Kingsbridge Private Hospital, Belfast - 20 January 2012
Kingsbridge Private Hospital, Belfast - 20 January 2012
Kingsbridge Private Hospital, Belfast - 20 January 2012

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
33333333333333333333333333333333<br />
RQIA<br />
Infection Prevention/Hygiene<br />
Announced inspection<br />
<strong>Kingsbridge</strong> <strong>Private</strong> <strong>Hospital</strong><br />
<strong>20</strong> <strong>January</strong> <strong>20</strong>12
Contents<br />
1.0 Inspection Summary 1<br />
2.0 Background Information to the Inspection Process 5<br />
3.0 Inspections 6<br />
4.0 Unannounced Inspection Process 7<br />
4.1 Onsite Inspection 7<br />
4.2 Feedback and Report of the Findings 7<br />
5.0 Audit Tool 8<br />
6.0 Environment 10<br />
6.1 Cleaning 10<br />
6.2 Clutter 11<br />
6.3 Maintenance and Repair 11<br />
6.4 Fixture and Fittings 11<br />
6.5 Information 11<br />
7.0 Patient Linen 13<br />
7.1 Management of Linen 13<br />
8.0 Waste and Sharps 14<br />
8.1 Waste 14<br />
8.2 Sharps 14<br />
9.0 Patient Equipment 16<br />
10.0 Hygiene Factors 17<br />
11.0 Hygiene Practice 19<br />
12.0 Endoscopy Suite 21<br />
12.1 Endoscopy Suite Environment 23<br />
12.2 Specialist Patient Equipment 23<br />
12.3 Policies and Procedures 23<br />
13.0 Key Personnel and Information 24<br />
14.0 Summary of Recommendations 25<br />
15.0 RQIA Hygiene Team Escalation Policy Flowchart 27<br />
16.0 Action Plan 28
1.0 Inspection Summary<br />
A joint inspection of endoscopy units in regulated independent<br />
healthcare facilities was conducted by members of RQIA infection<br />
prevention/hygiene Team (IPHT), estates, and HEIG (Health Estates<br />
Investment Group) inspectors from the DHSSPS.<br />
The purpose of the announced inspection to <strong>Kingsbridge</strong> <strong>Private</strong><br />
<strong>Hospital</strong> on the 21<strong>January</strong> <strong>20</strong>11 was to provide assurance that facilities<br />
and practices specific to endoscopic procedures within the clinic<br />
complied with current standards.<br />
The clinic was assessed against the Regional Healthcare Hygiene and<br />
Cleanliness standards, with an additional section developed specifically<br />
for endoscopy suites. Inspectors from HEIG also carried out an<br />
inspection using the Flexible Endoscope audit tool produced by<br />
DHSSPS Health Estates and Investment Group (HEIG) the following<br />
area was inspected:<br />
• Specialist Area - Endoscopy Suite/Theatre<br />
The hospital was originally registered <strong>20</strong>06, it was re-registered as the<br />
Kings Bridge <strong>Private</strong> <strong>Hospital</strong> in November <strong>20</strong>11, it is located in South<br />
<strong>Belfast</strong> and offers a range of both inpatient and out patient procedures.<br />
The endoscopy unit, which operates on an outpatient basis, is a<br />
separate area within the hospital. The endoscopy suite is on the<br />
second floor and is accessed via the main reception by lift or stairs.<br />
There is a small reception area with a consulting room (under<br />
construction), two changing rooms with en-suite, a theatre, clean utility<br />
room and two linked dirty utility rooms.<br />
Inspection Outcomes<br />
The results of the inspection showed an overall compliance level.<br />
However the structure and layout of the endoscopy decontamination<br />
room do not comply with the required standards as evidenced in the<br />
minimally compliant score achieved in this section of the audit tool.<br />
Inspectors also noted that improvement was required in some<br />
associated endoscopic practices.<br />
Observation of staff practice indicated overall compliance with hygiene<br />
and infection prevention and control practices. However more work is<br />
required to ensure effective hand hygiene is carried out by all staff.<br />
The safe management and disposal of waste also requires attention,<br />
and the clinic needs to review the use and supply of personal<br />
protective equipment (PPE).<br />
The inspection resulted in 22 recommendations for <strong>Kingsbridge</strong> <strong>Private</strong><br />
<strong>Hospital</strong>, a full list of recommendations is listed in Section 14. The<br />
1
eport and recommendations will be forwarded to the relevant inspector<br />
for performance management under the following regulations and<br />
standards:<br />
• The HPSS (Quality, Improvement and Regulation) (Northern<br />
Ireland) Order <strong>20</strong>03<br />
• The Independent Health Care Regulations (Northern Ireland)<br />
<strong>20</strong>05<br />
• The Department of Health, Social Services and Public Safety's<br />
(DHSSPS) draft Independent Health Care Minimum Standards<br />
for <strong>Hospital</strong>s and Clinics March <strong>20</strong>05<br />
• The Department of Health, Social Services and Public Safety's<br />
(DHSSPS) Health Estates Investment Group, Flexible<br />
Endoscope Decontamination Audit Tool, <strong>January</strong> <strong>20</strong>10<br />
A report from HEIG inspectors on their findings has been provided in<br />
the format of “key audit findings” and “points of concern”. A copy has<br />
been forwarded to the clinic requesting an action plan to address the<br />
deficiencies identified. The clinic was also asked to provide RQIA with<br />
a position statement regarding their proposal for future service delivery<br />
i.e. upgrading of the existing on-site reprocessing facilities or<br />
