Patients - Gundersen Health System
Patients - Gundersen Health System
Patients - Gundersen Health System

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Respecting Choices®<br />
Disease Specific-Patient Centered<br />
Advance Care Planning:<br />
A Program to Improve End-of-life<br />
Decision Making<br />
Linda Briggs, MS, MA, RN &<br />
Sandy Schellinger, RN, MSN, NP<br />
© Copyright 2009 All Rights Reserved – <strong>Gundersen</strong> Lutheran Medical Foundation, Inc.
Respecting Choices…An Advance<br />
Care Planning <strong>System</strong> That Works<br />
• In a 2008 study of all adult deaths in La Crosse<br />
county, the following results indicate the ongoing<br />
success of the Respecting Choices program<br />
– At death, 90% of adults have written advance directives<br />
– In 99% of cases, the AD is in the patient’s health record<br />
– In 67% of cases, a POLST form is completed<br />
– In virtually all cases, medical care was consistent with<br />
patient’s preferences<br />
• Hammes BJ, Rooney BL, Death and end-of-life planning in<br />
one Midwestern community…ten years later, AAHPM poster<br />
presentation 2009, Dallas, TX
The Problem: Planning for <strong>Patients</strong><br />
with Life-limiting Chronic Illness<br />
• More than 90 million Americans live with<br />
chronic illness<br />
• 7 out of 10 Americans will die from chronic<br />
illness<br />
• CHF, COPD, Cancer, CAD, Renal failure,<br />
PVD, Diabetes, Chronic liver failure,<br />
Dementia
End-stage Chronic Illness<br />
• Don’t fit the classification of “dying”<br />
• Incomplete prognostic information<br />
• Many have been “rescued”<br />
• Slow, progressive decline in function<br />
• Sudden complications without adequate<br />
expression of health care preferences<br />
• Difficult, confusing choices
Chronic Illness:<br />
Slow Decline, Periodic Crisis, Death<br />
<strong>Health</strong> Status<br />
Decline<br />
Crises<br />
Time<br />
Death<br />
Field & Cassel, 1997
Tracking the Care of <strong>Patients</strong> with<br />
Severe Chronic Illness<br />
The Dartmouth Atlas of <strong>Health</strong> Care 2008<br />
– Lead Author: John E. Wennberg<br />
– The Dartmouth Institute for <strong>Health</strong> Policy and<br />
Clinical Practice Center<br />
for <strong>Health</strong> Policy Research<br />
www.dartmouthatlas.org
Atlas Reports<br />
• Extensive unwarranted variation in quality<br />
of care delivered to Medicare recipients in<br />
last two years of life<br />
• Variations in spending are not due to<br />
prevalence of chronic illness<br />
• Variations in spending due to differences in<br />
“supply-sensitive” care
“Supply-Sensitive Care”<br />
• Services where the supply of specific<br />
resources has a major influence on<br />
utilization<br />
• Physician visits, hospitalizations, ICU stays,<br />
imaging services, among others
More is Not Better:<br />
High-spending Regions Report…<br />
• 32% higher per capita<br />
hospital beds<br />
• 65% more medical<br />
specialists<br />
• 26% fewer family<br />
practitioners<br />
• More hospital stays,<br />
MD visits<br />
• Mortality slightly<br />
higher after AMI, hip<br />
fracture<br />
• More likely to report<br />
poor communication<br />
with MD and<br />
inadequate continuity<br />
of care<br />
• No difference in<br />
patient satisfaction
Why Can More care Be Worse?<br />
• Hospitalizations are risky e.g., hospital<br />
acquired infections claim 100,000 deaths<br />
per year<br />
• Increase use of diagnostic tests to find<br />
problems that would not harm patient<br />
• Increase complexity of care, e.g., more<br />
MD’s, miscommunication, medical errors
Hospital<br />
Inpatient<br />
Reimbursements<br />
per decedent<br />
during last 2<br />
years of life<br />
Hospital days per<br />
decedent during<br />
last 2 years of<br />
life<br />
Reimburse per<br />
day during last 2<br />
years of life<br />
