

Common Lameness Problems In Endurance Horses - Australian ...
Common Lameness Problems In Endurance Horses - Australian ...
Common Lameness Problems In Endurance Horses - Australian ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
COMMON LAMENESS PROBLEMS<br />
IN ENDURANCE HORSES<br />
By John Kohnke BVSc RDA<br />
The major causes of lameness in endurance horses are largely related to ‘wear and tear’<br />
injuries as a result of concussion and the cumulative loading of joints and tendons by<br />
repetitive long distance exercise.<br />
The incidence of lameness is reduced in a well conditioned horse that has adapted and<br />
strengthened its musculo-skeletal structures to withstand the rigors of training. The<br />
Arabian bloodlines used for endurance competition have been selected over many years<br />
for their suitability and soundness for long distance exercise. Only mature horses over 5<br />
years of age are permitted to compete in AERA rides which significantly reduces the risk<br />
of bone and joint lameness associated with overloading during training and competition<br />
in younger, immature horses used in racing and other horse sports.<br />
However, the cumulative effects of many kilometres of training, particularly over hard,<br />
concussive surfaces, compounded by conformational weaknesses, poor farriery and<br />
nutritional imbalances, can increase the incidence of bone, joint and tendon injuries,<br />
especially as a horse ages and accumulates 1000’s of kilometres in training and<br />
competition. Expert health care and a well balanced diet, will ensure that many retiree<br />
endurance horses still remain sound into their senior years.<br />
<strong>In</strong> this review, I have grouped the common lamenesses into concussive or repetitive<br />
“wear and tear” type injuries, those associated with conformational weakness and poor<br />
farriery, and other common problems. Although many musculo-skeletal conditions can<br />
occur in endurance horses, I have only included the most common lameness problems.<br />
<strong>Lameness</strong> due to “Wear and Tear”<br />
<strong>In</strong> most athletic horses, lameness accounts for up to 70% of lost training days or lay off<br />
from training, and in endurance horses, concussion to the hoof structures and joints of the<br />
lower limbs in particular, is the major cause of downtime from training. Conformational<br />
weaknesses, such as upright pasterns and offset front cannon bones, often aggravated by<br />
developmental abnormalities in growing horses due to dietary imbalances, increase the<br />
risk of bone and joint overload and concussive failure.<br />
Pedal Bone <strong>Problems</strong><br />
The pedal bone and the coffin joint inside the hoof capsule are subjected to a high degree<br />
of concussion, which can result in demineralisation, arthritis and eventual lameness.<br />
Although the condition of pedal osteitis, or inflammation of one or both of the front limb<br />
pedal bones, is most common in immature thoroughbred racehorses, the cumulative
effects of weight bearing and concussion on compacted surfaces can lead to interference<br />
with blood perfusion, bone dissolution with initial subtle lameness on soft surfaces that<br />
compact under the soles Affected horses exhibit ‘shuffling’ and ‘proppy’ gait,<br />
especially on soft surfaces which is exacerbated after concussive exercise. As the pedal<br />
bone becomes more demineralised in more severe cases, in older campaigners, there is an<br />
increased risk of fractures of the outer sides of the pedal bones where greatest<br />
demineralisation and increase in vascular channelling occurs, as seen on X-ray.<br />
Ensuring that a horse’s hooves are trimmed and shod to reduce sole contact, and fitting<br />
underpads to horses with thin or flat soles, will help to reduce the risk and the severity of<br />
pedal bone concussion and associated lameness. <strong>Horses</strong> that have had any previous<br />
history of laminitis or mild founder, with any degree of downward rotation of the pedal<br />
bones and collapse of the soles, are more prone to concussive hoof injury. It is important<br />
that they are shod to support and protect the under surface of the sole and frog.<br />
Although demineralization cannot generally be reversed, even by providing calcium and<br />
bone minerals in excess relative to dietary requirements and resting the horses for<br />
extended periods, therapy to increase blood perfusion within the hoof and pedal bone,<br />
such as by fitting magnetic bell boots overnight, may help to slow down the progressive<br />
demineralisation.<br />
Navicular Syndrome and Coffin Joint Arthritis<br />
Although “navicular syndrome”, as it is now termed, is largely influenced by genetic<br />
predisposition, especially in horses with naturally small, contracted hooves, the<br />
concussive effects of long distance exercise can result in vascular changes within the<br />
navicular bone and arthritis in the associated coffin join. This progressive deterioration is<br />
now collectively referred to as navicular syndrome, rather than navicular disease.<br />
The navicular bone acts as a pulley implanted in the relative avascular upper structure of<br />
the deep flexor tendon as it passes over the coffin joint to attach on the under surface of<br />
the pedal bone. High loading forces in exercising horses of up to 40,000 Newtons (1000<br />
lbs per square inch) are thought to restrict blood supply to the navicular bone.<br />
Although early stage navicular deterioration is often responsive to oral vasodilating<br />
therapy (termed isoxsuprine responsive), new studies reveal that fluid pressure<br />
accumulates within the navicular structure to cause demineralisation and internal collapse<br />
of the navicular body. The fluid eventually erupts through the articular surface of the<br />
navicular bone into the coffin joint, resulting in progressive arthritic change. Early<br />
navicular disease is recognized by a stumbling gait, especially when moving downhill,<br />
increased wear on the toes of shoes, and a “scratchy” gait that often warms out on<br />
exercise returning to be more obvious for 2-3 days after a ride. <strong>Horses</strong> often appear<br />
to be “tied-up in the shoulders” because of the shortened stride length, and stand resting<br />
on the toe of the affected hoof(s) to relieve pressure on the painful navicular bone.