outsourcing of endoscope reprocessing.<br />
Notable Practice<br />
The inspection identified the following areas of notable practice:<br />
• Staff displayed a positive attitude to inspection and a<br />
willingness to learn and improve practices.<br />
The RQIA inspection team would like to thank the staff at the<br />
<strong>Kingsbridge</strong> <strong>Hospital</strong> for their assistance during the inspection.<br />
The following tables give an overview of compliance scores noted in<br />
areas inspected by RQIA:<br />
Table 1 summarises the overall compliance levels achieved.<br />
Tables 2-7 summarise the individual tables for sections two to seven of<br />
the audit tool as this assists organisation to target areas that require<br />
more specific attention.<br />
2
Table 1<br />
Areas Inspected<br />
Environment 84<br />
Patient Linen 91<br />
Waste 86<br />
Sharps 67<br />
General Patient<br />
Equipment<br />
87<br />
Hygiene Factors 88<br />
Hygiene Practices 86<br />
Endoscopy Suite 85<br />
Average Score 84<br />
Table 2<br />
General Environment<br />
Reception 98<br />
Corridors, stairs lift 83<br />
Public toilets 83<br />
Ward/department -<br />
general (communal)<br />
85<br />
Toilet 82<br />
Domestic store 78<br />
General information 77<br />
Average Score 84<br />
Table 3<br />
Patient Linen<br />
Storage of clean linen 90<br />
Storage of used linen 91<br />
Laundry facilities<br />
N/A<br />
Average Score 91<br />
Table 4<br />
Waste and Sharps<br />
Handling, segregation,<br />
storage, waste<br />
Availability, use, storage<br />
of sharps<br />
86<br />
67<br />
Compliant:<br />
85% or above<br />
Partial Compliance: 76% to 84%<br />
Minimal Compliance: 75% or below<br />
3
Table 5<br />
Patient Equipment<br />
Patient equipment 87<br />
Table 6<br />
Hygiene Factors<br />
Availability and<br />
cleanliness of wash hand 96<br />
basin and consumables<br />
Availability of alcohol rub 92<br />
Availability of PPE 82<br />
Materials and equipment<br />
for cleaning<br />
81<br />
Average Score 88<br />
Table 7<br />
Hygiene Practices<br />
Effective hand hygiene<br />
procedures<br />
67<br />
Safe handling and<br />
disposal of sharps<br />
100<br />
Effective use of PPE 83<br />
Correct use of isolation N/A<br />
Effective cleaning of ward 82<br />
Staff uniform and work<br />
wear<br />
97<br />
Average Score 86<br />
Table 8<br />
Endoscopy Suite<br />
Scrub Room<br />
N/A<br />
Endoscopy Theatre 97<br />
Endoscopy<br />
60<br />
decontamination room<br />
Specialist<br />
90<br />
Equipment/practices<br />
Policies and Procedures 93<br />
Average Score 85<br />
Compliant:<br />
85% or above<br />
Partial Compliance: 76% to 84%<br />
Minimal Compliance: 75% or below<br />
4
2.0 Background Information to the Inspection Process<br />
RQIA’s infection prevention and hygiene team was established to<br />
undertake a rolling programme of unannounced inspections of acute<br />
hospitals. The Department of Health Social Service and Public Safety<br />
(DHSSPS) commitment to a programme of hygiene inspections was<br />
reaffirmed through the launch in <strong>20</strong>10 of the revised and updated<br />
version of 'Changing the Culture' the strategic regional action plan for<br />
the prevention and control of healthcare-associated infections (HCAIs)<br />
in Northern Ireland.<br />
The aims of the inspection process are:<br />
• to provide public assurance and to promote public trust and<br />
confidence<br />
• to contribute to the prevention and control of HCAI<br />
• to contribute to improvement in hygiene, cleanliness and infection<br />
prevention and control across health and social care in Northern<br />
Ireland<br />
In keeping with the aims of the RQIA, the team will adopt an open and<br />
transparent method for inspection, using standardised processes and<br />
documentation.<br />
5
3.0 Inspections<br />
The DHSSPS has devised Regional Healthcare Hygiene and<br />
Cleanliness standards. RQIA has revised its inspection processes to<br />
support the publication of the standards which were compiled by a<br />
regional steering group in consultation with service providers.<br />
The inspections will be undertaken in accordance with the four core<br />
activities outlined in the RQIA Corporate Strategy, these include:<br />
• Improving care: we encourage and promote improvements in the<br />
safety and quality of services through the regulation and review of<br />
health and social care<br />
• Informing the population: we publicly report on the safety,<br />
quality and availability of health and social care<br />
• Safeguarding rights: we act to protect the rights of all people<br />
using health and social care services<br />
• Influencing policy: we influence policy and standards in health<br />
and social care<br />
6
4.0 Announced Inspection Process<br />
The hospital received advanced notice of the onsite inspection.<br />
4.1 Onsite Inspection<br />
The inspection team was made up of two inspectors, from RQIA’s<br />
infection prevention/hygiene team, one inspector from RQIA’s estates<br />
team and two inspectors from the DHSSPS Health Estates Investment<br />
Group (HEIG) inspection team. Membership of the inspection team is<br />
outlined in Section 13.<br />
The inspection process involves observation, discussion with staff, and<br />
review of some ward documentation.<br />
4.2 Feedback and Report of the Findings<br />
The process concludes with a feedback of key findings to<br />
organisational representatives and includes examples of notable<br />