<strong>Gundersen</strong><br />
Lutheran<br />
18,359<br />
13.5<br />
1,355<br />
Franciscan Skemp<br />
19,194<br />
15.8<br />
1,210<br />
Meriter, Madison,<br />
WI.<br />
22,166<br />
18<br />
1,233<br />
St. Joseph's<br />
Marshfield<br />
23,249<br />
20.6<br />
1,126<br />
UW Hospitals and<br />
Clinics<br />
28,827<br />
19.7<br />
1,462<br />
Cleveland Clinic<br />
31,252<br />
23.9<br />
1,307<br />
St. Mary's Mayo<br />
31,816<br />
21.3<br />
1,497<br />
UCLA<br />
58,557<br />
31.3<br />
1,871<br />
US Average<br />
25,860<br />
23.6<br />
1,096
• “Concern about the possibility that some<br />
chronically ill and dying Americans might<br />
be receiving too much care: more than they<br />
and their families actually want or benefit<br />
from.”<br />
– Tracking the Care of <strong>Patients</strong> with Severe Chronic Illness,<br />
www.dartmouthatlas.org pg. 4
One Solution…<br />
Assist patients to make informed end-oflife<br />
treatment choices well before a medical<br />
crisis and develop plans to<br />
honor these choices
Respecting Choices®<br />
Disease Specific-Patient Centered<br />
ACP Intervention: Key Features<br />
‣ 1.5 hour interview with<br />
patient and healthcare<br />
agent in outpatient setting<br />
‣ First assesses dyad’s<br />
understanding of illness<br />
‣ Structured interview that<br />
integrates communication<br />
techniques
Respecting Choices®<br />
Disease-Specific, Patient Centered<br />
ACP Intervention: Key Features<br />
‣ Provides context for<br />
decision making<br />
through Statement of<br />
Treatment Preference<br />
form that assists in<br />
clarifying goals for lifesustaining<br />
treatment.
Respecting Choices®<br />
Disease-Specific, Patient Centered<br />
ACP Intervention: Key Features<br />
‣ Delivered by trained<br />
professional facilitator<br />
who has clinical<br />
experience, comfort<br />
level with issues, and<br />
good communication<br />
skills
DS-PCACP Interview Stages<br />
1. Assess illness beliefs, goals, values<br />
2. Explore experiences<br />
3. Explain purpose of ACP<br />
4. Clarify goals for life-sustaining treatment<br />
5. Summarize what was learned<br />
6. Develop follow-up plan
Expected Outcomes<br />
• Assessment of<br />
patient’s<br />
understanding of<br />
illness and<br />
complications<br />
• Clarification of goals,<br />
values, and beliefs<br />
• Understanding of<br />
treatment benefits and<br />
burdens<br />
• Documentation in<br />
medical record of<br />
patient goals for care<br />
in situations of worst<br />
outcomes<br />
• Strengthening role of<br />
healthcare agent<br />
• Identification of need<br />
for referrals for other<br />
services
DS-PCACP Research<br />
• AHRQ funded randomized control study<br />
• Pilot replication with cardiac surgical<br />
patients<br />
• Pilot replication with adolescents with<br />
HIV/AIDS
Patient-Centered Approach<br />
to Advance Care Planning in<br />
End-Stage Illness<br />
Karin T. Kirchhoff, PhD, RN, FAAN - Principal Investigator<br />
Bernard J. Hammes, PhD<br />
Linda A. Briggs, MS, MA, RN<br />
Karen A. Kehl, PhD, RN, ACHPN<br />
Funded by the Agency for <strong>Health</strong>care Research and Quality<br />
5R01HS013374-04<br />
04<br />
20
Method<br />
Design<br />
Randomized controlled study, stratified by patient<br />
disease (CHF vs. ESRD) and site (La Crosse vs. Madison)<br />
– Randomization by sealed envelope method<br />
Subjects<br />
<strong>Patients</strong> with end-stage CHF or ESRD patients and their<br />
surrogate health care decision makers from areas<br />
around La Crosse and Madison, WI<br />
• 312 dyads (patient & surrogate)<br />
– 133 La Crosse CHF<br />
– 98 La Crosse ESRD<br />
– 45 Madison CHF<br />
– 36 Madison ESRD
Method<br />
• Pairs complete baseline questionnaires on<br />
demographics, and functional status.<br />
• Pairs assigned to the usual care group receive<br />
standard advance directive care.<br />