The progressive deterioration and associated pain of diminished blood supply and internal<br />
fluid accumulation, results in avoidance of heel contact, with development of higher<br />
and contracted heels, and deeper grooves (sulci) around the frog, with a progressive<br />
chronic lameness. Diagnosis by nerve blocks, X-rays and coffin joint anaesthesia can<br />
help confirm navicular syndrome in chronic cases.<br />
The use of rolled toes to hasten break-over and support to the heel area with eggbar<br />
shoes, with or without heel wedges, will improve comfort and gait in early cases. Daily<br />
supplementation with glucosamine based oral joint preparations (reviewed in a separate<br />
section in this publication) can provide relief of early navicular related arthritic changes<br />
in the coffin joint, in conjunction with therapeutic shoeing and regular hoof care.<br />
Recently, the use of magnetic bell boots with strong magnetic fields above 1500 gauss<br />
(Animal Magnetism, Wyong, Aust) have been observed to provide relief in early cases of<br />
navicular syndrome, presumably by improving blood perfusion within the navicular bone<br />
and hoof structure.<br />
Laminitis<br />
Laminitis caused by tearing and deterioration of the laminae attachment of the hoof wall<br />
to the pedal bone within the hoof capsule, can occur as a result of extreme concussive<br />
exercise, often referred historically as “road founder”. Although 80% of laminitic<br />
conditions result from starch overload from excess grain (such as corn) or very lush<br />
pastures (containing fructan sugars and other soluble non-structural sugars), during spring<br />
in grazing horses, the average endurance horse in training, with a controlled diet and “fit”<br />
body condition aided by regular exercise, is unlikely to develop a carbohydrate overlaod<br />
type “founder” condition. Concussive exercise on hard ground at speed can result in<br />
physical tearing of the laminae, with shortened stride and a ‘leaning back on the heels’<br />
stance, often with an increased digital pulse. Prompt first aid with ice packs and antiinflammatories,<br />
and rest, as prescribed by a veterinarian, will help resolve milk tearing of<br />
the laminae in an otherwise healthy hoof.<br />
Ring Bone<br />
The bony growth referred to as “ring bone” associated with the pastern and coffin joints<br />
is often a result of long term concussion, and is most prevalent in Arabian and other<br />
breeds of horses with lightly boned and long sloping pasterns and turned out toe<br />
conformation. <strong>In</strong>itially, peri-articular bone reaction, due to collateral ligament tearing<br />
away from the pastern bones and bone surface (periosteal) reaction above or below the<br />
joint, as a result of twisting and overflexion of the pastern joint, can cause shortening of<br />
the stride and a ‘scratchy’ gait. However, continued concussion, especially when the<br />
collateral ligaments are stretched and allow excess bone on bone movement within the<br />
pastern joint, can lead to cartilage damage and subchondral bone pain within the pastern<br />
joint. This results in chronic intra-articular ring bone in one or both front limbs. The<br />
lameness associated with early peri-articular ring bone can be alleviated by judicious use<br />
of anti-inflammatories, including DMSO and Dermcusal (Vetsearch, Australia), but if the<br />
bony proliferation encroaches into the pastern joint, then arthritic changes develop which
often require more extensive and long term anti-inflammatory medication, and in severe<br />
cases, retirement from competitive riding.<br />
Side Bone<br />
<strong>Lameness</strong> due to partial fracture of the lateral cartilages within the heel area that continue<br />
to flex as they mineralise to bone in long distance horses over 8 years of age, can lead to<br />
lameness in horses being worked over hilly terrain and sloping trails in training.<br />
Diagnosis is confirmed by X-ray, and in severe cases, surgical removal of the incomplete<br />
or fractured “side bones” is the only alternative where a horse exhibits discomfort and<br />
lameness during training.<br />
Fetlock Joint Sprain and Arthritis<br />
<strong>In</strong> young performance horses, such as 2 year olds in racing, fetlock lameness is the major<br />
cause of wastage. It results from overloading, concussion and overflexion with joint<br />
