

Critical Appraisal of Clinical Prediction Rules That Aim to Optimize ...
Critical Appraisal of Clinical Prediction Rules That Aim to Optimize ...
Critical Appraisal of Clinical Prediction Rules That Aim to Optimize ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
effect <strong>of</strong> rule status (positive or negative)<br />
on response <strong>to</strong> treatment (manipulation<br />
versus placebo). 32 The 2<br />
validation RCTs both used longer,<br />
more clinically relevant maximum<br />
follow-up times <strong>of</strong> 12 weeks 32 and 6<br />
months. 26<br />
Discussion<br />
We found that all derivation-level<br />
CPRs used single-arm study designs<br />
<strong>to</strong> derive predic<strong>to</strong>rs, raising doubts<br />
about the veracity <strong>of</strong> current CPRs.<br />
In <strong>to</strong>tal, 15 CPRs <strong>to</strong> aid selection <strong>of</strong> a<br />
range <strong>of</strong> treatments for musculoskeletal<br />
conditions were found. However,<br />
only 1 CPR for selecting spinal<br />
manipulation for LBP 30 had reached<br />
the validation stage <strong>of</strong> CPR development,<br />
with the CPR predicting<br />
response <strong>to</strong> treatment in a narrow<br />
validation study but not treatment effects<br />
in a broad validation study. 26,28,32<br />
Although single-arm study designs<br />
can be a preliminary step in developing<br />
prediction rules by identifying<br />
potential candidate variables, they<br />
are not able <strong>to</strong> differentiate between<br />
predic<strong>to</strong>rs <strong>of</strong> response <strong>to</strong> treatment<br />
and predic<strong>to</strong>rs <strong>of</strong> outcome regardless<br />
<strong>of</strong> treatment. These studies do<br />
not include a control group, so they<br />
cannot provide information on treatment<br />
effects or on fac<strong>to</strong>rs that modify<br />
treatment effects. The predictive<br />
fac<strong>to</strong>rs identified in these studies,<br />
therefore, have a higher risk <strong>of</strong> being<br />
merely nonspecific predic<strong>to</strong>rs<br />
<strong>of</strong> outcome or prognostic fac<strong>to</strong>rs.<br />
Neither <strong>of</strong> the 2 previous systematic<br />
reviews 16,17 on this <strong>to</strong>pic discussed<br />
this issue <strong>of</strong> use <strong>of</strong> a singlearm<br />
trial design at the derivation<br />
level. One review stated that “most<br />
<strong>of</strong> the derivation studies were <strong>of</strong><br />
high quality,” 17(p40) a claim we<br />
would argue is potentially misleading,<br />
considering no derivation studies<br />
used a study design that allows<br />
specific identification <strong>of</strong> treatment<br />
effect modifiers.<br />
<strong>Clinical</strong> <strong>Prediction</strong> <strong>Rules</strong> for Musculoskeletal Conditions<br />
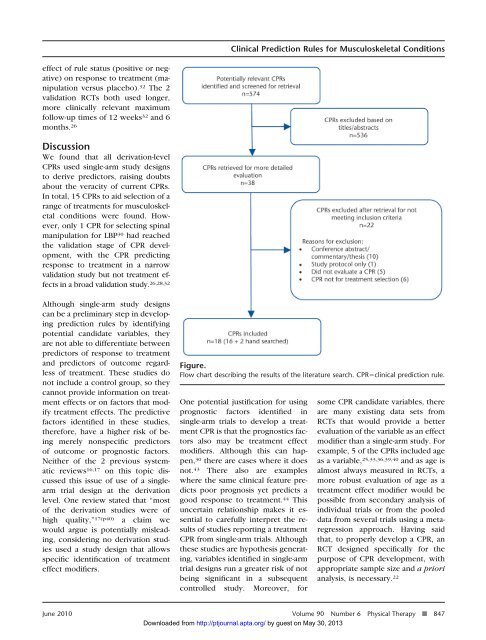
Figure.<br />
Flow chart describing the results <strong>of</strong> the literature search. CPRclinical prediction rule.<br />
One potential justification for using<br />
prognostic fac<strong>to</strong>rs identified in<br />
single-arm trials <strong>to</strong> develop a treatment<br />
CPR is that the prognostics fac<strong>to</strong>rs<br />
also may be treatment effect<br />
modifiers. Although this can happen,<br />
30 there are cases where it does<br />
not. 43 There also are examples<br />
where the same clinical feature predicts<br />
poor prognosis yet predicts a<br />
good response <strong>to</strong> treatment. 44 This<br />
uncertain relationship makes it essential<br />
<strong>to</strong> carefully interpret the results<br />
<strong>of</strong> studies reporting a treatment<br />
CPR from single-arm trials. Although<br />
these studies are hypothesis generating,<br />
variables identified in single-arm<br />
trial designs run a greater risk <strong>of</strong> not<br />
being significant in a subsequent<br />
controlled study. Moreover, for<br />
some CPR candidate variables, there<br />
are many existing data sets from<br />
RCTs that would provide a better<br />
evaluation <strong>of</strong> the variable as an effect<br />
modifier than a single-arm study. For<br />
example, 5 <strong>of</strong> the CPRs included age<br />
as a variable, 25,33,36,39,40 and as age is<br />
almost always measured in RCTs, a<br />
more robust evaluation <strong>of</strong> age as a<br />
treatment effect modifier would be<br />
possible from secondary analysis <strong>of</strong><br />
individual trials or from the pooled<br />
data from several trials using a metaregression<br />
approach. Having said<br />
that, <strong>to</strong> properly develop a CPR, an<br />
RCT designed specifically for the<br />
purpose <strong>of</strong> CPR development, with<br />
appropriate sample size and a priori<br />
analysis, is necessary. 22<br />
June 2010 Volume 90 Number 6 Physical Therapy f 847<br />
Downloaded from<br />
http://ptjournal.apta.org/ by guest on May 30, 2013