• Pairs assigned to the intervention group receive, in<br />
addition to standard advance directive care, the<br />
intervention interview by trained interveners/facilitators.<br />
<strong>Patients</strong> in both groups<br />
complete:<br />
•Statement of Treatment<br />
Preferences<br />
•Decisional Conflict Scale<br />
•Knowledge of ACP<br />
Surrogates in both group<br />
complete:<br />
•Statement of Treatment<br />
Preferences for the Patient<br />
•Knowledge of ACP
Elements of PC-ACP Intervention<br />
• An in-depth structured interview with patient<br />
and surrogate in outpatient setting<br />
• Exploration of dyad's understanding,<br />
experiences, and goals for living well<br />
• Use of active communication techniques to<br />
engage dyad<br />
• Use of decision-aide tool (Statement of<br />
Treatment Preferences) to assist in clarifying<br />
goals for life-sustaining treatment<br />
• Delivered by trained facilitator
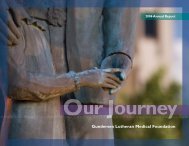
Results<br />
Congruence on Statement of Treatment Preferences<br />
100.00%<br />
90.00%<br />
80.00%<br />
70.00%<br />
Percent congruent<br />
60.00%<br />
50.00%<br />
40.00%<br />
30.00%<br />
20.00%<br />
10.00%<br />
0.00%<br />
1 2 3 4 Latitude<br />
Control 56.25% 54.10% 67.21% 57.14% 41.94%<br />
Intervention 88.57% 75.76% 86.57% 82.61% 82.61%<br />
Situation number
Conclusion<br />
• The increased agreement on the Statement of<br />
Treatment Preference form indicates that<br />
intervention surrogates are more prepared to<br />
make future decisions for their loved one<br />
• <strong>Patients</strong> and surrogates were highly satisfied<br />
with the quality of the communication (mean<br />
patient rating of 15.9 on a 1-171<br />
17 scale)<br />
• Care was consistent with documented<br />
preferences<br />
– Results submitted for publication
Cardiac Surgery<br />
<strong>Patients</strong> N=32<br />
Intervention group:<br />
Increase<br />
patient/healthcare<br />
agent congruence<br />
Decrease difficulty<br />
in making choices<br />
No difference in<br />
anxiety<br />
Song, 2005
DS-PCACP with Adolescents with<br />
HIV/AIDS<br />
• Medically stable adolescents (14-21 years<br />
of age) and parent/guardian<br />
• N=38 dyads, 92% Black<br />
• Significant increase in understanding of<br />
patient goals over control group<br />
• Intervention patients rated the quality of<br />
communication very good to excellent<br />
• Lyon, 2009, Pediatrics 123(2)
Goals of Advance Care Planning<br />
• Ensure clinical care consistent with wishes<br />
• Improve decision-making process<br />
– Facilitate shared decision-making among<br />
patient, physician and proxy<br />
– Allow proxy to speak on behalf of patient<br />
– Respond with flexibility to unforeseen clinical<br />
situations<br />
– Provide education regarding issues
A Means to a Better End…<br />
• Improve patient outcomes<br />
– Improve patient well-being by reducing over<br />
treatment and under treatment<br />
– Reduce patient concern’s regarding burden on<br />
family and significant others<br />
• Teno,1994
Allina Hospitals and Clinics<br />
• Integrated system with a patient<br />
centered care model<br />
• One Electronic Medical record<br />
• 11 hospitals in MN and WI<br />
• 85 Primary Clinics<br />
• 4 th largest medical group in the US<br />
• > 120,000 hospital admissions<br />
• 4.5 Million Clinic visits<br />
• Home and Community Services 28<br />
County Service Area (Home Care,<br />
Hospice, Palliative Care, Care<br />
Navigation, Senior Care Transitions,<br />
Care Management, DME)<br />
• 110,000 Home Care and Hospice visits<br />
• 15 Community Pharmacies<br />
• Medical Transportation<br />
• Medical Laboratories
Patient and Family Centered Care Goal:<br />
Aim: All patient’s and families goals, wishes, values and health care preferences will be<br />
honored at any point of care at any time and care setting.