practice identified during the inspection. The details of organisational<br />
representatives attending the feedback session is outlined in Section<br />
13.<br />
The RQIA team responsible for the facility is forwarded a copy of the<br />
draft report. The responsible inspector will review the report and<br />
recommendations and devise a Quality Improvement Plan. The draft<br />
report containing the Quality Improvement Plan of the inspection is<br />
forwarded to the organisation for agreement and factual accuracy<br />
checking and returned within two weeks. The Quality Improvement<br />
Plan will be subject to performance management by the inspector<br />
responsible for the facility.<br />
The infection prevention/hygiene team escalation process will be<br />
followed if inspectors/reviewers identify any serious concerns during<br />
the inspection (Section 15).<br />
A number of documents have been developed to support and explain<br />
the inspection process. This information is currently available on<br />
request and will be available in due course on the RQIA website.<br />
7
5.0 Audit Tool<br />
The audit tool used for the inspection is based on the Regional<br />
Healthcare Hygiene and Cleanliness standards. The standards<br />
incorporate the critical areas which were identified through a review of<br />
existing standards, guidance and audit tools (Appendix 2 of Regional<br />
Healthcare Hygiene and Cleanliness standards). The audit tool follows<br />
the format of the Regional Healthcare Hygiene and Cleanliness<br />
Standards and comprises of the following sections.<br />
1. Organisational Systems and Governance: policies and<br />
procedures in relation to key hygiene and cleanliness issues;<br />
communication of policies and procedures; roles and<br />
responsibilities for hygiene and cleanliness issues; internal<br />
monitoring arrangements; arrangements to address issues<br />
identified during internal monitoring; communication of internal<br />
monitoring results to staff<br />
2. General Environment: cleanliness and state of repair of public<br />
areas; cleanliness and state of repair of ward/department<br />
infrastructure; cleanliness and state of repair of patient bed area;<br />
cleanliness and state of repair of toilets, bathrooms and<br />
washrooms; cleanliness and state of repair of ward/department<br />
facilities; availability and cleanliness of isolation facilities;<br />
provision of information for staff, patients and visitors<br />
3. Patient Linen: storage of clean linen; handling and storage of<br />
used linen; ward/department laundry facilities<br />
4. Waste and Sharps: waste handling; availability and storage of<br />
sharps containers<br />
5. Patient Equipment: cleanliness and state of repair of general<br />
patient equipment<br />
6. Hygiene Factors: hand wash facilities; alcohol hand rub;<br />
availability of personal protective equipment (PPE); availability of<br />
cleaning equipment and materials.<br />
7. Hygiene Practices: hand hygiene procedures; handling and<br />
disposal of sharps; use of PPE; use of isolation facilities and<br />
implementation of infection control procedures; cleaning of<br />
ward/department; staff uniform and work wear<br />
8. Endoscopy Suite: anaesthetic room, scrub room, endoscopy<br />
theatre/room, endoscopy decontamination room/area, specialist<br />
equipment and policies/procedures.<br />
8
Level of Compliance<br />
Percentage scores can be allocated a level of compliance using the<br />
compliance categories below. The categories are allocated as follows:<br />
Compliant<br />
85% or above<br />
Partial compliance 76 to 84%<br />
Minimal compliance 75% or below<br />
Each section within the audit tool will receive an individual and an<br />
overall score, to identify areas of partial or minimal compliance to<br />
ensure that the appropriate action is taken.<br />
9
6.0 Environment<br />
STANDARD 2.0<br />
GENERAL ENVIRONMENT<br />
Cleanliness and state of repair of public areas; cleanliness and<br />
state of repair of ward/department infrastructure; cleanliness and<br />
state of repair of patient bed area; cleanliness and state of repair<br />
of toilets, bathrooms and washrooms; cleanliness and state of<br />
repair of ward/department facilities; availability and cleanliness of<br />
isolation facilities; provision of information for staff, patients and<br />
visitors.<br />
General Environment<br />
Reception 98<br />
Corridors, stairs lift 83<br />
Public toilets 83<br />
Ward/department -<br />
general (communal)<br />
85<br />
Toilet 82<br />
Domestic store 78<br />
General information 77<br />
Average Score 84<br />
The above table outlines the findings in relation to the environment of<br />
the facility inspected. The findings indicate that there are some areas<br />
for improvement. The findings in respect of the general environment,<br />
are detailed in the following sections.<br />
At the time of inspection major construction work was under way to<br />
create a new shared recovery bay, to service the endoscopy unit and<br />
theatres. The area had been screened off prior to taking down a wall<br />
however the screens had been removed once this work had finished.<br />
As a result the inspectors were concerned about the amount of dust<br />
that continued to permeate throughout the areas leading to the<br />
endoscopy unit<br />
6.1 Cleaning<br />
At the time of the inspection there was some evidence to indicate<br />
