department of health and human services centers for medicare ...
department of health and human services centers for medicare ...
department of health and human services centers for medicare ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
DEPARTMENT OF HEALTH AND HUMAN SERVICES<br />
PRINTED: 10/24/2011<br />
FORM APPROVED<br />
CENTERS FOR MEDICARE & MEDICAID SERVICES OMB NO. 0938-0391<br />
STATEMENT OF DEFICIENCIES<br />
AND PLAN OF CORRECTION<br />
(X1) PROVIDER/SUPPLIER/CLIA<br />
IDENTIFICATION NUMBER:<br />
(X2) MULTIPLE CONSTRUCTION<br />
A. BUILDING<br />
______________________<br />
B. WING _____________________________<br />
(X3) DATE SURVEY<br />
COMPLETED<br />
295037 03/04/2011<br />
NAME OF PROVIDER OR SUPPLIER<br />
HENDERSON HEALTHCARE CENTER<br />
STREET ADDRESS, CITY, STATE, ZIP CODE<br />
1180 E. LAKE MEAD DRIVE<br />
HENDERSON, NV 89015<br />
(X4) ID<br />
PREFIX<br />
TAG<br />
SUMMARY STATEMENT OF DEFICIENCIES<br />
(EACH DEFICIENCY MUST BE PRECEDED BY FULL<br />
REGULATORY OR LSC IDENTIFYING INFORMATION)<br />
ID<br />
PREFIX<br />
TAG<br />
PROVIDER'S PLAN OF CORRECTION<br />
(EACH CORRECTIVE ACTION SHOULD BE<br />
CROSS-REFERENCED TO THE APPROPRIATE<br />
DEFICIENCY)<br />
(X5)<br />
COMPLETION<br />
DATE<br />
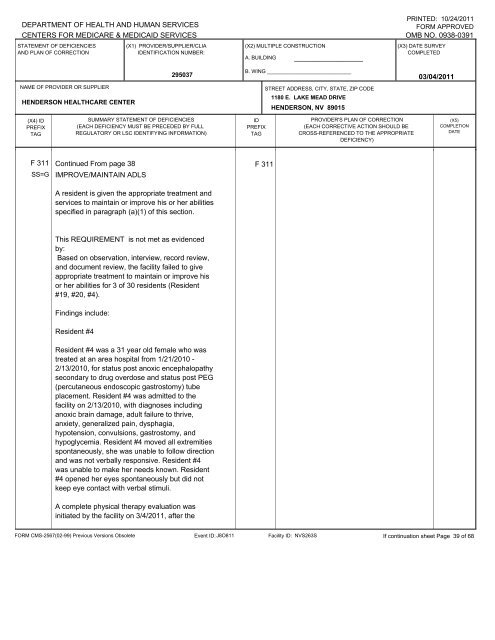
F 311 Continued From page 38 F 311<br />
SS=G<br />
IMPROVE/MAINTAIN ADLS<br />
A resident is given the appropriate treatment <strong>and</strong><br />
<strong>services</strong> to maintain or improve his or her abilities<br />
specified in paragraph (a)(1) <strong>of</strong> this section.<br />
This REQUIREMENT is not met as evidenced<br />
by:<br />
Based on observation, interview, record review,<br />
<strong>and</strong> document review, the facility failed to give<br />
appropriate treatment to maintain or improve his<br />
or her abilities <strong>for</strong> 3 <strong>of</strong> 30 residents (Resident<br />
#19, #20, #4).<br />
Findings include:<br />
Resident #4<br />
Resident #4 was a 31 year old female who was<br />
treated at an area hospital from 1/21/2010 -<br />
2/13/2010, <strong>for</strong> status post anoxic encephalopathy<br />
secondary to drug overdose <strong>and</strong> status post PEG<br />
(percutaneous endoscopic gastrostomy) tube<br />
placement. Resident #4 was admitted to the<br />
facility on 2/13/2010, with diagnoses including<br />
anoxic brain damage, adult failure to thrive,<br />
anxiety, generalized pain, dysphagia,<br />
hypotension, convulsions, gastrostomy, <strong>and</strong><br />
hypoglycemia. Resident #4 moved all extremities<br />
spontaneously, she was unable to follow direction<br />
<strong>and</strong> was not verbally responsive. Resident #4<br />
was unable to make her needs known. Resident<br />
#4 opened her eyes spontaneously but did not<br />
keep eye contact with verbal stimuli.<br />
A complete physical therapy evaluation was<br />
initiated by the facility on 3/4/2011, after the<br />
FORM CMS-2567(02-99) Previous Versions Obsolete<br />
Event ID: J8O811<br />
Facility ID: NVS263S If continuation sheet Page 39 <strong>of</strong> 68