Chronic Advancing Disease:<br />
Continuum of Care Model<br />
DISEASE SPECIFIC ADVANCE CARE PLANNING<br />
Disease modifying therapies to abort illness or treat for possible cure<br />
Presentation / Exacerbation of chronic progressive illness<br />
Hospice<br />
Benefit<br />
Bereavement<br />
Care<br />
Palliative Care<br />
Diagnosis<br />
of illness<br />
Therapies to relieve suffering<br />
and/or improve quality of life<br />
Home Care<br />
Palliative Care<br />
6m Death<br />
-----------------<br />
-----------------<br />
-----------------<br />
Hospice Care
END OF LIFE – patients and families<br />
most likely to die in the next 6-12<br />
months. Ongoing discussions on a<br />
regular basis by care team, i.e. PCP,<br />
Hospice , Palliative Care, hospital<br />
staff around goals, values, and<br />
health care wishes as their health<br />
progresses. As a result the patient<br />
may complete a POLST form and<br />
update current HCD.<br />
End<br />
of Life<br />
Disease Specific<br />
Patient Centered<br />
Advance Care<br />
Planning<br />
(DS-PCACP)<br />
Basic Advance Care<br />
Planning<br />
Goal: Allina Advance Care<br />
Planning Standard<br />
across the care continuum<br />
2009-2013<br />
DSPCACP - All patients and families<br />
with chronic advancing illness most<br />
likely to die in the next several years<br />
have assistance in intentionally<br />
discussing goals, values and health<br />
care wishes specific to their own<br />
individual situation by a trained ACP<br />
facilitator. Outcome: Documentation of<br />
ACP session in medical record;<br />
completed documents, i.e. HCD,<br />
statement of treatment preferences,<br />
POLST.<br />
BASIC ACP - All <strong>Patients</strong> 50 and older are encouraged to<br />
identify a POAHC, discuss and clarify health care wishes,<br />
goals, and values for a sudden health event where they may<br />
be unable to speak for themselves. A HCD may be completed<br />
as a result of basic ACP.
Where to Begin in Such a large<br />
<strong>Health</strong> <strong>System</strong>?<br />
2008 <strong>System</strong> Goal: Improving Care of Heart Failure<br />
across the Care Continuum demonstrated by<br />
reducing the number of unplanned hospital<br />
readmissions by 10%<br />
• ACP Pilot DSPCACP in Heart Failure Population<br />
– 2008 ACP Goal: complete 250 DSPCACP session with<br />
heart failure patients and their surrogate.<br />
• 268 sessions completed by 10 trained facilitators (palliative<br />
care clinicians)
100<br />
ACP Treatement Preferences<br />
DSPCACP<br />
Sessions<br />
80<br />
60<br />
40<br />
20<br />
0<br />
L Surv /H T m t<br />
H Surv /L F x n<br />
H Surv/L Cog<br />
Code Status<br />
Comf ort Care<br />
Not Sure<br />
Not Sure<br />
Full Treatment<br />
Comf ort Care<br />
Summary<br />
of<br />
Treatment<br />
Choices<br />
What do you understand about your condition?<br />
What care might you want under various circumstances? e.g.:<br />
Low probability of survival, but with good function,<br />
High likelihood of survival with functional impairment,<br />
High likelihood of survival with cognitive impairment.<br />
What do you know about CPR? Has your doctor talked about how it might apply in your case?
