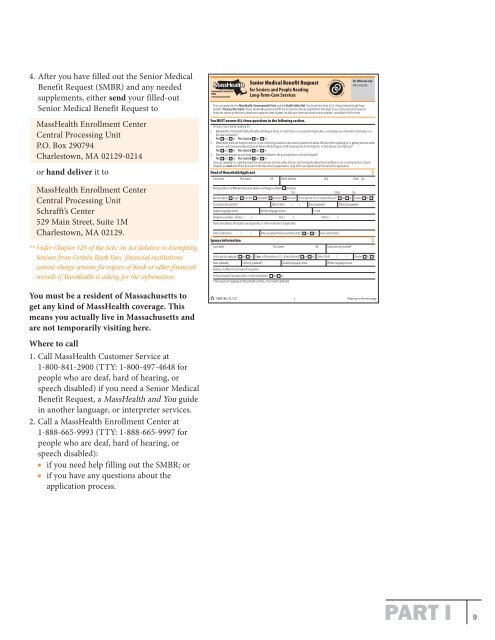
4. After you have filled out the Senior Medical<br />
Benefit Request (SMBR) <strong>and</strong> any needed<br />
supplements, either send your filled-out<br />
Senior Medical Benefit Request to<br />
<strong><strong>Mass</strong>Health</strong> Enrollment Center<br />
Central Processing Unit<br />
P.O. Box 290794<br />
Charlestown, MA 02129-0214<br />
or h<strong>and</strong> deliver it to<br />
<strong><strong>Mass</strong>Health</strong> Enrollment Center<br />
Central Processing Unit<br />
Schrafft’s Center<br />
529 Main Street, Suite 1M<br />
Charlestown, MA 02129.<br />
** Under Chapter 125 of the Acts: An Act Relative to Exempting<br />
Seniors from Certain Bank Fees, financial institutions<br />
cannot charge seniors for copies of bank or other financial<br />
records if <strong><strong>Mass</strong>Health</strong> is asking for the information.<br />
<strong>You</strong> must be a resident of <strong>Mass</strong>achusetts to<br />
get any kind of <strong><strong>Mass</strong>Health</strong> coverage. This<br />
means you actually live in <strong>Mass</strong>achusetts <strong>and</strong><br />
are not temporarily visiting here.<br />
Where to call<br />
1. Call <strong><strong>Mass</strong>Health</strong> Customer Service at<br />
1-800-841-2900 (TTY: 1-800-497-4648 for<br />
people who are deaf, hard of hearing, or<br />
speech disabled) if you need a Senior Medical<br />
Benefit Request, a <strong><strong>Mass</strong>Health</strong> <strong>and</strong> <strong>You</strong> guide<br />
in another language, or interpreter services.<br />
2. Call a <strong><strong>Mass</strong>Health</strong> Enrollment Center at<br />
1-888-665-9993 (TTY: 1-888-665-9997 for<br />
people who are deaf, hard of hearing, or<br />
speech disabled):<br />
if you need help filling out the SMBR; or<br />
if you have any questions about the<br />
application process.<br />
Commonwealth of <strong>Mass</strong>achusetts<br />
EOHHS<br />
www.mass.gov/masshealth<br />
SMBR (Rev. 01/13)<br />
Senior Medical Benefit Request<br />
for Seniors <strong>and</strong> People Needing<br />
Long-Term-Care Services<br />
For office use only<br />
Date received:<br />
This is an application for <strong><strong>Mass</strong>Health</strong>, Commonwealth Care, <strong>and</strong> the Health Safety Net. <strong>You</strong> do not have to be a U.S. citizen/national to get these<br />
benefits. Please print clearly. Please answer all questions <strong>and</strong> fill out all sections <strong>and</strong> any supplements that apply to you. If you need more space to<br />
finish any section on this form, please use a separate sheet of paper (include your name <strong>and</strong> social security number), <strong>and</strong> attach it to this form.<br />
<strong>You</strong> MUST answer ALL three questions in the following section.<br />
Are you or your spouse applying for:<br />
1. <strong><strong>Mass</strong>Health</strong> or the Health Safety Net while still living at home, in a rest home, in an assisted-living facility, a continuing-care retirement community, or a<br />
life-care community?<br />
<strong>You</strong> yes no <strong>You</strong>r spouse yes no<br />
2. <strong><strong>Mass</strong>Health</strong> while still living at home or in one of the living situations described in question #1 above AND also either applying for or getting services under<br />
a Home- <strong>and</strong> Community-Based Services Waiver, PACE (Program of All-Inclusive Care for the Elderly), or SCO (Senior Care Options)?<br />
<strong>You</strong> yes no <strong>You</strong>r spouse yes no<br />
3. <strong><strong>Mass</strong>Health</strong> because you are living in a medical institution, like a nursing home or chronic hospital?<br />
<strong>You</strong> yes no <strong>You</strong>r spouse yes no<br />
If you are applying for or getting long-term-care services at home under a Home- <strong>and</strong> Community-Based Services Waiver, or in a nursing home or chronic<br />
hospital, you must also fill out all or part of the blue sheet (Supplement A: Long-Term-Care Questions) at the end of this application.<br />
Head of Household/Applicant<br />
Last name First name MI Street address City State Zip<br />
Mailing address (if different from street address or if living in a shelter) homeless<br />
City State Zip<br />
Marital status single married separated widowed divorced Is this person a U.S. citizen/national? yes no Gender M F<br />
Social security number* Date of birth / / Race (optional) Ethnicity (optional)<br />
Spoken language choice Written language choice E-mail<br />
Telephone numbers Home: ( ) Cell: ( ) Work: ( )<br />
Name <strong>and</strong> address of hospital, nursing facility, or other institution (if applicable)<br />
Date of admission / / Were you placed here by another state? yes no If yes, what state?<br />
Spouse Information<br />
Last name First name MI Social security number*<br />
Is this person applying? yes no If yes, is this person a U.S. citizen/national? yes no Date of birth / / Gender M F<br />
Race (optional) Ethnicity (optional) Spoken language choice Written language choice<br />
Address, if different from head of household<br />
Is this a hospital, nursing facility, or other institution? yes no<br />
* Not required if applying for <strong><strong>Mass</strong>Health</strong> Limited or the Health Safety Net.<br />
1 Please go to the next page<br />
HOH<br />
HOH<br />
PART I 9