sprain of the fetlock structures, followed by internal cartilage and subchondral bone<br />
deterioration, leading to chronic arthritis. Conversely, in the mature endurance horse, the<br />
incidence of fetlock sprain is generally low and related to accidental sprain on uneven<br />
ground or a fall, rather than overflexion at speed. Aged campaigners are prone to<br />
developing changes within all joints, including the forelimb fetlock joints, often seen<br />
externally as joint ‘wind galls’ due to joint capsule and tendon bursa enlargement<br />
resulting from long term “wear and tear” of accumulated long distance exercise. The use<br />
of oral joint therapies, even as an ‘insurance’ against cartilage deterioration, have been<br />
widely credited as a worthwhile preventative, and in the case of developing arthritic<br />
change, fetlock support, and ‘joint foods’ are a useful form of therapy to maintain<br />
soundness in endurance horses.<br />
Splints<br />
<strong>Horses</strong> with badly offset front cannon bones (“bench knees”) have a higher risk of<br />
developing ‘high’ splints that involve the upper end of the front cannon bone under the<br />
knee joint, because the medial splint bone (4 th metacarpal bone inside the cannon bone)<br />
forms part of the lower knee joint surface. <strong>In</strong>itially, ‘high’ splints cause shortening of the<br />
stride as the ligaments that attach the splint bone to the upper cannon bone shaft are torn<br />
away from the cannon bone, as more weight is loaded onto the “bench knee” area. This<br />
is a particular problem in a young horse being ridden over long distances, especially<br />
downhill, when more weight is transferred to the front limbs. However, by 5-6 years of<br />
age, the ligament attachments begin to turn to bone (ossify), attaching the upper third of<br />
the splint to the cannon bone by a bony bridge, reducing the risk of ‘high’ splints. During<br />
the process of developing a more permanent bony attachment, inflammation and bony<br />
reaction can cause lameness, with shortening of the stride. <strong>In</strong>itial rest, followed by a<br />
reduction in the level of exercise, with discomfort alleviated by cold packs and antiinflammatories<br />
such as ‘Bute’ and topical DMSO, can help to “work out” a high splint so<br />
that it resolves over 4-6 weeks to form a more permanent bony attachment.
Occasionally, the upper section of a splint bone can be fractured by a knock or being<br />
tangled up with a stick when riding. Rest for 4-6 weeks, support bandaging and cold<br />
packs are the favoured forms of therapy, relative to the degree of fracture or bone<br />
displacement.<br />
‘Low’ splints, which can develop on the inside or outside of the cannons, where the splint<br />
bones become thin and are vulnerable to trauma and fracture, are not uncommon,<br />
characterised by local swelling, pain and lameness.<br />
Where the lower end of the splint bone is fractured, often concluded because cold packs,<br />
rest and bandaging do not resolve the pain or discomfort within 5-7 days (X-rays can<br />
confirm a fracture), it is best to rest the horse and apply anti-inflammatories and support<br />
bandaging, including magnetic wraps over the area to aid bone repair.<br />
Knee and Shoulder Joints<br />
Because endurance horses are mature when training is commenced, the incidence of knee<br />
and shoulder joint arthritis is generally low. However, often a ‘tying-up’ type gait that<br />
appears to be located in the shoulders, is most commonly due to lower limb and hoof<br />
conditions below the fetlock, seen as restricted stride and shoulder extension resulting<br />
in a ‘scratchy’, uneven gait. Diagnosis of the location and management under<br />
veterinary supervision is recommended. <strong>Horses</strong> with poor conformation, such as ‘back at<br />
the knee’, ‘deviation at the knee’ or ‘over at the knee’ have a higher risk of developing<br />
knee joint conditions and may not withstand long term training and competition.<br />
Tendon <strong>In</strong>juries<br />
The structural development and load bearing capacity of elastic tendon and suspensory<br />
ligament tissues is influenced by exercise, cumulative loading and aging, with tendons<br />
operating almost to their functional limit and developing elastic rebound fatigue during<br />