compliance with regional specifications for cleaning. However<br />
inspectors observed that greater attention to detail was required to<br />
ensure effective cleaning mechanisms were in place and implemented<br />
to prevent the build-up of dust and debris. This in turn prevents the<br />
build-up of bacteria and subsequently reduces the potential risk for the<br />
transmission of infection.<br />
10
The main hospital reception on the ground floor and the waiting area<br />
for the endoscopy unit were clean and in good decorative order.<br />
Greater attention to detail was required when cleaning the public toilets<br />
on the ground floor to remove splashes and stains from walls, skirting<br />
and the air vent. The inside of the toilet was stained and there was<br />
limescale on the taps. The toilets in the endoscopy unit also required<br />
further cleaning as the inside of both toilets and the vinyl covered back<br />
rest on the disabled toilet were stained.<br />
The walls in the domestic store were splashed and stained and there<br />
was debris on the floor under the low sluice sink. Both the sluice sink<br />
and equipment sink were dirty and the taps had limescale present.<br />
The hand touch points on the door were grubby and the shelving unit<br />
was dusty.<br />
6.2 Clutter<br />
The general areas were clutter free, two large x-ray machines were<br />
observed in the endoscopy waiting area, these were removed during<br />
the inspection.<br />
6.3 Maintenance and Repair<br />
This is a relatively new building and in good repair, however the<br />
inspectors did note that the vinyl flooring in the endoscopy unit was<br />
damaged in places. The flooring outside the endoscopy room has<br />
bubbled and some of the welds at the joins were missing or of poor<br />
finish and there were cracks to plaster work in the patient changing<br />
area.<br />
6.4 Fixtures and Fittings<br />
Unlike the rest of the unit the<br />
chairs in the patient changing<br />
area were old and worn, the<br />
vinyl covering was split and<br />
torn in places and therefore<br />
not impervious to moisture.<br />
6.5 Information<br />
Picture 1: Damaged vinyl on chair<br />
As the hospital has only been registered to the current owners some<br />
policies and guidelines are still being developed. A cleaning policy for<br />
11
nursing staff is in place but detailed cleaning schedules are being<br />
formulated. Similarly a support service manager has just been<br />
appointed and is currently re-drafting the domestic cleaning schedule<br />
which was very basic. Information leaflets on MRSA, Clostridium<br />
difficile and common infections were not available. Infection Prevention<br />
and Control policies are being developed for the hospital but staff have<br />
access to the Regional Infection Prevention and Control manual on<br />
line.<br />
Recommendations<br />
1. The hospital should ensure that the systems and processes<br />
in place for environmental cleaning, provide the necessary<br />
assurance that cleaning is carried out effectively, and that all<br />
staff are aware of their responsibilities.<br />
2. The healthcare environment should be repaired and<br />
maintained, and damaged furniture replaced to maintain<br />
public confidence and to help reduce the risk of the spread<br />
of infection.<br />
3. The hospital should review current storage arrangements to<br />
maintaining a clutter free environment.<br />
4. The hospital should continue on developing policies,<br />
guidelines and cleaning schedules.<br />
12
7.0 Patient Linen<br />
STANDARD 3.0<br />
PATIENT LINEN<br />
Storage of clean linen; handling and storage of used linen; ward/<br />
department laundry facilities.<br />
7.1 Management of Linen<br />
Patient Linen<br />
Storage of clean linen 90<br />
Storage of used linen 91<br />
Laundry facilities<br />
N/A<br />
Average Score 91<br />
Staff achieved an overall compliant score in this standard.<br />
The bed linen store was clean neat and tidy, however in the store used<br />
for staff scrubs the inspectors noted that some scrub suits were lying<br />
on the floor. In the clean decontamination room off the theatre, a<br />
supply of exposed clean sheets was observed on a trolley, these<br />
sheets should be stored covered or in a linen cupboard to prevent<br />
exposure to airborne contamination.<br />
The used linen baskets in the patient changing areas were made of<br />
wicker and therefore could not be effectively cleaned, and the cloth<br />
bags used as liners were ripped and damaged. Used linen awaiting<br />
collection was stored in a designated area and bags were not over<br />
filled.<br />
Staff advised inspectors that personal protective equipment (PPE) is<br />
used when handling soiled/contaminated linen and that theatre<br />
uniforms are reprocessed by a recognised external laundry contractor.<br />
Recommendations<br />
5. The hospital should ensure that clean linen is stored in a<br />
designated area which is fit for purpose.<br />
6. Equipment used for the storage of used linen should be<br />
cleanable and fit for purpose.<br />
13
8.0 Waste and Sharps<br />
STANDARD 4.0<br />
WASTE AND SHARPS<br />
Waste: Effectiveness of arrangements for handling, segregation,<br />
storage and disposal of waste on ward/department<br />
Sharps: Availability, use and storage of sharps containers on<br />
ward/department<br />
Waste and Sharps<br />
Handling, segregation,<br />
storage, waste<br />
Availability, use, storage<br />