Honoring Patient Wishes Current State within Allina<br />
1/1/08 - 10/08 Heart Failure <strong>Patients</strong>:<br />
Availability of HCD in EMR<br />
Source Ace Report and ACP Audit<br />
90<br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
ACP n=220<br />
89%<br />
83%<br />
40%<br />
No ACP n=6,621<br />
16%<br />
HCD (%)<br />
HCD In chart (%)
40.0%<br />
35.0%<br />
30.0%<br />
25.0%<br />
23.0%<br />
20.4%<br />
20.0% 18.8%18.9% 19.3%<br />
Allina Hospitals and Clinics<br />
Percent HF (Pdx) Unique <strong>Patients</strong> That Had One or More Readmissions Within 30 Days<br />
Median Readmit Rate<br />
17.1%<br />
22.7%<br />
18.9%<br />
20.1%<br />
22.3%<br />
23.8%<br />
22.5%<br />
19.6%<br />
21.1%<br />
24.9%<br />
21.8%<br />
21.2%<br />
19.7%19.6%<br />
17.9%<br />
24.1%<br />
16.5% 17.0% 20.4%<br />
25.1%<br />
24.4%<br />
16.8%<br />
20.0% 19.6%19.8%<br />
17.6%<br />
20.9%<br />
19.4%<br />
19.7%<br />
19.8%<br />
HF<br />
Readmission<br />
Rate Allina<br />
<strong>Health</strong> <strong>System</strong><br />
vs. with ACP<br />
20%<br />
15.0%<br />
2008 Goal = 18.12%<br />
10.0%<br />
% Rehospitalization of ACP pts 1/1/08-10/08<br />
Source ACP Chart Audit<br />
5.0%<br />
0.0%<br />
2006 1<br />
2006 3<br />
2006 5<br />
2006 7<br />
2006 9<br />
2006 11<br />
2007 1<br />
2007 3<br />
2007 5<br />
2007 7<br />
20<br />
2007 9<br />
2007 11<br />
2008 1<br />
15% 15%<br />
2008 3<br />
2008 5<br />
2008 7<br />
2008 9<br />
2008 11<br />
19%<br />
15<br />
10<br />
5<br />
0<br />
30 days 60 days 90 days<br />
3
Outcomes of ACP in <strong>Patients</strong> Dying of Heart Failure, 2008<br />
100<br />
90<br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
No<br />
ACP<br />
ACP<br />
No<br />
ACP<br />
ACP<br />
No<br />
ACP<br />
ACP<br />
Deaths (%) HCD in chart Hospice LOS
Allina Implementation Strategies<br />
• Engaged leadership and key stakeholders to create consistent message.<br />
• Culture: ACP needs to be a normal part of conversation for all patients.<br />
• Started Pilot with a specific population of patients vs. basic ACP<br />
– Easier to “sell” ACP because these patients really needed ACP.<br />
• Identified clear outcomes and measures.<br />
• Small test of changes to gain buy in and adjust processes and<br />
workflow.<br />
• Set up <strong>System</strong>s for success<br />
– i.e. ACP on order sets for heart failure patients.<br />
• Train engaged and interested staff (Palliative Care RN’s and SW’s, RN<br />
Care Managers in the Clinic)<br />
– Some staff were required to get trained as ACP is part of their role but<br />
may not be the right “fit” to facilitate ACP discussions
Allina Barriers/Challenges<br />
• Lack of centralized ACP documentation.<br />
• Large <strong>Health</strong> <strong>System</strong><br />
• Primary Care Physicians<br />
• Implemented DSPCACP before Basic<br />
– Most patients did not have basic ACP before session<br />
which made the actual session longer and complex<br />
• Palliative Care Program Director managing ACP<br />
program<br />
– Pros and Cons<br />
• Economics – ACP role does not pay for itself.
