APRN - Department of Nursing
APRN - Department of Nursing
APRN - Department of Nursing

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
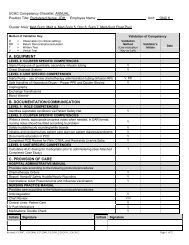
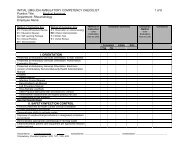
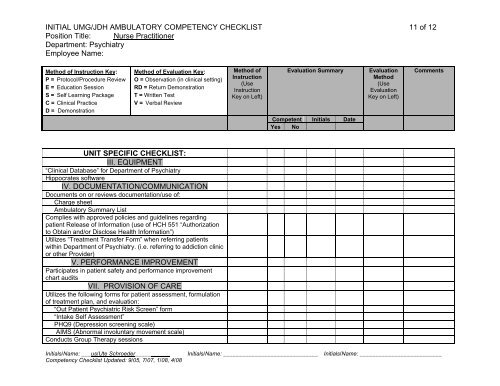
INITIAL UMG/JDH AMBULATORY COMPETENCY CHECKLIST 11 <strong>of</strong> 12<br />
Position Title: Nurse Practitioner<br />
<strong>Department</strong>: Psychiatry<br />
Employee Name:<br />
Method <strong>of</strong> Instruction Key:<br />
P = Protocol/Procedure Review<br />
E = Education Session<br />
S = Self Learning Package<br />
C = Clinical Practice<br />
D = Demonstration<br />
Method <strong>of</strong> Evaluation Key:<br />
O = Observation (in clinical setting)<br />
RD = Return Demonstration<br />
T = Written Test<br />
V = Verbal Review<br />
Method <strong>of</strong><br />
Instruction<br />
(Use<br />
Instruction<br />
Key on Left)<br />
Evaluation Summary<br />
Evaluation<br />
Method<br />
(Use<br />
Evaluation<br />
Key on Left)<br />
Comments<br />
Competent Initials Date<br />
Yes No<br />
UNIT SPECIFIC CHECKLIST:<br />
III. EQUIPMENT<br />
“Clinical Database” for <strong>Department</strong> <strong>of</strong> Psychiatry<br />
Hippocrates s<strong>of</strong>tware<br />
IV. DOCUMENTATION/COMMUNICATION<br />
Documents on or reviews documentation/use <strong>of</strong>:<br />
Charge sheet<br />
Ambulatory Summary List<br />
Complies with approved policies and guidelines regarding<br />
patient Release <strong>of</strong> Information (use <strong>of</strong> HCH 551 “Authorization<br />
to Obtain and/or Disclose Health Information”)<br />
Utilizes “Treatment Transfer Form” when referring patients<br />
within <strong>Department</strong> <strong>of</strong> Psychiatry. (i.e. referring to addiction clinic<br />
or other Provider)<br />
V. PERFORMANCE IMPROVEMENT<br />
Participates in patient safety and performance improvement<br />
chart audits<br />
VII. PROVISION OF CARE<br />
Utilizes the following forms for patient assessment, formulation<br />
<strong>of</strong> treatment plan, and evaluation:<br />
“Out Patient Psychiatric Risk Screen” form<br />
“Intake Self Assessment”<br />
PHQ9 (Depression screening scale)<br />
AIMS (Abnormal involuntary movement scale)<br />
Conducts Group Therapy sessions<br />
Initials/Name: ___us/Ute Schroeder___________ Initials/Name: ______________________________ Initials/Name: __________________________<br />
Competency Checklist Updated: 9/05, 7/07, 1/08, 4/08