of sharps<br />
86<br />
67<br />
8.1 Waste<br />
Although this standard was compliant, several issues were identified<br />
which need to be addressed. Waste was not disposed of appropriately<br />
in accordance with the hospitals waste policy, paper waste was<br />
observed in the sharps box in the endoscopy theatre and<br />
household waste bags were in the large clinical waste euro bins in the<br />
outside compound. The inside of the clinical waste euro bins were dirty<br />
and had loose waste, one of the clinical waste bins was over filled and<br />
the lid could not be locked.<br />
In the endoscopy reception area there was no household waste bin<br />
only a clinical waste bin, the clinical waste bin in the theatre had a<br />
paper label secured with tape and the clinical waste bin in the dirty<br />
utility room had a black household waste liner.<br />
8.2 Sharps<br />
This standard was minimally compliant and improvement is required in<br />
the following areas to ensure safe practice.<br />
The temporary closure mechanism on sharps boxes was not in use,<br />
the sharps box in the theatre had blood splatters and the sharps box on<br />
the dressing trolley was not secured. Not all sharps boxes within the<br />
unit were signed and dated and the inspectors noted this was also the<br />
same for sharps bins which had been disposed of into the large outside<br />
clinical waste euro bin.<br />
Recommendations<br />
7. The hospital should monitor the implementation of its<br />
policies and procedures in respect of the management of<br />
14
waste and sharps to ensure safe and appropriate practice is<br />
in place.<br />
8. The hospital should ensure waste bins and sharps boxes are<br />
clean.<br />
9. Systems and processes should be in place to assure that<br />
staff practice is correct in respect of the correct disposal of<br />
waste.<br />
15
9.0 Patient Equipment<br />
STANDARD 5.0<br />
PATIENT EQUIPMENT<br />
Cleanliness and state of repair of general patient equipment.<br />
Patient Equipment<br />
Patient equipment 87<br />
The unit achieved compliance in this standard however with attention to<br />
detail and the implementation and monitoring of the nursing cleaning<br />
schedule for patient equipment this score could be improved.<br />
In the endoscope theatre<br />
inspectors observed that<br />
ventilator equipment, oxygen<br />
pipes on the anaesthetic<br />
machine and notes trolley<br />
were dusty and stained. Staff<br />
dealt with these cleaning<br />
issues immediately.<br />
Picture 2: Stained framework of ventilator<br />
The inside of the doors of the dressing procedure trolley were stained<br />
and the top surface was dusty. Tourniquets were made of material and<br />
could not be effectively cleaned, and in the dirty utility room a 50ml<br />
flushing syringe had been removed from it packaging and left on the<br />
side of the double, scope cleaning sink.<br />
Recommendations<br />
10. The hospital and individual staff have a collective<br />
responsibility to ensure that general and specialist<br />
equipment is clean.<br />
11. Staff should ensure sterile equipment is not removed from its<br />
packaging prior to use.<br />
16
10.0 Hygiene Factors<br />
STANDARD 6.0<br />
HYGIENE FACTORS<br />
Hand wash facilities; alcohol hand rub; availability of PPE;<br />
availability of cleaning equipment and materials.<br />
Hygiene Factors<br />
Availability and<br />
cleanliness of wash hand 96<br />
basin and consumables<br />
Availability of alcohol rub 92<br />
Availability of PPE 82<br />
Materials and equipment<br />
for cleaning<br />
81<br />
Average Score 88<br />
In this standard overall compliance was achieved.<br />
Alcohol hand rub was generally available, however the portable alcohol<br />
dispenser and holder in the endoscope theatre room was dirty, dusty<br />
and empty.<br />
The section on the availability of personal protective equipment was<br />
partially compliant. Gauntlet sleeves were worn by staff when<br />
manually cleaning the endoscopes, however these were not effective<br />
as they continually slid down exposing the arm.<br />
Different colour single used aprons for clean and dirty work were not<br />
available and a box of vinyl gloves were observed on the shelf in the<br />
endoscope theatre. The Infection Prevention Society advise that these<br />
are used during low risk procedures. It is advised that the type of glove<br />
used is reviewed to ensure staff are use the correct gloves with the<br />
correct protection for all care activities.<br />
Face or eye protection was not worn consistently for the manual<br />
cleaning procedure, reusable goggles were available but stained. Hats<br />
and head gear were not available for use in the endoscope area.<br />
The section on cleaning materials and equipment was also partially<br />
compliant. On inspection of the domestic store, wooden mop handles<br />
and a wooden deck scrubber were noted, the mop buckets were dirty<br />
and water buckets were not colour coded. Not all buckets were<br />
inverted or dry. Equipment such as wet pickup mops, floor polishers<br />
and the domestic trolley were dusty.<br />
17
Recommendations<br />
12. The hospital should ensure hand washing facilities are clean<br />
and accessible.<br />
13. The hospital should ensure alcohol rub dispensers and filled<br />
and clean.<br />
14. The hospital should ensure PPE is available, fit for purpose<br />
and worn by staff.<br />
15. The hospital should ensure equipment for general cleaning is<br />