Honoring wishes at time of death:<br />
68 year old male with CHF, COPD,<br />
Respiratory Failure<br />
• ACP Session: 6/23/08; Understood his condition as having heart disease and diabetes.<br />
Also understands that he is at risk for kidney failure. His disease burden included<br />
dizziness, fear of falling, swelling in his legs, shortness of breath and dependence on<br />
oxygen. Quality of life dramatically changed by his limited declining status. Hope for<br />
improvement of sores on his legs but knows he cannot cure his lung disease. Statement<br />
of Treatment preferences – full code; also, if he suffered a serious complication with low<br />
probability of survival or he survived a serious event and had significant cognitive or<br />
functional deficits he would want to stop all efforts to keep him alive and focus on<br />
comfort. ACP note and HCD documents were in the EMR.<br />
• Date of death: 7/27/08; EMR Death D/C summary and course of care during<br />
hospitalization – In ICU on BiPAP for respiratory failure. Deterioration in mental status.<br />
• Per MD note in summary, “In Accordance with his well stated previous wishes and<br />
wishes of his family, aggressive medical treatments were discontinued and the<br />
patient was made comfort cares only. The patient was kept comfortable with PRN<br />
morphine. The patient died peacefully on 7/27 with family present.”
Improving Families confidence and<br />
reducing burden of decision making<br />
• 64 y/o married male with end-stage ischemic cardio-myopathy, s/p aortic<br />
valve replacement. Waiting for heart transplant. ACP Session completed<br />
3/26/08: full code try CPR for 3-4 minutes if it does not work let me go. If<br />
seriously ill and was cognitively or functionally impaired” just let me go”<br />
• 5/27/08 hospitalized for worsening heart failure. 6/8/08 received heart<br />
transplant which was uneventful. Re-intubated 8 days after transplant.<br />
Went downhill; subsequent infections and multi-system organ failure.<br />
• Per MD D/C summary, “ The family has been extremely supportive<br />
throughout this ordeal and the decision was made on Mr. H’s wishes not to<br />
be kept alive on life-support.” Died 7/7/08<br />
• Decision Making: Per hospital staff and spouse, there were three times<br />
during the last few weeks of life where the spouse needed to make<br />
treatment decisions. Each time she pulled out the documents and<br />
referenced the ACP session discussions to help her make the decision.
Allina ACP goals<br />
• 2009<br />
– 750 patients (500 heart failure and 250 other chronic illness) will receive<br />
ACP session resulting in completed and documented advance care plan.<br />
– 250 Allina Home and Community Services – Home Care patients will have<br />
a documented basic advance care plan<br />
• 2010<br />
– 5000 patients and employees of the Allina <strong>Health</strong> <strong>System</strong> will have a<br />
documented advance care plan.<br />
• 3000 Disease Specific ACP session will be completed for patients with<br />
chronic advanced illness.<br />
• 1500 basic ACP documented for Allina patients age greater than 50<br />
years old.<br />
• 1000 Allina employees will have a basic ACP documented.<br />
• 400 POLST forms completed for patients in hospice, LTC, AL, TCU<br />
• 2013<br />
– All patients greater than age 50 years old will have a documented ACP in<br />
their medical record.
Summary:<br />
Advance Care Planning in Allina<br />
Basic and Disease<br />
Specific Advance Care<br />
Planning<br />
A Process<br />
<strong>Health</strong> Care Directive /<br />
Living Will<br />
POLST<br />
A Patientdirected<br />
Document<br />
A Physician’s<br />
Order
Next Steps/Questions<br />
• When does Advance Care Planning become<br />
standard/best practice?<br />
• Are there other opportunities to research use of<br />
ACP for patients other cultures and diseases.<br />
• ACP reimbursement:<br />
– Government and Third Party Payers payment for ACP<br />
• Minnesota U Care reimbursing for ACP as of 7/1/09