exercise. Once structurally formed by 5 months of age in a young horse, tendons have<br />
very limited, if any, capacity to regenerate after injury and can only repair damaged<br />
collagen fibrils within the tendon bundles.<br />
The strength, mechanical strain resistance and elastic capacity of tendons are dependant<br />
on the nutritional input, and the structural matrix organisation and loading capacity within<br />
the tendon fibre bundles. Tendon strength and resilience is only stimulated and<br />
maintained by progressive loading in a step-wise manner while training.<br />
<strong>In</strong> endurance horses, sudden overloading of tendons by slipping, falls or uphill climbs<br />
which are already suffering cumulative fatigue, is a common cause of a ‘bowed’ tendon<br />
or tendonitis, with highest incidence in the superficial digital flexor tendon (SDFT) on the<br />
rear of the front limbs. Traumatic injury to tendons with internal bruising by knocks and<br />
falls is also a common cause of tendonitis and associated swelling and lameness.
It is beyond the scope of this review to fully discuss tendon injuries and their<br />
management. However, prompt first aid to limit internal blood vessel haemorrhage when<br />
core tendon fibres tear or rupture, or external trauma results in bruising, is paramount to<br />
the long term repair and rehabilitation of tendons. Prompt application of cold therapy by<br />
ice or a cold pack (cold water hosing is not ‘cold’ enough), under an elastic bandage,<br />
repeated 3-4 times per day, and anti-inflammatories such as ‘bute’ even for minor tendon<br />
‘bumps’ or ‘bows’, will help control internal haemorrhage and inflammation and limit the<br />
extent of long term structural damage to injured tendon tissue. Rest and confinement to a<br />
stable or yard, with support bandaging of the opposite limb, and ultrasound scanning of<br />
the injured area, are important management procedures to reduce the risk of repeated<br />
injury and assist in formulating an appropriate rehabilitation program over a 9-12 month<br />
period. Routine icing of tendons within 5-10 minutes after exercise to remove heat and<br />
inflammation is considered a useful aid to reducing the risk of tendon injuries in long<br />
distance horses. Ensuring the horse has adequate heel height and avoiding long toes will<br />
help to reduce abnormal tendon loading.<br />
Hock Conditions<br />
The hock joints and associated tendon and ligament structures are prone to concussive<br />
injury, especially if inherent conformational weaknesses such as “sickle hock” or<br />
“straight hocks” increase the direct loading or sprain forces on the hocks. Working<br />
horses on hilly terrain increases the loading of the hock joints as horses climb, with<br />
development of initial internal inflammation and increased joint fluid (referred to as ‘bog<br />
spavin’), which can develop in time to out growths and bony arthritic change within the<br />
hock joints, or ‘bone spavin’.<br />
Hock joint arthritic changes are usually slow to develop and have an insidious,<br />
progressive onset with restricted stride and ‘scratchy’, uneven gait which warms out on<br />
exercise. <strong>In</strong> a horse with a hock injury, it is unwise to exercise the animal on an inclined<br />
treadmill or swim to maintain physical fitness as the injury may be exacerbated.<br />
Sacro-Iliac Sprain<br />
Although back injury only accounts for 1% of lameness in working horses, back<br />
problems are a common diagnosis for a restricted stride, lack of lateral flexion, tensing<br />
of the backline, tail swishing and dragging the rear toes under saddle. However,<br />
studies indicate that sprain of the sacro-iliac ligaments accounts for 50% or more of back<br />
related lameness, followed by bruising and injury to the vertical spinal processes on the<br />
spinal column under the backline muscles.<br />
Strain of the sacro-iliac ligaments that attach the spinal column (sacrum) to the pelvic<br />
girdle bone (ilium) can cause a noticeable ‘bump’ or raised area (commonly referred to as<br />
a “Hunter’s Bump”)on the midline just behind the pin bones or ‘os coxae’ (see<br />
illustration). When deep pressure is applied around the edges of the bump area just<br />
behind the high part of the rump with the fingers, horses with sacro-iliac strain will dip<br />
and attempt to ‘squat’ because of discomfort.