clean and fit for purpose.<br />
18
11.0 Hygiene Practices<br />
STANDARD 7.0<br />
HYGIENE PRACTICES<br />
Hand hygiene procedures; handling and disposal of sharps; use<br />
of PPE; use of isolation facilities and implementation of infection<br />
control procedures; cleaning of ward/department; staff uniform<br />
and work wear.<br />
Hygiene Practices<br />
Effective hand hygiene<br />
procedures<br />
67<br />
Safe handling and<br />
disposal of sharps<br />
100<br />
Effective use of PPE 83<br />
Correct use of isolation N/A<br />
Effective cleaning of the<br />
facility<br />
82<br />
Staff uniform and work<br />
wear<br />
97<br />
Average Score 86<br />
In this standard overall compliance was achieved, the safe handling and<br />
disposal of sharps was fully compliant, however a minimally compliant score<br />
was achieved in effective hand hygiene procedures. Staff were observed<br />
entering the dirty utility room on several occasions but failed to use alcohol<br />
hand rub to decontaminate their hands. Staff were also observed not washing<br />
their hands before donning disposable gloves.<br />
Personal protective equipment, disposable gloves and aprons were worn<br />
where appropriate. Staff did not wear the appropriate head protection when in<br />
the endoscope unit, staff in the adjoining theatre were observed wearing their<br />
head protection continuously instead of as a single use item.<br />
Nursing staff when questioned, were not aware of NPSA guidelines for colour<br />
coding of cleaning equipment in relation to theatres.<br />
The information on dilution rates for cleaning and disinfection chemicals was<br />
displayed in the domestic store but was difficult to read, and when domestic<br />
staff were questioned they were they were unable to give the correct dilution<br />
rates for the cleaning agent or disinfectant in use in the hospital.<br />
A dress code policy is in place within the hospital and generally staff were<br />
compliant, however inspectors observed that a member of theatre staff was<br />
wearing hoop earrings.<br />
19
Recommendations<br />
16. The hospital and individual staff have a responsibility to<br />
ensure that hand hygiene is carried out in line with the seven<br />
step technique and that all PPE is used appropriately.<br />
17. The hospital and individual staff have a collective<br />
responsibility to ensure that staff knowledge is kept up to<br />
date with regard to the correct dilution rates for chemicals<br />
and colour coded equipment used for cleaning and<br />
decontamination of equipment and specialist patient<br />
equipment.<br />
18. Staff should comply with the hospitals dress code policy.<br />
<strong>20</strong>
12.0 Endoscopy Suite<br />
STANDARD 8.0<br />
ENDOSCOPY SUITE<br />
Endoscopy Suite: anaesthetic room, scrub room, endoscopy<br />
theatre/room, endoscopy decontamination room/area, specialist<br />
equipment and policies/procedures.<br />
12.1 Endoscopy Suite Environment<br />
Endoscopy Suite<br />
Scrub Room<br />
N/A<br />
Endoscopy Theatre 97<br />
Endoscopy<br />
60<br />
decontamination room<br />
Specialist<br />
90<br />
Equipment/practices<br />
Policies and Procedures 93<br />
Average Score 85<br />
The endoscopy unit is a separate area located at one end of the<br />
hospital and accessed by a dedicated stairway or lift which leads to the<br />
first floor unit.<br />
In the endoscope theatre, inspectors observed a blood stain and paper<br />
labels attached to the theatre trolley. The scrub sink is located within<br />
the theatre space, the sink was clean and in good state of repair. The<br />
clean decontamination room is located off the theatre and can only be<br />
accessed through the theatre.<br />
In the clean decontamination room the top of the endoscope storage<br />
unit was dusty and the shelves were cluttered, stained and dusty.<br />
Adhesive tape had been used to secure labels to the drawers of the<br />
dressing trolley, adhesive tape cannot be effectively cleaned and<br />
alternatives should be sourced.<br />
A new drying cabinet had been<br />
installed in the clean<br />
decontamination room was in<br />
the process of being<br />
commissioned.<br />
Picture 3: New drying cabinet<br />
21
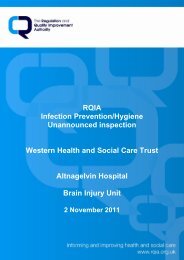
Picture 4: Blocked access to and washing sink<br />
The dirty decontamination<br />
area, was cluttered and dust<br />
was again an issue, there<br />
was dust on the top of the<br />
endoscope cabinet, air vents,<br />
storage units and skirting.<br />
Access to the hand wash<br />
sink was obstructed by<br />
boxes, the sink also required<br />
cleaning.<br />
There were stains on the<br />
front of the drying cabinet,<br />
adjoining door and the floor.<br />
The low sluice sink was dirty,<br />
and was being used as a<br />
work surface, inspectors<br />
noted that the central wheel<br />
from the endoscope washer<br />
disinfector stored on top of it.<br />
Picture 5: Sluice sink used as storage surface<br />
The double deep sink used to manually clean the scopes was stained<br />
and had signs of rust, and a dirty measuring jug was sitting on the edge<br />
of the sink unit. The double sink in the dirty decontamination room was<br />
not set at the correct high to minimise back injury. There was limescale<br />
deposits on the taps.<br />
The ventilation in the decontamination room did not appear to be<br />
working.<br />
Both the clean and dirty decontamination areas were cluttered with<br />
