

ANESTHESIA & ANALGESIA - IARS
ANESTHESIA & ANALGESIA - IARS
ANESTHESIA & ANALGESIA - IARS

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
ANESTH ANALG ABSTRACTS<br />
2004; 98; S-1–S-282<br />
S-86<br />
FACTORS AFFECTING THE CONCENTRATION OF CO IN<br />
THE BREATHING CIRCUIT AND THE CONCENTRATION<br />
OF ARTERIAL COHB DURING LOW-FLOW ISOFLURANE<br />
<strong>ANESTHESIA</strong> IN SMOKING AND NON-SMOKING<br />
SUBJECTS<br />
AUTHORS: M. Yamakage, S. Yoshida, S. Iwasaki, M. Mizuuchi,<br />
A. Namiki;<br />
AFFILIATION: Sapporo Medical University School of Medicine,<br />
Sapporo, Japan.<br />
INTRODUCTION: Smokers have a high incidence of postoperative<br />
respiratory complications, and smoking can also increase the<br />
concentration of carboxyhemoglobin (COHb) up to 5%~10%, leading<br />
to cardiac events during anesthesia. Carbon monoxide (CO) can be<br />
produced from degradation of isoflurane by soda lime, especially with<br />
dry soda lime or by the use of a low-flow anesthetic technique. Some<br />
carbon dioxide (CO2) absorbents that contain few or no strong bases<br />
have become available for clinical use. We investigated the<br />
concentration of CO in the anesthetic circuit and the concentration of<br />
arterial COHb during low-flow isoflurane anesthesia in smoking and<br />
non-smoking subjects using various kinds of CO2 absorbents with and<br />
without strong bases.<br />
METHODS: Sixty ASA physical status I or II adult patients were<br />
enrolled in this study. Thirty patients who were smoking up to the<br />
operating date and 30 patients who had never smoked were selected as<br />
smoker group and non-smoker group, respectively. Anesthesia was<br />
maintained with isoflurane and nitrous oxide (1 L/min)/oxygen (1 L/<br />
min). Ventilation was controlled to maintain end-tidal partial pressure<br />
of CO2 between 34 and 38 mmHg. The end-tidal isoflurane<br />
concentrations were adjusted to 1.0%. Each group (smoker or nonsmoker<br />
group) randomly divided into three groups according to the type<br />
of CO2 absorbent used. The CO2 absorbents used were Wakolime A,<br />
Dragersorb Free, and Amsorb. Gas samples for measurement of CO<br />
(Carbolyzer, mBA-2000) were obtained from the inspiratory limb of the<br />
circle system at 0, 1, 2, 3, and 4 hrs after exposure to isoflurane.<br />
Concentrations of arterial COHb were measured at the same time as the<br />
S-87<br />
8500 POET ® IQ -AN ACCURATE <strong>ANESTHESIA</strong> GAS<br />
MONITOR?<br />
AUTHORS: P. R. Lichtenthal, R. G. Loeb, S. E. Morgan;<br />
AFFILIATION: University of Arizona, Tucson, AZ.<br />
INTRODUCTION: While many companies sell respiratory gas<br />
monitors, most of these are OEM; only a few companies manufacture<br />
gas monitor benches. Criticare Systems, Inc., a longtime manufacturer<br />
of gas analyzer benches, recently released a new product, the 8500<br />
Poet ® IQ. This sidestream analyzer uses non-dispersive infrared (NDIR)<br />
technology to identify and measure CO2, N2O and five halogenated<br />
anesthetics, and a fast polarographic cell to measure O2 . The object of<br />
this study was to determine the accuracy and stability of this new<br />
respiratory gas analyzer as compared to an industry-standard analyzer<br />
(Datex AS3).<br />
METHODS: For a period of four weeks we conducted daily quality<br />
checks on both gas analyzers. Each was calibrated prior to the study by<br />
a factory-authorized technician . The analyzers were used clinically<br />
during the study period; they were located in the same operating room,<br />
and were used simultaneously for every case. Both analyzers were<br />
tested every morning for their ability to correctly analyze a series of 9<br />
precision gas mixtures (Scott Medical Products), each of which<br />
contained CO2. The analyzer sample lines were connected to computercontrolled<br />
solenoid valves that simulated respiratory rates of 10, 30, 60<br />
breaths per minute by switching the inflow path between test gas and<br />
room air every 3, 1, or 0.5 second, respectively. Stable end-tidal values<br />
were recorded from each analyzer’s display. Data from both analyzers<br />
for each of the 9 gases at 3 respiratory rates were collected. The average<br />
of the daily readings during the study (mean), day-to-day variation<br />
(SD), and the average error (bias) were then calculated.<br />
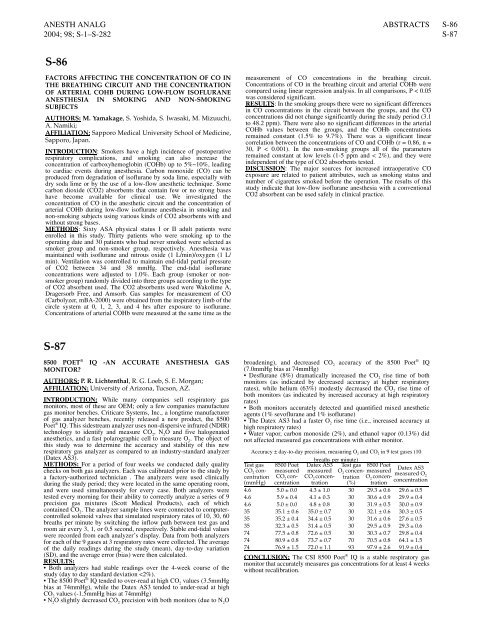
RESULTS:<br />
Both analyzers had stable readings over the 4-week course of the<br />
study (day to day standard deviation


