2011 Summer Catalog - Gallaudet University
2011 Summer Catalog - Gallaudet University
2011 Summer Catalog - Gallaudet University

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
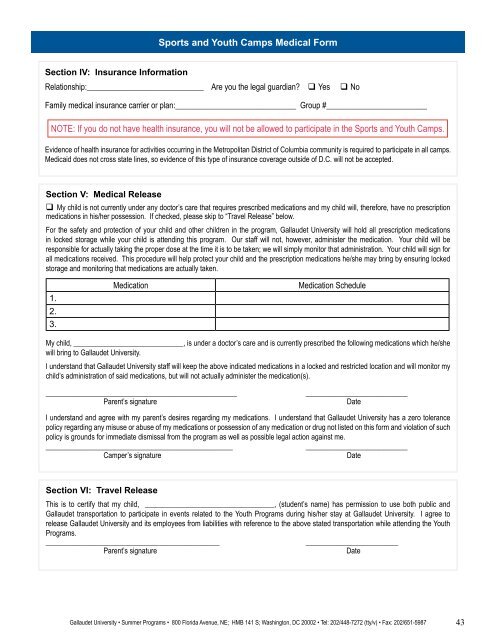
Section IV: Insurance Information<br />
Section V: Medical Release<br />
My child is not currently under any doctor’s care that requires prescribed medications and my child will, therefore, have no prescription<br />
medications in his/her possession. If checked, please skip to “Travel Release” below.<br />
For the safety and protection of your child and other children in the program, <strong>Gallaudet</strong> <strong>University</strong> will hold all prescription medications<br />
in locked storage while your child is attending this program. Our staff will not, however, administer the medication. Your child will be<br />
responsible for actually taking the proper dose at the time it is to be taken; we will simply monitor that administration. Your child will sign for<br />
all medications received. This procedure will help protect your child and the prescription medications he/she may bring by ensuring locked<br />
storage and monitoring that medications are actually taken.<br />
1.<br />
2.<br />
3.<br />
My child, ______________________________, is under a doctor’s care and is currently prescribed the following medications which he/she<br />
will bring to <strong>Gallaudet</strong> <strong>University</strong>.<br />
I understand that <strong>Gallaudet</strong> <strong>University</strong> staff will keep the above indicated medications in a locked and restricted location and will monitor my<br />
child’s administration of said medications, but will not actually administer the medication(s).<br />
_______________________________________________ _________________________<br />
Parent’s signature Date<br />
I understand and agree with my parent’s desires regarding my medications. I understand that <strong>Gallaudet</strong> <strong>University</strong> has a zero tolerance<br />
policy regarding any misuse or abuse of my medications or possession of any medication or drug not listed on this form and violation of such<br />
policy is grounds for immediate dismissal from the program as well as possible legal action against me.<br />
______________________________________________ _________________________<br />
Camper’s signature Date<br />
Section VI: Travel Release<br />
Sports and Youth Camps Medical Form<br />
Relationship:_____________________________ Are you the legal guardian? Yes No<br />
Family medical insurance carrier or plan:______________________________ Group #_________________________<br />
NOTE: If you do not have health insurance, you will not be allowed to participate in the Sports and Youth Camps.<br />
Evidence of health insurance for activities occurring in the Metropolitan District of Columbia community is required to participate in all camps.<br />
Medicaid does not cross state lines, so evidence of this type of insurance coverage outside of D.C. will not be accepted.<br />
Medication Medication Schedule<br />
This is to certify that my child, ___________________________________, (student’s name) has permission to use both public and<br />
<strong>Gallaudet</strong> transportation to participate in events related to the Youth Programs during his/her stay at <strong>Gallaudet</strong> <strong>University</strong>. I agree to<br />
release <strong>Gallaudet</strong> <strong>University</strong> and its employees from liabilities with reference to the above stated transportation while attending the Youth<br />
Programs.<br />
_______________________________________________ _________________________<br />
Parent’s signature Date<br />
<strong>Gallaudet</strong> <strong>University</strong> • <strong>Summer</strong> Programs • 800 Florida Avenue, NE; HMB 141 S; Washington, DC 20002 • Tel: 202/448-7272 (tty/v) • Fax: 202/651-5987<br />
43