boxes and plastic bags sitting on the floor. In the dirty decontamination<br />
area the scope storage area was cramped and there was insufficient<br />
work area.<br />
The recovery room was not inspected as it was in constant use<br />
throughout the inspection.<br />
New guidance CFPP 01-06 is to be issued in the near future, all<br />
endoscope decontamination facilities in Northern Ireland will be<br />
required to meet "best practice" requirements of this document in<br />
relation to layout, quality systems and environmental requirements.<br />
22
12.1 Specialist Patient Equipment<br />
In the clean decontamination room the storage trolley for the<br />
endoscopes was dusty. In the dirty decontamination room, the second<br />
sink used in the double sink manual cleaning process of the scopes did<br />
not have a fill line.<br />
In relation to effective cleaning, the HEIG inspectors noted that in the<br />
manual wash area the unit dispensing detergent was faulty and an<br />
incorrect ratio of detergent to water was being used. Detergents<br />
should be diluted as per the manufactures guidelines to be effective.<br />
12.2 Policies Procedures and Training<br />
This is a new open facility and while some policies, for example the<br />
decontamination of endoscopy equipment and stand operational<br />
procedures are in place. Others such as, procedures for regular audits<br />
and the hospitals own infection prevention and control policy have still<br />
to receive approval. Staff currently use the Regional Infection<br />
Prevention and Control guidance on line. A training and validation<br />
programme has just been put in place.<br />
Recommendations<br />
19. The environment of the endoscopy suite should be clean and<br />
free of clutter.<br />
<strong>20</strong>. The decontamination room should be fit for purpose and<br />
comply with relevant standards.<br />
21. Improvements required in the decontamination process<br />
should be addressed and work commenced to comply with<br />
CFPP.<br />
22. All recommendations as outlined by the HEIG inspectors in<br />
their key findings report should be addressed.<br />
23
13.0 Key Personnel and Information<br />
Members of the RQIA inspection team<br />
Mrs S O'Connor<br />
Mrs M Keating<br />
Mr C Muldoon<br />
- Inspector Infection Prevention/Hygiene Team<br />
- Inspector Infection Prevention/Hygiene Team<br />
- Inspector Estates Team<br />
Members of the DHSSPS Health Estates Investment Group (HEIG)<br />
inspection team<br />
Mr David Pollock - Inspector, Health Estates Investment Group<br />
Mr Eddie Clarke - Inspector, Health Estates Investment Group<br />
<strong>Hospital</strong> representatives attending the feedback session<br />
The key findings of the inspection were outlined to the following trust<br />
representatives:<br />
Ms R Wilson - Governance Manager<br />
Mr R Mackinnon - Facilities Manager<br />
Ms Zana O’Neill - GON Cleaning Contractor<br />
Mr P Monaghan - GON Cleaning Contractor<br />
Supporting documentation<br />
A number of documents have been developed to support the inspection<br />
process, these are:<br />
• Infection Prevention/Hygiene Inspection Process (methodology,<br />
follow up and reporting)<br />
• Infection Prevention/Hygiene Team Inspection Protocol (this<br />
document contains details on how inspections are carried out and<br />
the composition of the teams)<br />
• Infection Prevention/Hygiene Team Escalation Policy<br />
• RQIA Policy and Procedure for Use and Storage of Digital Images<br />
This information is currently available on request and will be available<br />
in due course on the RQIA website.<br />
24
14.0 Summary of Recommendations<br />
1. The hospital should ensure that the systems and processes<br />
in place for environmental cleaning, provide the necessary<br />
assurance that cleaning is carried out effectively, and that all<br />
staff are aware of their responsibilities.<br />
2. The healthcare environment should be repaired and<br />
maintained, and damaged furniture replaced to maintain<br />
public confidence and to help reduce the risk of the spread of<br />
infection.<br />
3. The hospital should review current storage arrangements to<br />
maintaining a clutter free environment.<br />
4. The hospital should continue on developing policies,<br />
guidelines and cleaning schedules.<br />
5. The hospital should ensure that clean linen is stored in a<br />
designated area which is fit for purpose.<br />
6. Equipment used for the storage of used linen should be<br />
cleanable and fit for purpose.<br />
7. The hospital should monitor the implementation of its<br />
policies and procedures in respect of the management of<br />
waste and sharps to ensure safe and appropriate practice is<br />
in place.<br />
8. The hospital should ensure waste bins and sharps boxes are<br />
clean.<br />
9. Systems and processes should be in place to assure that<br />
staff practice is correct in respect of the correct disposal of<br />
waste.<br />
10. The hospital and individual staff have a collective<br />
responsibility to ensure that general and specialist<br />
equipment is clean.<br />
11. Staff should ensure sterile equipment is not removed from its<br />
packaging prior to use.<br />
12. The hospital should ensure hand washing facilities are clean<br />
and accessible.<br />
13. The hospital should ensure alcohol rub dispensers and filled<br />
and clean.<br />
25
14. The hospital should ensure PPE is available, fit for purpose<br />