Sacro-iliac sprain is relatively common in horses carrying heavy weight riders, horses<br />
with hock or other hindlimb injuries, those working on hilly terrain or resulting from a<br />
fall, especially where the poll area shows discomfort on manipulation. Treatments for<br />
back problems are many and varied, and there is no single beneficial therapy. Studies<br />
indicate that chiropractic manipulation and acupuncture therapy only provide short term<br />
relief for sacro-iliac strain.
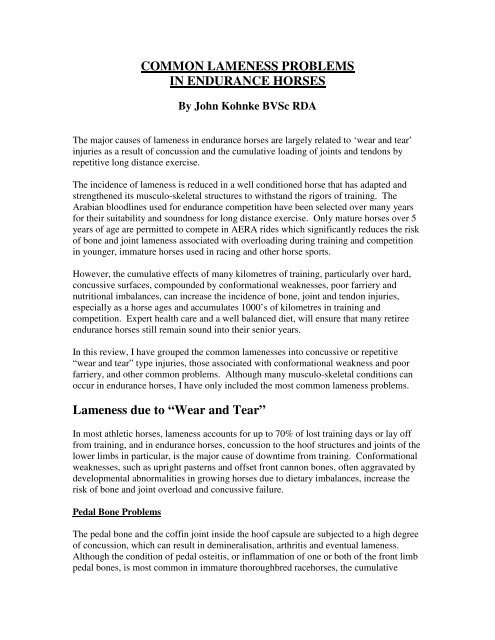
Poles 150mm<br />
(6”) diameter<br />
and 2.5 metres<br />
in length<br />
Repeat 4-5 times<br />
3 horse<br />
lengths apart<br />
Lateral movement pattern to strengthen sacro-iliac ligaments to<br />
assist recovery and reduce overall risk of sacro-iliac sprain.<br />
Where obvious pain and discomfort is present, an injection of long acting cortisone is<br />
recommended, followed by controlled exercise, designed to strengthen the sacro-iliac<br />
ligaments. <strong>In</strong>itial finger massage with a liniment over the sacro-iliac area for 3-5 minutes<br />
prior to exercise helps to relieve discomfort and muscle spasms. This is followed by<br />
walking the horse at an angle over 3-4 poles (150mm diameter) spaced 3 horse lengths<br />
apart, so that it has to lift its rear legs and move its pelvis diagonally to walk over the<br />
poles. This is repeated 4-5 times during the warm up before riding, turning in a crisscross<br />
manner over the poles to flex the sacro-iliac each way during the walk. Once<br />
mounted, walking and trotting in a ‘shoulder-in’ pattern each way over 200-300 metres<br />
will help to further strengthen the sacro-iliac ligaments over a 3-4 week period and, in<br />
most cases, will resolve this potentially chronic condition. It is possible that routine<br />
‘shoulder-in’ exercise each way at the walk and trot during warm-up prior to training,<br />
could reduce the incidence of this most common back injury by strengthening the sacroiliac<br />
ligaments and lower back structures. A blanket with magnets strategically located<br />
over the lower back may help assist blood perfusion within the sacro-iliac area when<br />
applied overnight and aid healing and chances of long term soundness.
Summary<br />
There are a number of common lameness conditions related to the ‘wear and tear’ on<br />
joints and other limb structures as a result of the concussive, loading and cumulative<br />
stress effects of long distance exercise. It is paramount for all horses being trained for an<br />
endurance career to have good limb conformation, a sound joints and limb structures in<br />
order to withstand long term training.<br />
A step-wise increase in distance and speed over a 10-12 week period to ‘leg up’ and<br />
adapt bones and joints in horses coming into training at the beginning of each season will<br />
help to reduce the incidence of many ‘wear and tear’ injuries as joint surfaces thicken,<br />
bone density increases and tendons strengthen by progressive loading. Regular hoof care<br />
is essential to minimise concussion to joints and maintenance of adequate heel height and<br />
short toe length, with correct hoof balance, will help encourage break over and reduce<br />
limb loading on the flexor tendons and suspensory ligaments.<br />
Sacro-iliac injury can be minimised by adopting a lateral movement pattern during warmup<br />
exercise on a daily basis.
An earlier fracture of this inside<br />
splint bone has caused a bony<br />
reaction and soft tissue swelling<br />
which will not affect long term<br />
soundness.