and worn by staff.<br />
15. The hospital should ensure equipment for general cleaning is<br />
clean and fit for purpose.<br />
16. The hospital and individual staff have a responsibility to<br />
ensure that hand hygiene is carried out in line with the seven<br />
step technique and that all PPE is used appropriately.<br />
17. The hospital and individual staff have a collective<br />
responsibility to ensure that staff knowledge is kept up to<br />
date with regard to the correct dilution rates for chemicals<br />
and colour coded equipment used for cleaning and<br />
decontamination of equipment and specialist patient<br />
equipment.<br />
18. Staff should comply with the hospitals dress code policy.<br />
19. The environment of the endoscopy suite should be clean and<br />
free of clutter.<br />
<strong>20</strong>. The decontamination room should be fit for purpose and<br />
comply with relevant standards.<br />
21. Improvements required in the decontamination process<br />
should be addressed and work commenced to comply with<br />
CFPP.<br />
22. All recommendations as outlined by the HEIG inspectors in<br />
their key findings report should be addressed.<br />
26
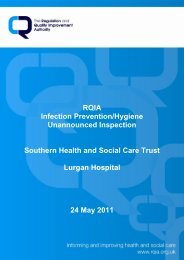
15.0 Escalation Process<br />
RQIA Hygiene Team: Escalation Process<br />
B<br />
RQIA IPH<br />
Team<br />
Escalation<br />
Process<br />
Concern / Allegation / Disclosure<br />
Inform Team Leader / Head of Programme<br />
MINOR/MODERATE<br />
Has the risk been<br />
assessed as Minor,<br />
Moderate or Major?<br />
MAJOR<br />
Inform key contact and keep a record<br />
Inform appropriate RQIA Director and Chief Executive<br />
Record in final report<br />
Inform Trust / Establishment / Agency<br />
and request action plan<br />
Notify Chairperson and<br />
Board Members<br />
Inform other establishments as appropriate:<br />
E.g.: DHSSPS, RRT, HSC Board, PHA,<br />
Seek assurance on implementation of actions<br />
Take necessary action:<br />
E.g.: Follow-Up Inspection<br />
27
16.0 Action Plan<br />
Reference<br />
number<br />
Recommendations<br />
1. The hospital should ensure that the systems and<br />
processes in place for environmental cleaning, provide<br />
the necessary assurance that cleaning is carried out<br />
effectively, and that all staff are aware of their<br />
responsibilities.<br />
Designated<br />
department<br />
Action required<br />
Date for<br />
completion/<br />
timescale<br />
2. The healthcare environment should be repaired and<br />
maintained, and damaged furniture replaced to<br />
maintain public confidence and to help reduce the risk<br />
of the spread of infection.<br />
3. The hospital should review current storage<br />
arrangements to maintaining a clutter free<br />
environment.<br />
4. The hospital should continue on developing policies,<br />
guidelines and cleaning schedules.<br />
5. The hospital should ensure that clean linen is stored in<br />
a designated area which is fit for purpose.<br />
6. Equipment used for the storage of used linen should<br />
be cleanable and fit for purpose.<br />
7. The hospital should monitor the implementation of its<br />
policies and procedures in respect of the management<br />
of waste and sharps to ensure safe and appropriate<br />
practice is in place.<br />
28
Reference<br />
number<br />
Recommendations<br />
8. The hospital should ensure waste bins and sharps<br />
boxes are clean.<br />
Designated<br />
department<br />
Action required<br />
Date for<br />
completion/<br />
timescale<br />
9. Systems and processes should be in place to assure<br />
that staff practice is correct in respect of the correct<br />
disposal of waste.<br />
10. The hospital and individual staff have a collective<br />
responsibility to ensure that general and specialist<br />
equipment is clean.<br />
11. Staff should ensure sterile equipment is not removed<br />
from its packaging prior to use.<br />
12. The hospital should ensure hand washing facilities are<br />
clean and accessible.<br />
13. The hospital should ensure alcohol rub dispensers<br />
and filled and clean.<br />
14. The hospital should ensure PPE is available, fit for<br />
purpose and worn by staff.<br />
15. The hospital should ensure equipment for general<br />
cleaning is clean and fit for purpose.<br />
16. The hospital and individual staff have a responsibility<br />
to ensure that hand hygiene is carried out in line with<br />
the seven step technique and that all PPE is used<br />
appropriately.<br />
29
Reference<br />
number<br />
Recommendations<br />
17. The hospital and individual staff have a collective<br />
responsibility to ensure that staff knowledge is kept up<br />
to date with regard to the correct dilution rates for<br />
chemicals and colour coded equipment used for<br />
cleaning and decontamination of equipment and<br />
specialist patient equipment.<br />
Designated<br />
department<br />
Action required<br />
Date for<br />
completion/<br />
timescale<br />
18. Staff should comply with the hospitals dress code<br />
policy.<br />
19. The environment of the endoscopy suite should be<br />
clean and free of clutter.<br />
<strong>20</strong>. The decontamination room should be fit for purpose<br />
and comply with relevant standards.<br />
21. Improvements required in the decontamination<br />
process should be addressed and work commenced<br />
to comply with CFPP.<br />
22. All recommendations as outlined by the HEIG<br />
inspectors in their key findings report should be<br />
addressed.<br />
30